 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 26-30 Prevalence and risk factors of low back pain among nurses in a typical Nigerian hospital *Sikiru L1, Hanifa S2 1. Department of Biomedical Technology, School of Health Technology, Federal University of Technology, Nigeria *Corresponding author: Lamina Sikiru, Biomedical Technology Department, School of Technology, Federal University of Technology, Oweri, Nigeria E-mail: siklam_86@yahoo.co.uk Tel: +080 25294087, 080 353 19469 Code Number: hs10006 Abstract Objective: The objective of this study was to determine the prevalence and risk factors of LBP among nurses in a
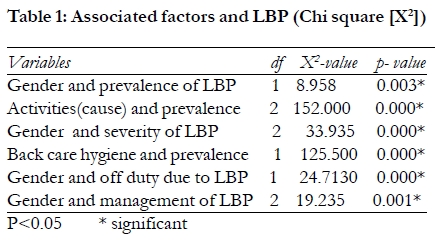
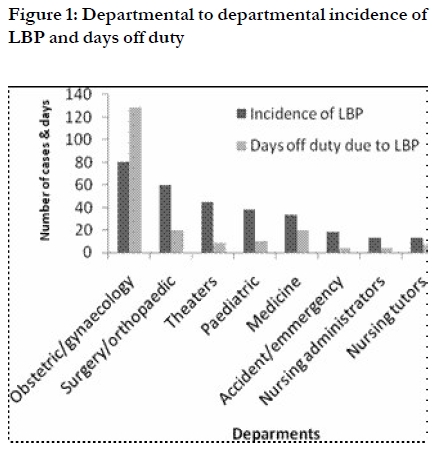
typical Nigerian Specialist Hospital. Keywords: LBP; Nurses; Ergonomics; Nigeria. Introduction Pain is an unpleasant emotional state felt in the mind but identifiable as arising in a part of the body. In other words, it is a subjective sensation. Pain is a defense mechanism designed to make the subject protect an injured part from further damage1. Low back pain (LBP), perhaps more accurately called lumbago or lumbosacral pain, occurs below the 12th rib and above the gluteal folds2,3 . Low back pain is a well recognized cause of morbidity in the industrialized world, where several studies3-6 have reported the occurrence of LBP in general population and occupational settings7-9. LBP is a common cause of morbidity in health care workers. Nurses are among the occupational groups within the health service that are vulnerable to LBP10. According to Cesena et al11 mechanical hazards in the hospitals include LBP from manual lifting (patients in particular) which makes nursing one of the occupations most affected by LBP. Describing the extent of musculoskeletal injury in nurses, survey showed that nurses lost 750,000 days a year as a result of back pain12. Harrington and Gill10 stated that LBP is the most common cause of early retirement on ground of ill health, sickness absence, job changes and a fall in the work speed among the working population. Nurses are required to lift and transport patients or equipments, often in difficult environment particularly in developing nations where lifting aids are not always available or practicable. This study was carried out to determine the prevalence and risk factors of LBP among nurses in a typical Nigerian Hospital. Method The study was a cross-sectional survey carried out among nurses in Murtala Mohammad Specialist Hospital (MMSH), Kano, North-West Nigeria. The hospital is managed by Kano State Government Parastatal, the Hospital Management Board a subsidiary of Kano State Ministry of Health. The hospital has in its employment list over 508 registered and licensed nurses and midwives. Instrument: The instrument for data collection was a self structured questionnaire developed by the investigators and validated by a jury of experts involved in the management of LBP (a physician, orthopaedic surgeon, nurse and a physiotherapist). The questionnaire sought information on identification, demographic information, prevalence, severity, back hygiene, causes, off duty status, management and duration of LBP. A reliability coefficient of 0.92 was obtained in a pilot study conducted using 50 nurses (age ranged 30-53 years, mean and SD of 37.9 + 8.71 years) at an interval of four weeks using test-retest correlation (Spearman rank order) coefficient method. Administration of the Instrument: A departmental to departmental administration of the questionnaire was adopted. The investigators administered the questionnaires to about 500 nurses who volunteered to participate in the study. The questionnaires were retrieved as soon as they were fully responded to. This made it possible for retrieving about 408 (81.6%) of the administered questionnaire. Data analysis The coded responses on the questionnaire were then entered on the computer general purpose coding forms. They were analyzed using Statistical Package for the Social Sciences (SPSS) (Windows Version 10.0 Chicago IL, USA). The results were presented with the use of simple percentage (%), mean and standard deviation (SD). Chi square (X2) was used to determine the association between variables. A probability level of 0.05 or