 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 18-25 Blood loss and contributing factors in femoral fracture surgery *Kajja I1, Bimenya GS2, Eindhoven B3, Jan ten Duis H4, Sibinga CTS5. 1. Department of Orthopaedics, Mulago Hospital, Kamapala, Uganda
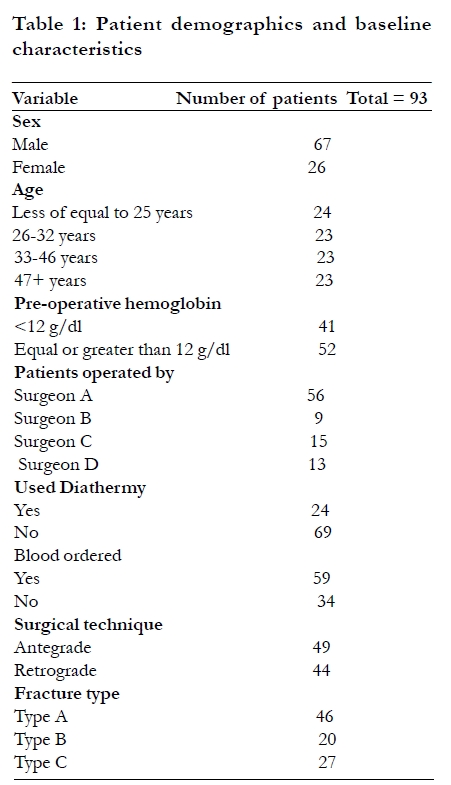
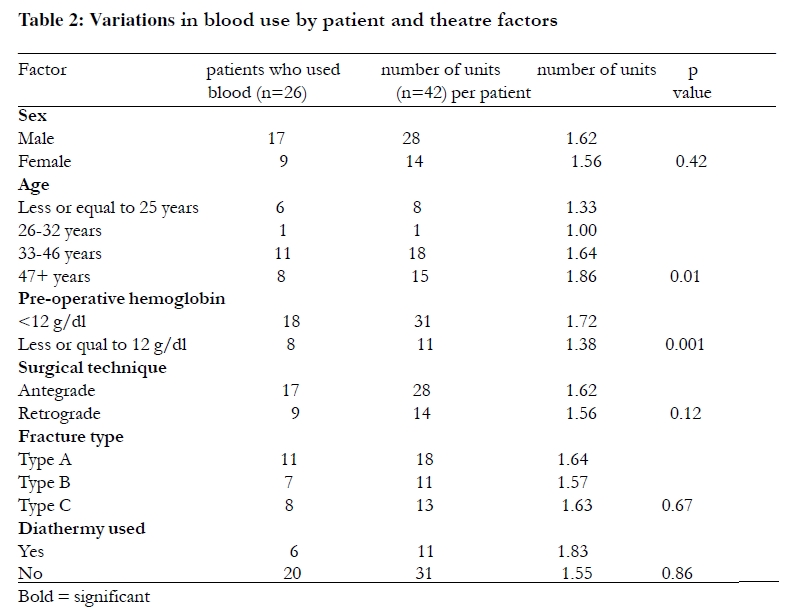
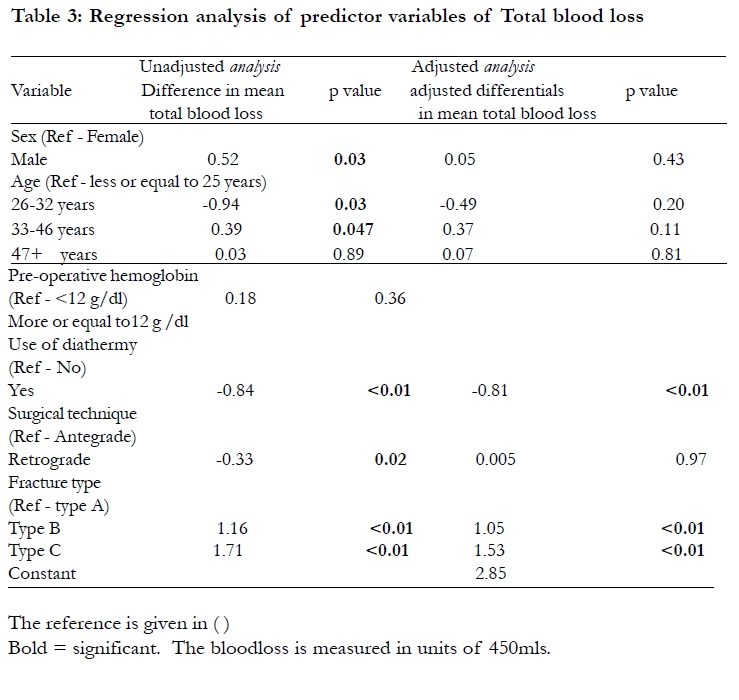
Code Number: hs10005 Abstract Background: Substantial blood losses frequently accompany orthopedic procedures. Introduction Studies of major orthopedic surgery procedures demonstrate a considerable intra-operative blood loss1, 2, 3. The amount of blood loss during surgery varies with patient and institution for a given surgical procedure 1, 2, which limits standardization of peri-operative blood orders. However, such blood losses are usually controlled by use of appropriate surgical techniques including meticulous cauterization of bleeding vessels with diathermy. Blood order schedules that result into grouping, cross-matching or holding of blood units which peri-operative use may not materialize 4, 5, stress the limited hospital blood bank financial and human resources, and limit access of the sparse blood units to those most in need. It is therefore important for each institution to establish the intra-operative blood losses and needs for the various surgical procedures performed in order to increase the efficiency of limited blood supplies. This is particularly important in the developing world. However, it may be difficult to ascertain the appropriate amount of blood loss as this varies with patient, surgeon or institutional factors 6,7. Such factors include irrational peri-operative blood transfusions in some institutions which makes it even harder to compute the exact amount of blood lost during surgery. In order to measure blood loss at surgery 8, 9, 10, two methods can be used the direct and the indirect methods. The direct method involves measuring collected blood in swabs, drainage bags and suction bottles, while the indirect method measures blood loss by hemoglobin or hematocrit changes over the peri-operative time. At Mulago Hospital, a 1500 bed national referral and major teaching hospital in Uganda, whole blood units are routinely transfused during and after orthopedic surgical procedures, the commonest of which is open reduction and internal fixation of femoral shaft fractures. It is a known fact that one transfused whole blood unit of 450mls leads to a 1g/dl elevation in the hemoglobin level measured after full hemodynamic equilibrium at 72 hours after surgery. The orthopedic department at Mulago Hospital uses the SIGN [Surgical Implant Generation Network] intramedullary nail technique11 an open intramedullary locking nail system for internal fixation of femoral shaft fractures. This is performed without use of fluoroscopy or a traction fracture table. The procedure is accompanied by massive intra-operative and post-operative hemorrhage and therefore consumes a substantial amount of blood in the peri-operative time. Unfortunately, there is limited or no information to facilitate or to streamline the appropriate blood orders in this resource limited setting. This has lead to unavoidable wastage of blood units especially when such units can not be used within the peri-operative time. The objectives of this study are first to determine the peri-operative blood loss during open reduction and internal fixation of unilateral femoral shaft fractures. In this study, peri-operative time ranged from 24 hours before to 72 hours after the surgical procedure. Second, we determined the factors that contribute to this blood loss. MethodsStudy setting The study was conducted in the wards and operating theatre of the department of Orthopedics at Mulago Hospital, the major referral hospital in Kampala, Uganda. Patients with fractures of the femur who present to this hospital do not undergo surgery until after a minimum of five days due to shortages in theater space and