 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 9, No. 4, December, 2009, pp. 290-293 Survival in primary a plastic anaemia; experience with 20 cases from a tertiary hospital in Nigeria *Arewa OP, Akinola NO Department of Haematology & Blood Transfusion, Obafemi Awolowo University Teaching Hospital Ile-Ife, Osun State. Code Number: hs09068 Abstract Background: Aplastic anaemia is a condition characterized by pancytopenia and unexplained bone marrow
hypocellularity. Without treatment, it is invariably fatal. However with the currently available treatment options, patient survival is
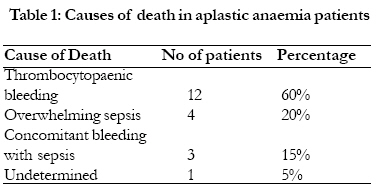
improving in the developed countries. Keywords: Aplastic anaemia; survival, Nigeria. Running title: Survival in aplastic anaemia in Nigeria. Introduction Aplastic anaemia (AA), a haematological disorder resulting from the failure of haemopoiesis and characterized by pancytopaenia and a hypocellular marrow in the absence of foreign cells, may result from several etiopathogenetic mechanisms. Aplastic anaemia could be acquired or inherited. Environmental triggers include drugs, viruses and toxins; however the most common is idiopathic or primary aplastic anaemia1. The incidence of aplastic anemia shows geographical variability. It is lower in Europe, North America and Brazil, and higher in Asia2. This variability in incidence rates may reflect differences in exposure to environmental factors including viruses, drugs and chemicals, genetic background, diagnostic criteria, and study designs. In Africa, there is paucity of literature on epidemiological studies reporting population based incidence of aplastic anaemia. Aplastic anaemia patients generally have varied clinical courses; while some patients have may have mild symptoms with a stable clinical course that necessitate little or no therapy (stable aplastic anaemia; SAA), others present with life-threatening pancytopenia; a haematological emergency. The outcome of patients with severe aplastic anemia is not only influenced by patients' variables such as severity of the disease and age, but also by the choice of the initial treatment.3 The case fatality rate of severe aplastic anemia is high although treatment, whether by allogeneic stem-cell transplantation or immunosuppression, has dramatically improved the prognosis over the last 25 years, and more than 75% of patients can now be expected to have long term survival with either therapy.2 However the benefit of bone marrow/stem cell transplantation and immunosuppressive drug therapy with antithymocyte globulin and cyclosporine is not readily accessible to Nigerians with aplastic anaemia. In a 1992 study to review cases of aplastic anaemia seen at the University College Ibadan, Nigeria over a 20 year period, Aken'Ova et al, 4 observed that the high mortality reported within one year of presentation was due to late presentation and inadequate supportive care. This present study highlights the challenges of management of patients with aplastic anaemia in another centre, Obafemi Awolowo University Teaching Hospital Ile-Ife, a tertiary level of care in Osun State Nigeria. Materials and Methods Case records of twenty five patients with established diagnosis of primary aplastic anaemia over a period of fifteen years were reviewed. Patients on cancer chemotherapy, radiation therapy and hypersplenism as well as lymphomas with bone marrow involvement were excluded from the study. Information extracted for each patient included age, sex, date of diagnosis, haematologic parameters at diagnosis (White blood cell count, Haematocrit, Platelet count), date of death or date lost to follow up. The severity of aplastic anemia was defined according to the widely accepted criteria described by Camitta et al.5 Severe disease was defined as the presence in two of three blood counts of an absolute neutrophil count <0.5×109/L, platelet count <20×109/L, and reticulocytes <1%. Extreme neutropenia (absolute neutrophil count <0.2×109/L) defined very severe aplastic anemia. All other cases were defined as moderate. Duration of survival is taken as the interval between the date of diagnosis and death or date patient was last seen on follow up. Analysis was done using the Microsoft Excel software (2003). Survival analysis included only patients diagnosed up to December 2004. One of the limitations of our study is that we obtained the follow-up information from clinical records. As a result, the last date of follow up for some of the patients was assumed to be a fair estimation of the last date of survival. Results A total of twenty five patients were diagnosed with aplastic anaemia over a fifteen year period; giving an annual incidence of 1.6 cases per year. Twenty patients had complete analyzable data. The age range of the patients was between 12 to 58 years; (mean 28.7±15.6, median 22 years). The male female ratio was 1.3: 1. The mean (±SD) packed cell volume at diagnosis/haematocrit was 15±5%, white cell count; 3.0 x 109/L ± 1.7 x 109/L, Absolute neutrophil count (ANC); 0.67 x 109/L ± 0.4 x 109/L, and platelets; 25 x 109/L ± 22.9 x 109/L. Sixteen (80%) of the patients presented with severe aplastic anaemia at diagnosis. Management of the patients included transfusion support with fresh unbanked whole blood, packed red cells, platelet concentrate, partial platelet concentrates, antibiotics and high dose methyl-prednisolone. All patients were blood transfusion dependent. Adequate transfusion support was often limited by the non availability of multiple blood bags needed for component preparation as well as inadequacy of blood donors. The median survival from presentation/ diagnosis was 6.5 weeks. The longest surviving patient was followed up for 55 weeks. Late presentation was an important issue in the majority of cases seen. There is a positive correlation between survival and platelet count at diagnosis (r=0.53); furthermore, a younger age at diagnosis correlated positively with survival (r=0.52). No significant statistical difference was seen in relation to sex. None of the patients had the benefit of bone marrow transplantation or immunosuppressive therapy with cyclosporine and anti-thymocyte immunoglobulin. The major cause of death was thrombocytopaenic bleeding in 60% of the patients. 20% of the patients died from overwhelming sepsis and another 15% died from a combination of sepsis and thrombocytopaenic bleeding. The cause of death was undetermined in 1 case (5% of the patients; table 1). Discussion Aplastic anaemia is a relatively rare disease, characterized by the loss of haemopoietic stem cells in the bone marrow, exchanged with fat cells and pancytopenia in the peripheral circulation. The treatment of this disease essentially consists of supportive therapy with blood products and ultimately the definitive treatment, where there are two established possibilities: immunosuppression and bone marrow transplantation.1, 6 The benefits of each are comparable. However, certain subsets of patients derive superior benefit from one or the other. Bone marrow transplantation is the initial treatment of choice for young patients (<20 years old). 