 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 4, December, 2009, pp. 284-289 Case Reports Mesenteric venous thrombosis in Uganda: a retrospective study of five cases *Galukande M1, Fualal J2, Nyangoma E1 1- Department of Surgery, School of Medicine, College of Health Sciences, Makerere University Code Number: hs09067 Abstract Introduction: Mesenteric venous thrombosis is a rare but lethal form of mesenteric ischemia. Diagnosis before
frank thrombosis and gangrene is a challenge. Documented experience in the East African region is scanty. This short
series suggest renal dysfunction as a consequence of delayed diagnosis, intussusception as a differential and highlights
the challenges of management with limited investigative capacity.
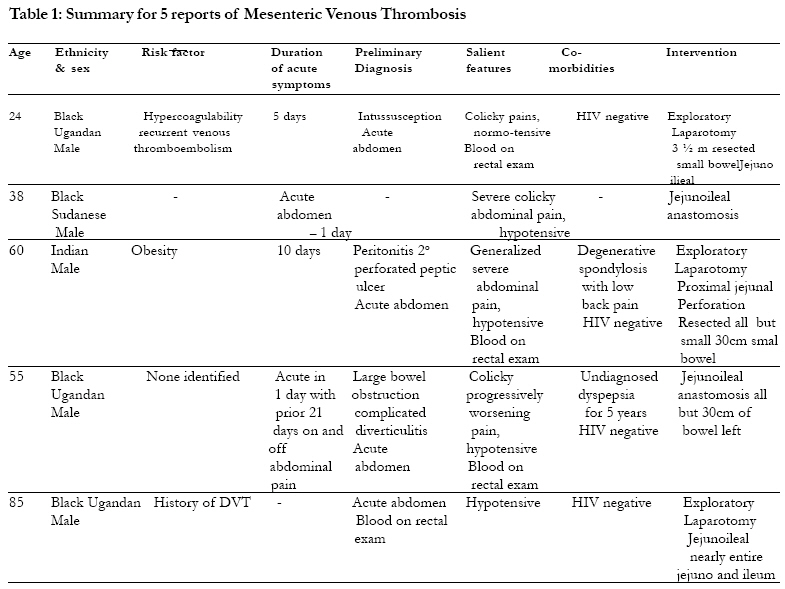
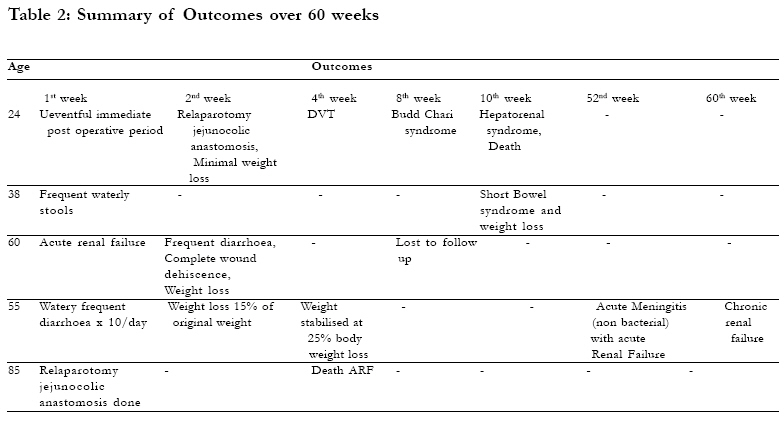
Introduction Mesenteric venous thrombosis is a rare but lethal form of mesenteric ischemia. Mesenteric venous thrombosis as a cause of mesenteric ischemia was described a century ago. Lately, many review articles and texts describe the recent advances in the understanding and management of mesenteric ischemia, particularly venous thrombosis1,2,3,4. Intestinal infarction as a result of ischemia due to venous thrombosis is reported to have a mortality rate of up to 34% after resection. Not much literature is available about this condition in the regional context of Eastern Africa This paper therefore describes the presentation of five patients with mesenteric venous thrombosis in two Kampala hospitals. Methods Descriptive Retrospective review of five mesenteric venous thrombosis patients diagnosed at laparotomy over a 48 months period in two Kampala Hospitals by two surgeons. Patient data were files reviewed and manually analyzed, according to a set of parameters, demographics (age, sex and ethnicity), risk factors, co morbidities, clinical presentation and outcomes. Results Five patients were reported on over a 2-year period. One was lost to follow up, two died within the first 10 weeks the fourth had adult malnutrition features and end stage chronic renal failure at the 60-week point (time of writing). The fifth had signs of adult malnutrition from short bowel syndrome. The tables below summaries the salient points in this five report series. Discussion Risk factors The risk of acute mesenteric venous thrombosis increases in patients with hypercoagulable states (e.g. polycythemia vera, protein C and S deficiencies), visceral infection (intra abdominal sepsis) 4, 5, portal hypertension, perforated viscus, blunt abdominal trauma, malignancy, previous abdominal surgery (open or laparoscopic), or pancreatitis and in patients who smoke6, 7, 8. Women taking oral contraceptives are also at increased risk of venous thrombosis9 Patients who have undergone Splenectomy, colectomy, and Roux-Y gastric bypass are at increased risk of subsequent portal venous thrombosis, which rarely results in bowel infarction. No underlying cause is found in 25-50% of patients diagnosed with mesenteric venous thrombosis. In this small number series hypercoagulability was noted in one patient and a past history of DVT in another. For the other three no identifiable risks were found. All the five were male. Pathophysiology While the mesenteric arterial system may carry 25-40% of the cardiac output at one time, the venous system typically carries 30%. The mechanism that causes ischemia is a massive influx of fluid into the bowel wall and lumen, resulting in systemic hypovolemia and hemoconcentration. All the patients in this series required Intravenous resuscitation with large amounts of crystalloids. Resulting bowel edema and decreased outflow of blood secondary to venous thrombosis impede the inflow of arterial blood, which leads to bowel ischemia. While bowel ischemia is detrimental to the patient, the resulting multiple organ system failure actually