less was used to indicate statistical significance. Results The age of subjects ranged from 25-55 years with mean and SD of 39.20+9.09 years. There were 148 (36.27%) males and 260 (63.73%) females out of which 96 (23.53%) males and 204 (50.00 %) females reported LBP; while 52 (12.75%) males and 56 (13.73%) females reported no LBP. Prevalence of LBP Low back pain presently and within the last 12 months was reported by 300 respondents (73.53%). Of the 300 respondents reporting LBP, 96 (32%) were males and 204 (68%) were females. X2 showed significant association (P<0.05) between gender (sex) and prevalence of LBP among nurses as shown in Table 1. Out of the reported LBP cases, those working in the Obstetric and Gynecology (O & G) department including labour room/ward showed high prevalence of LBP 80 (26.67%) as indicated in Figure 1. The duration of LBP was acute (less than 2 weeks in 140 (46.67%), sub-acute (lasting between 2 weeks to 3 months) in 58 (19.33%) and chronic lasting more than 3 months in 102 (34%). Prevalence of LBP increased with age; age group < 35, 36-45 and > 46 reported LBP of 19 (6.3%), 81 (27%) and 200 (66.7%) respectively. Causes of LBP 200 (66.67%) of the LBP cases believed that their LBP was related to their work (occupation) while 40 (13.33%) and 60 (20.00%) associated their back pain with domestic and previous trauma respectively. There was significant association between activities (causative factors) and incident of LBP at p< 0.05. Back care ergonomics All respondents (100%) with no LBP had previous knowledge of back care hygiene. 80 (26.67%) of nurses with LBP had knowledge of back care hygiene while 220 (73.33%) LBP respondents had no knowledge of back care hygiene. Table 1 showed significant association between knowledge of back care ergonomics and incident of LBP. Severity of LBP One hundred and thirty 130(43.34%) nurses indicated that their pain was mild and that it did not disturb their daily activities; 116 (38.66%) reported that it was moderate and 54(18%) was severe. Out of the 116 nurses with moderate LBP, 53 reported that it prevented from going to work while the remaining 63 only reported restriction in daily activities. 54 (18%) thought it was severe, preventing them from going to work. Table 1 showed significant association between gender and severity of LBP. Day's off-duty due to LBP About 107 (35.67%) who reported LBP had been off-duty in one time or the other for the past 12 months. Out of this, 92 (85.98%) were females while 15 (14.02%) were males. Female nurses reported 164 (81.19%) days while males reported 38 (18.81%) days off-duty. There was a significant association between sex and days off-duty at P<0.05. A total of 202 off-duty days was reported by those with LBP, The highest number of off duty days (129 days [63.86%]) was from Obstetrics and Gynecology department including Labour wards, followed by Medicine and Surgical Unit with 20 days (9.90%) each. The least off duty days (4 days [1.98%]) each was reported from Accident and Emergency Unit and among nursing administrators. Two hundred and two days off-duty was reported by 107 nurses resulting to an average of 1.89 days (approximately 2 days) within 2 months. The total working days for all respondents were 148,920 days (408 X 365) and total off-duty days were 202 (0.14%). Management of LBP Of those with LBP, 125 (41.67%) sought relief from medical consultation prescriptions, 81 (27%) sought relief by physiotherapy, while the remaining 94 (31.33%) sought relief by self medication. Discussion The 12 month prevalence of LBP in this study was 73.53%, this is considered high and was in line with that reported by Maul et al13. They reported high annual prevalence varying from 73% to 76% among nurses employed by a large university hospital in Switzerland. The present study also concurs with the findings of Knibbe and Friele14 and Smedley et al15. They reported slightly higher prevalence varying between 56% and 90% among nurses. The increase in prevalence of LBP with age in the present study may not be unconnected to the report of study carried out by Charlotte and Stuart16 that the susceptibility of chronic diseases increases with age; this increase is a reflection of both physiological changes and cumulative