 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 14-17 Testicular and para-testicular tumors in south western Nigeria Salako A A1, *Onakpoya U U 1, Osasan SA2, Omoniyi-Esan G O2 1Department of Surgery, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Nigeria *Correspondence author: Dr Uvie Ufuoma Onakpoya, Department of Surgery, Obafemi Awolowo University Teaching Hospitals Complex, PMB 5538, Ile-Ife 22006, Osun state, Nigeria. E-mail: uvtoyin@yahoo.com Phone number: +2348037194945 Code Number: hs10004 Abstract Background: Tumors of the testis and paratesticular tissues are rare, especially in men of African descent. In recent
reviews however, the incidence is rising among the Caucasians and black Americans. We set out to determine the incidence in
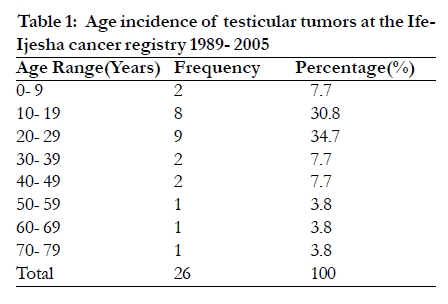
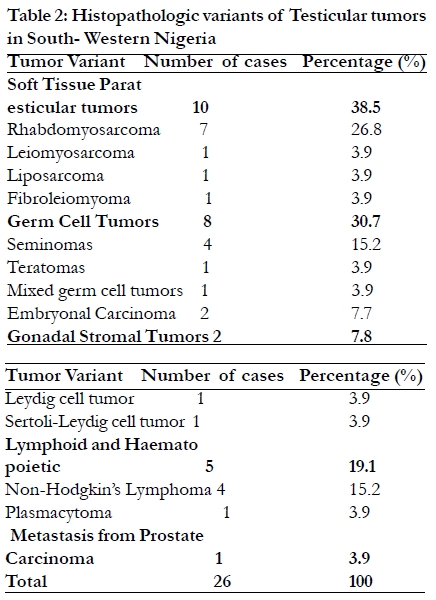
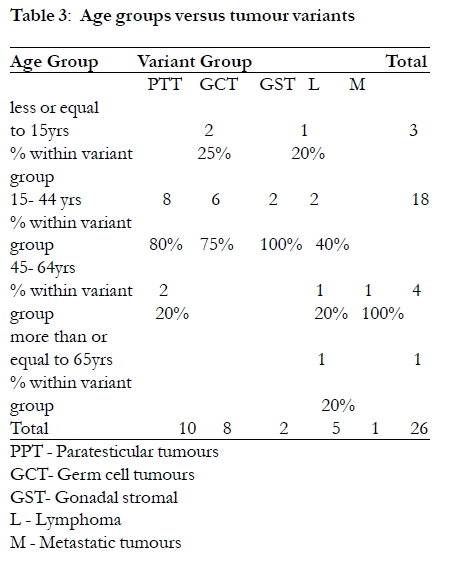
South-Western Nigeria and to examine the histopathologic variants. Key words: testis, tumors, Nigeria Introduction Tumors of the testis and para-testicular tissues are rare in men. However, they constitute the most common solid malignancies in men aged between 15 and 35 years 4, 5. With an incidence of 0.5 2% of all malignancies 1- 3. The discrepancy in the incidence of testicular tumors in the Caucasians compared to men of African descent has been well described in previous studies with a marked lower incidence in Africans 6- 11. Whereas the incidence is rising in the Western and Asian countries (over 60% and 40% increase in white and black Americans respectively), reports from black populations of Africa and West Indies show persistently low incidence 12- 15. We review all testicular and para-testicular tumours examined in the department of Morbid Anatomy and Histopathology, Obafemi Awolowo University Teaching Hospital, Ile- Ife, South Western Nigeria, which hosts the Ife- Ijesha cancer registry, over a seventeen year period to determine the incidence, clinical characteristics and the histopathologic variants. Methods This is a retrospective study including all patients who had histopathologically confirmed testicular and para-testicular tumors between 1989 and 2005 (17 years). Ethical clearance was obtained from the Institutional Ethical Clearance Committee. These patients had their records consisting of age, sex, laterality, and histologic variant listed in the Ife-Ijesha cancer registry which serves 4.7 million men who reside in Ondo, Ekiti and Osun states of South-Western Nigeria16. These extracted records were analyzed using SPSS version 11.0. Patients with inconclusive histopathologic reports were not included in the analysis. All the paraffin sections of the tumors stained by haematoxylin and eosin were reviewed. Special staining was done where necessary. The tumors were classified using the Mostofi classification adopted by the WHO expert committee 17. Results There were 26 cases of histopathologically confirmed testicular and para-testicular tumors over the 17 year period the study covered, giving an average incidence of 1.5 cases per year. The incidence of testicular cancer in our study was 0.55 per 100,000 population (95% CI, 0.52- 0.57). There were 2275 male malignancies in this period making testicular cancer to account for 1.1% of all cancers in men. The median age was 20 years with a mean of 26.8 ± 3.6 years. The age range was 4- 70 years. More than 65% of cases occurred in the 2nd and 3rd decades as shown in Table 1. Para-testicular tumors occurred in ten patients (38.5%) with embryonal rhabdomyosarcoma accounting for 70% of these (7 patients), others were Leiomyosarcoma (1 patient), Liposarcoma (1 patient) and Fibroleiomyoma (1 patient). On the other hand, germ cell tumors were found in eight men (30.7%). Of these, pure seminomas occurred in 50% of the patients (4 men), Embryonal carcinoma in 25% (2 men), Teratomas in 12.5% and mixed germ celltumours in 12.5%. Tumors of lymphoid tissues were seen in five patients (19.1%) and were mostly non Hodgkins lymphomas (80%). Two men had gonadal stromal tumors (7.8%) while there was one case of secondary metastasis to the testis (3.9%) from advanced prostate carcinoma as shown in Table 2. Fifteen of the tumours were on the right side (57.7%) while eight (30.8%) were left-sided. There was bilateral involvement in three cases (11.5%). Discussion Tumors of the testis and para-testicular tissues still remain relatively rare among native African men as demonstrated in our series where we had only 26 patients in a 17-year period showing an incidence of 1.5 cases per year. This low incidence has remained unchanged over the past half a century 6- 8. This contrasts with reports from the Western and Asian countries where a much higher incidence has been consistently noted R1. This high incidence in Western nations has even be noted to be rising even further 18- 20. This has been attributed to higher incidence of cryptorchidism, diets rich in oestrogen, increasing environmental (industrial) pollution and genetic factors. 