accounts for the increased mortality rate. The renal failure seen in two of these patients in a function of volume loss a consequence of bowel Ischaemia and gangrene. The venous system, for the most part, parallels the arterial system. The superior mesenteric vein (SMV) is formed by the jejunal, ileal, ileocolic, right colic, and middle colic veins, which drain the small intestine, caecum, ascending colon, and transverse colon. The right gastroepiploic vein drains the stomach to the SMV, while the inferior pancreaticoduodenal vein drains the pancreas and duodenum. The inferior mesenteric vein drains the descending colon, the sigmoid colon, and the rectum through the left colic vein, the sigmoid branches, and the superior rectal vein, respectively. The inferior mesenteric vein joins the splenic vein, which then joins the SMV to form the portal vein, which enters the liver. Clinical presentation It may present in any of the three forms: acute, subacute and chronic 10 Patients with mesenteric venous thrombosis have an insidious onset of symptoms described as vague abdominal discomfort that typically evolve over 7-10 days. The presentation of the patients in this report is consistent with this duration. Patients may have a condition that predisposes them to a hypercoagulable state, which may be elicited by taking a thorough history. Cancer, polycythemia vera, or a history of deep vein thrombosis or pulmonary embolus are important risk factors that should be elicited from the history. The 24 year old in this paper had a history of recurrent venous thrombosis embolism (Thrombophilia) with hypercoagulability though the exact cause of this was never established. Patients presenting with pancreatitis or signs of intra-abdominal infection should be considered predisposed to developing mesenteric venous thrombosis. Patients may have a distended abdomen and guaiac-positive stool samples. If the patient has an underlying intra-abdominal infection, peritoneal signs may be elicited and a palpable abdominal mass may be felt. As with acute mesenteric ischemia, patients may report pain disproportionate to that normally elicited during a physical examination, which presentation mimics acute pancreatitis. What was consistent in this series is they all presented as emergencies with an acute abdomen and all had intestinal infarct and needed emergency laparotomy. The challenges here lies in early diagnosis would it have been impossible to make the diagnosis before the catastrophic events they presented with? For the patients in this series, in only one did we entertain the diagnosis before Surgery. The points that raised the suspicion were the history of DVT in the past and the acute abdomen picture that wasn't fitting in the typical commoner causes of acute abdomens in our environment. The other consistent finding was blood on the rectal examination, which normally would point to intussusceptions or a severe infective process and rarely ulcerative colitis in our environment. Diagnosis and Investigations4, 11, 12, 13 14 As part of clinical assessment, paracentesis may demonstrate bloody peritoneal fluid; however, this occurs after bowel infarction and, therefore, is a late sign. By this time the clinical presentation would have warranted an emergency laparotomy, so this paracentesis may be of limited value. Unfortunately, laboratory examinations are not of much help for confirming the diagnosis of venous thrombosis. Laboratory studies help more to suggest, rather than exclude, the diagnosis. Requisite laboratory studies include a coagulation profile: prothrombin time (PT) activated partial thromboplastin time (aPTT), CBC count (which may reveal leukocytosis and/or hemoconcentration), and chemistries (which may show metabolic acidosis). Leukocytosis and acidosis are the more specific laboratory findings in patients with ischemia. Unfortunately, they are