1 It results in the complete reconstitution of haematopoiesis, whereas autologous haematopoietic remissions after immunosuppressive therapy are more susceptible to relapse. Survival rates after marrow transplantation in patients between 20-40 years are comparable to those reported for immunosuppressive therapy. For patients older than 40 years, the treatment of choice is immunosuppressive therapy. 1 The standard regimen for immunosuppressive therapy is combination of antithymocyte globulin (ATG) and cyclosporine A (CSA); a systematic review and meta-analysis of all randomized controlled trials that compared ATG and CsA to ATG alone as first-line treatment for patients with severe and non severe aplastic anemia concluded that a combination of both drugs should be considered the gold standard only for patients with severe aplastic anemia.7 The age range of affected patients in this study shows that the young adult population is largely affected with a mean age of 28.7±15.6 years, median 22 years. This finding is somewhat similar to the first peak age incidence reported in some other studies. 2, 8-9 The reported studies were population based and essentially showed a bimodal peak age incidence; the first peak in the young adult age group and a second peak in the fifth to sixth decade. Montane et al,2 reported a bimodal peak age incidence at 15-24 years and greater than or equal to 65 years in Spain. In addition to the reported studies being population based studies as against the hospital based setting of the present study, the second peak of may be a reflection of a higher life expectancy in the populations studied (Spain, France and Thailand) as against Nigeria where the average life expectancy is much less at 50.1 years.10 There is no difference in the incidence of aplastic anaemia by sex in this study. This is also similar to findings from some earlier studies.2, 4 In comparism to other recent studies, the median survival of patients with aplastic anaemia in this series is abysmally short at six and half weeks. Patients with higher platelet count at diagnosis survived relatively longer than those with lower values. This is most likely due to a reduced risk of thrombocytopaenic bleeding in such patients. Bleeding complications as a result of low platelet count was the most common cause of death in this study. Management of thrombocytopaenic bleeding presents a special challenge in the absence of adequate platelet support services as red cell transfusion does not help and may indeed aggravate the situation and provoke further bleeding.11 This is because red cell diapedesis is accentuated in thrombocytopaenic states and microvascular capillary bleeding is thus worsened. Significantly, the management of aplastic anaemia in this series is suboptimal. Current survival rates where optimal management facilities and therapeutic options are available are significantly higher with reports of 70-90% five year survival12 and 51% at fifteen years.2 The non-availability of bone marrow/stem cell transplantation is a major contributory factor to the very short survival recorded in this study. Aken'Ova et al in a 1992 review identified non-availability of bone marrow transplant facility in Nigeria as an important factor contributing to the poor survival of aplastic anaemia patients in Nigeria. 4 Sadly, the situation has not improved to the point where such patients can now access improved care; if anything, the level of care has worsened. In an era where bone marrow transplantation is now considered as the definitive management modality for a number of haematologic disorders including aplastic anaemia, it is unfortunate that there is no single centre offering this treatment in a country with a population of over 140 million. As a country that accounts for about 50% of the West African economy, 13 the establishment of a bone marrow transplant centre which could offer the treatment to the population as well as possibly serve as a referral centre for patients in need of this care in the West African sub region is most appropriate. Many of the patients presented late in the course of the disease with 16 out of 20 (80%) of the patients presenting as severe aplastic anaemia at diagnosis. This could also be a contributory factor to the short survival. While immunosuppressive therapy is a relevant alternative to bone marrow/stem cell transplantation in the management of aplastic anaemia, potent relevant immunosuppressive drugs such as cyclosporine and antithymocyte globulin are not available. In addition to the very high cost of these drugs which is out of reach of the majority of the affected patients, the drugs are not generally available in the Country. Steroids such as prednisolone and durabolin are ineffective in achieving the desired effect but unfortunately in the absence of the potent immunosuppressive drugs, methyl prednisolone is used as an adjunct in the management of the patients in this series. The result, not unexpectedly is poor. Furthermore, there is inadequate transfusion support service for the supply of the much needed blood component (red cell and platelet concentrates) required for transfusing the patients as necessary. This is due to the near absence of a reliable voluntary blood donor base as well as inadequacy of supply of multiple blood bags required for component preparation thus making the availability of blood component irregular and inadequate. All the factors highlighted above contribute to short median survival of patients in this series. In conclusion, while there is evidence of improved survival in aplastic anaemia globally, the experience from this series shows that the story is different in Nigeria. There is a clear need for a policy that ensures the availability of proven therapeutic options for patients such bone marrow/stem cell transplantation and drugs (CSA and ATG) to improve on the situation. Acknowledgement The authors acknowledge the efforts of the Consultants, Resident doctors and Nurses in the Department of Haematology Obafemi Awolowo University Teaching Hospital Ile-Ife in caring for the patients. I also appreciate the assistance of the staff of the Medical records unit in retrieving the case record files of the patients. References
Copyright © 2009 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs09068t1.jpg] |
| |||||||||

{kind=link}