staffing. During this time the fractures are maintained under skin traction to control fracture site bleeding and pain. Two to five days before surgery the attending surgeons conduct preparatory pre-operative ward rounds during which they haphazardly make orders for the units of blood to be used in the peri-operative time. This resource constrained hospital has erratic supplies of blood which are competed for by many categories of patients. The shortage of blood often leads to postponement of surgical procedures. If the blood is available in the hospital blood bank, it is delivered to the operating theater a day before or on the morning of surgery and kept in a domestic refrigerator with uncontrolled temperatures until the anesthesiologist requests for it during surgery or 24 to 48 hours after surgery. Study design The study was designed as an open observational and descriptive study. Over a period of 11 months a consecutive cohort of 93 patients undergoing open reduction and internal fixation of unilateral fracture of the femoral shaft, was prospectively followed from the time a decision was made to operate up to three days after the surgical procedure. During this time, the age, gender, fracture type, hemoglobin change in levels measured 24 hours before surgery and 72 hours after surgery, representing blood loss, peri-operative blood orders and use were recorded. We also observed the surgical technique and the use of diathermy for dissection and cauterization during the surgical procedures. Inclusion and exclusion criteria All patients with an isolated fracture of the femoral shaft, sixteen years and older, were included in the study after obtaining a written informed consent. Study recruitment was done at the time when the decision to operate was made by the attending surgeon, who placed peri-operative blood orders. Patients presenting more than one month after the injury, with old non-unions of the femur, for repeat surgery for a fractured femur, with pathological fractures of the femur, with an open fracture femur, with bilateral femoral shaft fractures and patients with multiple skeletal injuries were excluded from the study due to the wide variation in intra-operative blood losses in these groups of patients. Also excluded were patients with medical and surgical co-morbidities, patients on cancer chemotherapy, patients with history of a bleeding disorder and female patients in their menses. No patient received any thrombo-embolic prophylactic drug during hospital stay. Patients were randomly allocated to surgeons. The study protocols were approved by the Mulago Hospital Research and Ethics Committee and the Uganda National Council for Science and Technology. The SIGN nail procedure This is a solid and circular inter-medullary locking nail. It has three oval slots, one proximal and two distal and one proximal circular hole. The slots allow dynamization of the locked system to stimulate bone healing while the hole limits migration of the nail in the vertical axis. The nail is fixed without an intra-operative x-ray support (fluoroscopy) since it is supplied with a special targeting device that assists in locating and locking of slots and holes proximally and distally. Blood loss The amount of blood lost due to the surgical procedure was represented by hemoglobin lost (Hb-lost) in the peri-operative time and calculated according to equation 1, where Pre-opHb is pre-operative hemoglobin (g/dl) measured 24 hours before surgery; Post-opHb is hemoglobin in g/dl level measured 72 hours after surgery; BU is hemoglobin in g/dl that was provided by transfused allogeneic whole blood units in the peri-operative time. (1 Unit equivalent to 1g/dl). Pre-opHb - Post-opHb + BU = Hb-lost.............................................equation 1. For patients who did not receive allogeneic blood the amount of blood lost was calculated using equation 2 Pre-opHb - Post-opHb = Hb-lost ………………………….equation 2. Blood sample collection Following a written informed consent