environmental (occupation) and genetic risk factor exposure. Despite this high prevalence, the etiology and nature of LBP are not yet well understood. Many studies have reported a strong association between musculoskeletal disorders and work related factors12, 17-19 and work pressure20. This was also found among nurses21. In the present study, 66.67% related their LBP to their occupational hazard. Poor working and incorrect lifting postures has been implicated as causative factors in LBP22-27. In the present study, all nurses without LBP (108) had previous knowledge of back hygiene while 220 (77.33%) with LBP had no knowledge of back care hygiene. Significant association (P<0.05) was found between back care hygiene and incident of LBP among nurses as shown in Table 1. There was a significant association (P<0.05) between sex and severity of LBP. Males reported 16.67%, 5.33% and 10% for mild, moderate and severe LBP, while females reported 26.67%, 33.33 and 8% for mild, moderate and severe LBP respectively. Generally, 64.86% of the total male reported LBP while 78.46% of the total female reported LBP. Significant association was found between gender and prevalence of LBP. The reason for female preponderance in this study is unclear but it may be related to the anatomical, physiological and structural difference between males and females; also mechanical disadvantage, sprain and strain, are more common in females than males28-30. Back muscle weakness, sprain and strain (low back sprain), has been implicated as a causative factor of LBP 2,27,31 . In the present study, nurses generally lost about 202 working days in 12 months (408 X 365 days) amounting to about 0.14%. This is considered very low. LBP has been identified as one of the main causes of loss of hours and days among the working class citizens. Frost and Mofett32 reported that the time off work due to LBP in England in 1989 increased by 40% in comparison to 5.6% for other complaints. The survey showed by Triolo12 indicated that nurses lost 750,000 days a year as a result of back pain. The reasons for low loss of working hours and days in the present study might not be unconnected to fear of premature retirement or termination of appointment by employers on the pretence of ill-health. Also, nurses and employers often reject excused duty (complete rest) due to severe shortage of staff coupled with high turn out of patients. There was a significant gender association with off duty days at P<0.05, this is due to the fact that females reported high incidence of LBP. In the present study, obstetric and gynecology including labour ward reported the highest incidence of LBP 80 (26.67%) while nursing administrators and tutors reported the least of 13 (4.33%) each. The highest in O & G department might be related to the fact that only female nurses (midwives) work in O & G department and prevalence is more in females. It might also be related to work pressure in O & G including labour ward in MMSH. Management of LBP with physiotherapy, chemotherapy and surgery has been well established25,33. There was no sex difference in consultation and management of LBP, but there was a significant association between severity of LBP and type of management adopted by nurses at P<0.05. Conclusion The prevalence and cause of LBP in MMSH, Kano, Nigeria is similar to those reported within and outside Nigeria. The study concluded, therefore that LBP is a widespread disease affecting nurses but not a major cause of sickness absence in the workplace. Poor knowledge of back care ergonomics and unavailability of lifting equipment are major predisposing factors to LBP among nurses (occupation hazard oriented). Recommendation (1) Refresher course on back care ergonomics and patient transfer should be organized for nurses on regular basis. (2) Hospitals should be well equipped with all necessary lifting equipment. All these might go a long way in reducing the high rate of LBP among nurses. Acknowledgements The authors are grateful to all the nurses at the Murtala Mohammad Specialist Hospital, Kano, for their cooperation during the collection of data. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10006f1.jpg] [hs10006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}