late findings. Evaluating patients for protein C and S deficiencies; antithrombin III deficiency; and abnormalities in lupus anticoagulant, anticardiolipin antibody, and platelet aggregation would be possible if the diagnosis is made pre operatively. Besides these are not routinely available to us in resource limited environments. CT scanning is considered to be the diagnostic tests of choice in patients stable enough for it. A CT scan of the abdomen may show an enlarged mesenteric or portal vein with sharp definition of the venous wall and low density within the vein. An arteriogram where available may show vasospasm, contrast in the bowel lumen, non-visualized venous system, reflux of contrast into the aorta. In an emergency low resourced setting a CT scan for every patient with an acute abdomen is an unlikely course of action, however, a plain erect abdominal x-ray is mostly available all the time. However, plain x-ray films may show nonspecific findings such as dilated loops of bowel with air-fluid levels. Air in the portal system may also be observed on plain films, although this is rare. Blunt, semi opaque indentations of the bowel lumen (thumb printing are indicative of mucosal oedema, whereas gas in the bowel wall (pneumatosis intestinalis) as been described. A duplex scan of the mesenteric vessels is beneficial only if used early and of course if the diagnosis was entertained when the patient first presented. There will be absent flow to necrotic bowel areas. When hemoconcentration is found the clinician will think of dehydration, on that the possibility of MVT should always be considered. MRI is also very sensitive, but because of cost and the time required for the examination, it is not as practical as CT scanning. CT angiography and gadolinium-enhanced magnetic resonance angiography enable volumetric acquisitions with the patient holding only a single breath, and they offer excellent diagnostic capabilities for patients with venous thrombosis, again these are only available in well-resourced settings. Despite all of these diagnostic indicators, the diagnosis of venous thrombosis is usually confirmed during laparotomy or autopsy. Medical management The goals of the initial treatment of venous thrombosis are defining the underlying cause of the patient's hypercoagulable state and treating it appropriately. This presupposes that the diagnosis is made. Patients with polycythemia should undergo phlebotomy, while those with clotting abnormalities should receive anticoagulation therapy with low molecular weight heparin. After achieving appropriate anticoagulation, patients should stay on long-term warfarin and subsequent follow up with regular INR measurements. The 24 year old was on long term anti coagulants and followed up in a haematology clinic. Lytic therapy with urokinase, streptokinase, or tissue plasminogen activator has been found to be beneficial in some cases. Mechanical transhepatic thrombectomy has recently been described 15, 16. What about low dose Aspirin? Postoperative care includes close monitoring of blood pressure and hemoglobin parameters to evaluate for sepsis or hemorrhage. Studies have shown that 60% of cases of rethrombosis of the mesenteric vein occur at the site of re-anastomosis, probably because of local thrombotic factors. This finding demonstrates the importance of maintaining the patient on postoperative heparin therapy. Unlike patients with arterial ischemia, patients with venous thrombosis do not require a second-look laparotomy unless progression of the disease is possible, which typically occurs in 40% of patients. Because of the high incidence of concomitant vascular disease, patients require close monitoring. Surgical treatment Nasogastric decompression, fluid resuscitation to correct any acid base abnormalities and bowel rest, should be instituted at the onset. Anticoagulation therapy with