from each of the participants, up to 2.0 mls of blood were collected under aseptic conditions from the cubital vein at the elbow, using a Becton Dickinson vacutainer® system containing EDTA-K3.Blood was collected 24 hours before and 72 hours after the surgical procedure when hemodynamic equilibration was assumed to have occurred. The tube was shaken to allow proper mixing of blood with the anticoagulant, legibly labeled with first and given name, age, sex and hospital number of the patient. A laboratory request form for hemoglobin determination was filled by the staff drawing the blood, who delivered both the sample and the form to the hospital central laboratory. Hemoglobin determination A technician determined the hemoglobin levels immediately after blood delivery, using the Coulter STKS (Coulter corporation, Hialeah, FL, USA) photometric system (cyanmethemoglobin method). The Coulter STKS was calibrated daily according to the manufacturer's recommendations. Blood use in the peri-operative time The decision of the anesthesiologists to transfuse peri-operatively was based on visual assessment of the extent of soaking of the operation swabs with blood and volumes of sucked blood from the operation site. This also depended on the extent of pallor of the finger nail beds, palms and mucous membranes. Whole blood units were used, each measuring 450 mls and equivalent to 1g/dl rise in hemoglobin level. Factors relating to blood loss For all participating patients, the x-ray fracture patterns, surgical technique used for fixing the fracture and use of diathermy during surgery were documented. Fracture type The fractures were classified into 3 types according to the AO System (Arbeitsgemein schaft für Osteosynthesefragen, an Association for the study of internal fixation system) which depends on the extent of comminution. Types A (the least comminuted fractures) are simple spiral, oblique or transverse fractures. Types B are wedged spiral, wedged bending or wedged fragmented fractures where Type C (the most severely comminuted) are either complex spiral, complex segmental or complex irregular fractures. Surgical techniques All patients (n=93) were operated under general anesthesia, in a supine position and without use of a traction fracture table. The surgical techniques under observation included incising of skin and other tissues and control of surgical bleeding. One group (n=24) involved the use of monopolar diathermy for incising the dermis and other tissue layers and cauterization of bleeding vessels while the other group (n=69) involved the use of a scalpel for all incisions from skin to bone and a standard surgical knot tying for the bleeders. All surgeries were performed through a straight lateral incision for manipulation of the bone segments to achieve reduction and the nails were introduced either antegrade (through the fossa piriformis) or retrograde through the inter trochelia notch of the ipslateral knee according to the surgeon's discretion. After the bone reduction and fixation with the intra-medullary nail, the inner soft tissue layers were closed with standard absorbable suture materials (chromic catgut number 2 or vicryl number 1) which ever was available. The skin was closed with non-absorbable suture material nylon number 1 in all cases. The surgical procedures were performed by surgeons (n=4) of similar training background and work experience. Statistical methods The continuous outcome variable peri-operative blood loss was tested for normality using the Normal Q-Q plot and the Shapiro-Wilk W test and showed a normal distribution. Total blood losses from patients operated by the same surgeon were not considered as independent observations. We adjusted for this clustering of observation within a surgeon using cluster command in STATA, and obtained robust standard errors for all regression estimates. For analytical purposes, continuous independent variables age and pre-operative hemoglobin level were categorized as follows; age