3 The low incidence observed in this study contrary to the rising incidence in the black Americans, may be attributed to absent cases of cryptorchidism (a major risk factor) 21. Also, patients in this study were all native black Nigerian Africans in poorly industrialized locations. Genetic studies were not done on our patients with bilateral tumors as it is believed that many of such tumors may be hereditary in origin. More than 65% of the men were in their 2nd and 3rd decades of life with a peak age incidence in the 3rd decade (Table 1). This is in keeping with most previous reports from Africa 6- 8. The most common age observed in the USA series was 30-34 years while the lowest rates were at 15-19 years. This lower cancer age may be due to the difference in life expectancy in the two groupsR2. Right sided involvement was seen in almost 60% of cases while there were three cases of bilateral testicular tumours. These occurred in a 60 year old man with metastatic adenocarcinoma of the prostate gland, a 38 year old man with Non-Hodgkins lymphoma and in a 37 year old man with Leydig cell tumor who also had primary infertility. This bilaterality of testicular tumors occurred in 42.8% of men aged over 30 years of age in this series. The para-testicular tumors are the most common testicular neoplasia in the Ife- Ijesha cancer registry of South- Western Nigeria accounting for 10 cases (38.5%) of which most (70%) are rhabdomyosarcomas (Table 2) whereas germ cell tumors constitute the second commonest testicular tumors in the Ife- Ijesha cancer registry (Table 2) occurring in eight men (30.7%). This is in contrast with previous reports from other regions of Nigeria, Kenya and Uganda 6- 8 which all showed germ cell tumors as the most common, occurring in 64.5- 75% in those studies. Notably, the incidence of rhabdomyosarcomas which was found in 26.8%of men with testicular neoplasia in this study has remained unchanged since a similar study was conducted in Lagos, Nigeria about 17 years ago8. The emergence of the para-testicular tumors as the predominant neoplasia seems to stem from a reduction in the incidence of germ cell tumors in the men who live in the Ife-Ijesha zone of South- Western Nigeria compared with reports from the Western world. Indeed, seminomas and teratomas which account for more than 80% of Western and Asian series22, 23 only constituted 23% of our cases. We tend to agree with Zimmerman and Kung'u6 who alluded to the fact about thirty years ago that the low overall incidence of testicular neoplasia found in African series is probably due to the low incidence of seminomas and teratomas in men of African descent. Is this low incidence even falling lower? The reasons for this observed trend in our series is not fully understood but may be due to dietary factors24 since the population covered by the cancer registry is mainly agrarian with a low incidence of consuming refined food. This hypothesis may be confirmed if other researchers studying men of African descent living in agrarian areas come up with similar findings as ours. The confirmation of this decreasing incidence of germ cell tumors by other workers may also open a new vista of research into new ways of decreasing the incidence in Western and Asian countries and may result in a global reduction of this disease in men. This is of particular social and economic importance since all variants of testicular tumours have their highest incidence in men aged between 16- 44 years of age (Table 3). The patient who had bilateral testicular metastasis from advanced prostatic adenocarcinoma was incidentally discovered when his orchiectomy specimen were submitted for histopathologic analysis. No patient in this series had abnormalities of testicular descent as a predisposing factor compared with reports from Caucasians.R2 Lymphomas and tumors of lymphoid origin accounted for 19.2% (5 cases), unchanged since the report by Zimmerman and Kung'u in 19786. The fact that there was only one case of a benign testicular tumor in this study highlights the seriousness with which any testicular mass in a man should be taken as earlier reported by Salako et al 25. We suggest further studies in African hospitals and cancer registries to examine this stable incidence in testicular cancer in the native blacks and the new trend in histopathologic variant of testicular and paratesticular cancers as highlighted in this study. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10004t2.jpg] [hs10004t3.jpg] [hs10004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}