intravenous heparin should be continued intraoperatively. Indications for surgery in patients with acute mesenteric venous thrombosis include signs of peritonitis, possible bowel infarction, and hemodynamic instability. Resection and anastomose is the likely procedure.Because of the massive amount of blood lost from the circulatory system to the bowel, patients may require blood transfusions without hesitation. Therefore, type and cross match at least 4 units of packed red blood cells before surgery. Start all patients on broad-spectrum antibiotic therapy before the operation. Direct venous surgery to remove the clot is usually unsuccessful and is best reserved for patients with portal or superior mesenteric vein involvement. Because patients become acutely hypovolemic, acute renal failure may occur. Keeping the patient well hydrated and administering mannitol before the aorta is cross-clamped can prevent acute renal failure. All the patients in this series developed Acute Renal failure. Is it a function of hypovolemia or a sequel of MVT? Reports of diagnostic laparoscopy 17 in patients with venous thrombosis suggest this modality may have some use in preventing fruitless Laparotomies in these patients; however, the decreased mesenteric blood flow that occurs with laparoscopy may worsen bowel ischemia, therefore making it improbable choice once diagnosis is considered. Patients with severe intestinal loss due to mesenteric venous thrombosis may be considered for intestinal transplantation but only in specialized centers. A second-look laparotomy is a reasonable strategy especially in patients with significant bowel involvement, to minimize the amount of bowel loss. At the first laparotomy as little as possible should be resected, a benefit of doubt given to borderline looking bowel. A second look 24-48 hours later helps confirm viability and necessity of further resection18. Two of the patients reported here had second look laparotomies. Where available, one gram of intravenous fluorescein followed by bowel examination under Wood lamp illumination can delineate poorly perfused bowel. Intraoperative Doppler studies are not as effective as fluorescein studies in determining venous thrombosis. Prognosis Acute venous thrombosis has a 30% mortality rate with a 25% recurrence rate without anticoagulant therapy19. Anticoagulant therapy combined with surgery is associated with the lowest recurrence rate (~3-5%). Patients presenting with peritonitis and infarcted bowel have a prolonged and complicated course 20. Of all etiologies of mesenteric ischemia, venous thrombosis carries the best prognosis. Survival has improved over the last four decades in literature from the developed world, no sufficient information in sub-Saharan Africa to make that judgment. Mesenteric venous thrombosis is an insidious disease with a high mortality rate typically attributed to the long delay in diagnosis. Patients with this condition benefit from rapid diagnosis and expedient surgical therapy. Those that survive the initial assault are confronted with the challenges of short bowel syndrome and the malnutrition that goes with it21. In these patients, dietary changes, vitamin supplements and codeine were used to reduce on the frequency and consistence of the motions they had. Conclusion The biggest challenge of management of MVT is early diagnosis. The clinician should always consider MVT when the typical picture of the considered diagnosis is not clear-cut and in the presence of any hint of hypercoagulability. Blood on rectal examination showed in these reports is clearly a late sign. Whereas it gets one to think intussusception or dysentery, MVT should be included on the list of possibilities. This would possibly contribute to reduction in mortality. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09067t1.jpg] [hs09067t2.jpg] |
| |||||||||

{kind=link}
{kind=link}