into quartiles of years (less or equal to 25, 26-32, 33-46 and 47+), while pre-operative hemoglobin was into two groups (< 12 or more or equal to 12) g/dl. We used linear regression analysis to obtain unit change in total blood for every unit increase in the independent variable., The linear regression coefficient was interpreted as a mean difference in total blood loss comparing categories of a factor against its referent group. In the unadjusted analysis, all the factors were individually regressed against the primary continuous outcome variable- total blood loss. In the adjusted linear regression model, we included all variables significant at p<0.15 in the unadjusted analysis, or potential confounder. Statistical significance was assessed with using p<0.05 or 95% confidence interval for each estimated coefficient in the adjusted or unadjusted models. All statistical analyses were performed with the help of computer software STATA version 9.2. Results Demographics Ninety three patients were recruited presenting with unilateral fracture of the femoral shaft. There were more males 67 (72%) compared to females 26 (28%). Mean (SD) age was 40 (19.4) years, about three quarters were below 47. Mean pre-operative hemoglobin level was 12.6 (range 9.0-17.1)g/dl. Mean preoperative hemoglobin level was higher among males 12.94 (range 9.0-17.1) g/dl compared to females, 12.00 (range10.5-14.3) g/dl, (p=0.046). Most patients [n=46 (49.5%)] had type A fracture, where 20 (21.5%) and 27 (29.0%) patients had type B and type C fractures respectively. Majority of patients, 56/93 (60.2%), were operated by surgeon A, whereas the other three surgeons operated 9, 15 and 13 patients respectively. Sixty nine (74.2%) patients were operated using the traditional surgical dissection and standard surgical knotting for bleeding vessels, while 24 (25.01%) were operated with the assistance of monopolar diathermy for dissection of tissues and cauterizing bleeding vessels (Table 1). Blood use A total of 42 units were transfused to 26 patients, ten of whom received 1 unit and sixteen received two units each. Among the 26 patients who received blood (Table 2), patients in age group 33-46 years (n=11) received the highest number of transfusions [18/42 transfused units (42.8%)], while only one unit was administered to patients in the 26-32 year group (p=0.01). Thirty one units were administered to patients with a pre-operative hemoglobin <12g/dl compared to 11 units transfused to patients with a pre-operative hemoglobin e"12g/dl (n=8) (p=0.001). Six out of the 24 (25%) patients who were operated with the diathermy technique fordissections and cauterization of bleeding vessels received 11 units of blood whereas 20 out of the 69 (35%) patients operated with the traditional surgical techniques of tissue dissection and surgical knotting, used a total of 31 units of blood. Seventeen of the 49 (34.7%) patients whose SIGN nails were introduced with an antegrade technique, received 28 units of blood compared to 14 units transfused to the nine of the forty four (20.5%) who underwent a retrograde technique. Thirty three patients did not receive blood, although 70 units had been ordered and cross matched pre-operatively (Table 1). Blood loss Mean hemoglobin level measured 72 hours postoperatively was 9.75 g/dl (range 5.4-16.0). Male patients had a higher pre- and postoperative hemoglobin level compared to the female patients (12.94/10.19 vs 12.00/8.63 g/dl). Mean total blood loss assessed 72 hours after the surgical procedure was 3.31 (SD 1.56) units of whole blood. A bivariate regression analysis (Table 3) of patient and operation theater variables by total blood loss showed a statistically significant difference in the mean blood loss between male and female; 3.16 and 3.68 units respectively (p=0.03). Compared to patients in age group d"25 years, patients in 26-32 years group lost less blood, while patients in age group 33-46 years lost more blood (p=0.034 and 0.047 respectively). Patients operated with diathermy lost less blood compared to those whose operated with the traditional surgical techniques (2.68 to 3.53 units), which was statistically significant (p <0.01). Patients whose SIGN nails were introduced with an antegrade technique lost more blood compared to those with a retrograde technique (difference in mean=0.33 units, p=0.02). Fracture type significantly affected total blood loss, where patients with types B and C fractures were losing more blood compared to those with type A (p<0.01). Pre-operative hemoglobin had no significant effect on total blood loss. Factors related to blood loss Bivariate regression analysis showed sex, age, use of diathermy, surgical technique and fracture type to significantly affect blood loss. However, following a multiple regression analysis and after adjusting for other significant factors on bivariate analysis, two factors (diathermy use and fracture type) were individually found to influence blood loss. Diathermy use significantly reduced peri-operative blood loss (p<0.01) according to the following model: Blood loss with diathermy was 2.85 0.8 (units of total blood loss without use of diathermy). This means that for every unit of blood lost per patients in the group operated without diathermy, there was a 0.8 unit reduction in the amount of blood lost by the group with diathermy. Likewise, the severity of comminution of the fracture was found to significantly affect total blood loss (p<0.01). Thus, compared to fracture type A, total blood loss in units varied with positive proportionalities and according to the following model: Blood loss for type B fracture = 2.85 + 1.05 (blood loss for type A fracture). Blood loss for type C fracture = 2.85 + 1.53 (blood loss for type A fracture). This means that for every unit of blood lost in the peri-operative time of facture type A, there was a 1.05 and 1.53 unit increase in blood loss for type B and type C fractures respectively. Discussion Generally orthopedic procedures are accompanied by loss of larger amounts of blood. This is partly due to the intrinsic difficulty in stopping hemorrhage in a bleeding bone but is also due to patient and institutional factors 12, 13. Our study demonstrates that a substantial amount of blood (up to 3.31 units of 450ml whole blood) is lost due to surgery of fractures of the femur performed in a developing world operating theater. Open reduction and internal fixation of fractures of the femur is still performed widely in the developing world due to shortage of resources to support minimal interventional surgery like closed intramedullary nailing for such injuries 11. The use of appropriate surgical techniques and facilities like diathermy, fluoroscopy and fracture tables reduces operation time and intra-operative blood loss 14,15. However, these facilities are not easily accessible in hospitals in developing countries. This explains the higher blood loss among patients whose procedures were performed without diathermy. A similarly higher loss was observed by Kearns et al 15 in their work on hip hemiarthroplasties operated using scalpel alone for incision compared to incisions performed with diathermy. Wu et al 16 have also established a comparatively higher rate of blood transfusion in revision femoral fracture surgeries performed with an open technique. It is anxiety created by these losses that drives attending clinicians sometimes to irrational peri-operative transfusions. A fracture of the femur is a major traumatic event which provokes a local and systemic inflammatory response that is characterized by activation of circulating granulocytes to produce pro-inflammatory cytokines one of which is soluble thrombomodulin 17,18. This cytokine binds to thrombin and the formed complex converts protein C into the natural anticoagulant activated protein C which consumes the clotting factors 19,20.We believe that the delay in the fixation of fractured femurs at our institution with its attendant continued mobility at the fracture site must have been accompanied by sustained production of this cytokine. In addition, open reduction and internal fixation of the fractured femur is accompanied by a second hit phenomenon of more pro-inflammatory cytokine release 18. This additive effect of soluble thrombomodulin could have lead to excessive natural anticoagulant consumption resulting into disturbed hemostasis hence the observed substantial blood loss among our patients. Abrahan et al 21 in a series of 21 delayed and open intramedullary femoral fracture fixations also found an increased peri-operative blood loss. Their study was conducted in a theater without traction fracture tables or fluoroscopy, which is comparable to our theater situations. This study has also established that the greater the damage to the bone the higher the peri-operative blood loss. This is due to the fact that open reduction and fixation of severely comminuted femoral shaft fractures is a technically demanding procedure therefore carries a prolonged operation time to achieve a reduction and has an increased tendency to disrupt the endosteal and periosteal blood vessels. Although the other studied patient factors had no statistically significant relationship to the peri-operative blood loss (after the multiple regression analysis), there was a distinct difference in the loss among the different age groups. The observed higher losses among the elderly patients is in line with the advanced age related reduction in haemostatic abilities that are essential in stopping surgical hemorrhage 22. There are two main limitations of the present study. First, the differentials in blood losses of patients operated by a particular surgeon were not considered as independent variables so we cannot completely account for the salient difference between individual skills in controlling surgical bleeding. However, this lack of independence was adjusted for in the statistical analyses. Second, due to lack of operational guidelines on transfusion triggers at our institution, the haphazard use of blood by anesthesiologists in this group of patients could have resulted in the observed high peri-operative blood loss. In conclusion, isolated femoral shaft fractures in relatively young healthy patients treated by open reduction and internal fixation in a developing world operation theatre, leads to a substantial peri-operative blood loss. The major contributing factors to this loss are; the fracture pattern and lack of standard theater facilities (diathermy) necessary to limit peri-operative blood loss. Based on the above observations, the administrative structure of Mulago hospital should designs strategies first, to ensure that patients presenting with femoral fractures are operated as they come so as to shorten time between admission and surgical intervention. Secondly, to improve surgical technology by equipping the orthopedic theatres with fluoroscopy, fracture tables and ensuring that diathermy is used as a standard method of controlling surgical bleeding in all cases. Acknowledgement The authors thank the colleagues at Mulago Hospital for their cooperation and understanding. The authors certify that they have no affiliation with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in this manuscript. The authors have full control of the data gathered and presented and agree to allow the journal to review theses if requested. The study protocols were approved by the Mulago Hospital Research and Ethics Committee and the Uganda National Council for Science and Technology. All patient and staff related data have been anonymised. Research was conducted at the Department of Orthopedics, Mulago Hospital, the national referral and teaching hospital of Makerere University College of Health Sciences, Kampala, Uganda. The research is part of a PhD study of the prime author. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10005t3.jpg] [hs10005t2.jpg] [hs10005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}