 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 31-39 Antenatal determinants of oro-facial clefts in Southern Nigeria Omo-Aghoja VW1, *Omo-Aghoja L O2, Ugboko VI3, Obuekwe ON4, Saheeb BDO4, Feyi-Waboso p5. Onowhakpor A2 1Department of Oral and Maxillofacial Surgery, Central Hospital, Sapele, Nigeria Code Number: hs10007 Abstract Objectives: Cleft lip with or without cleft palate, is the most common serious congenital anomaly that affects the
orofacial regions. The management and care of the cleft patient constitutes a substantial proportion of the workload of the
Nigerian maxillofacial surgeon and allied specialties. Yet, there are no specific programmes targeted at this group. We believe that
the findings of this study is capable of identifying useful interventions for designing programs that will lead to a reduction
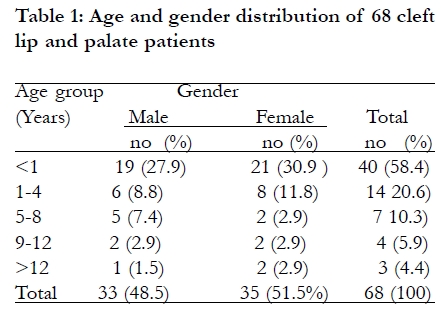
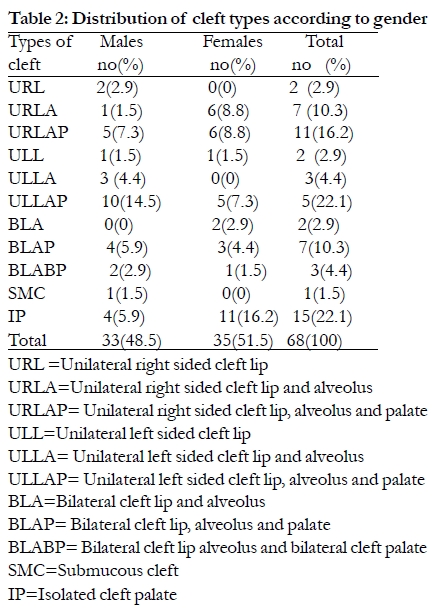
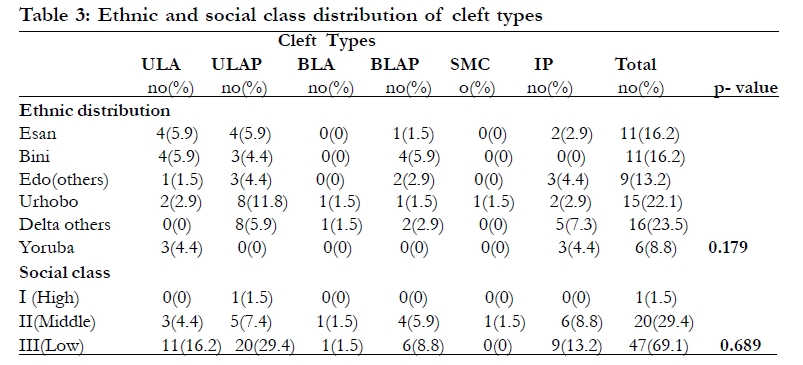
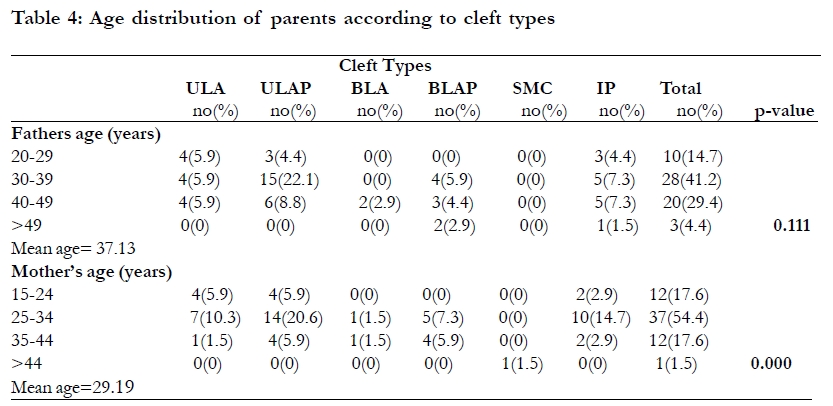
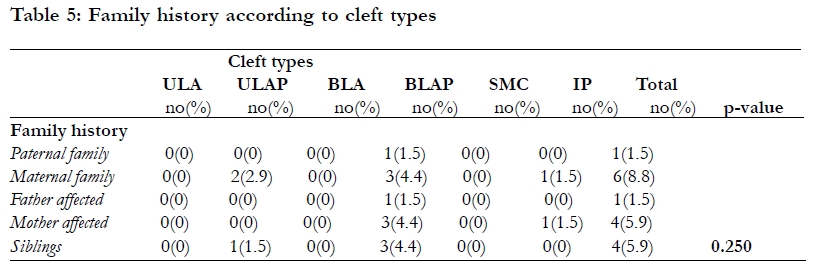
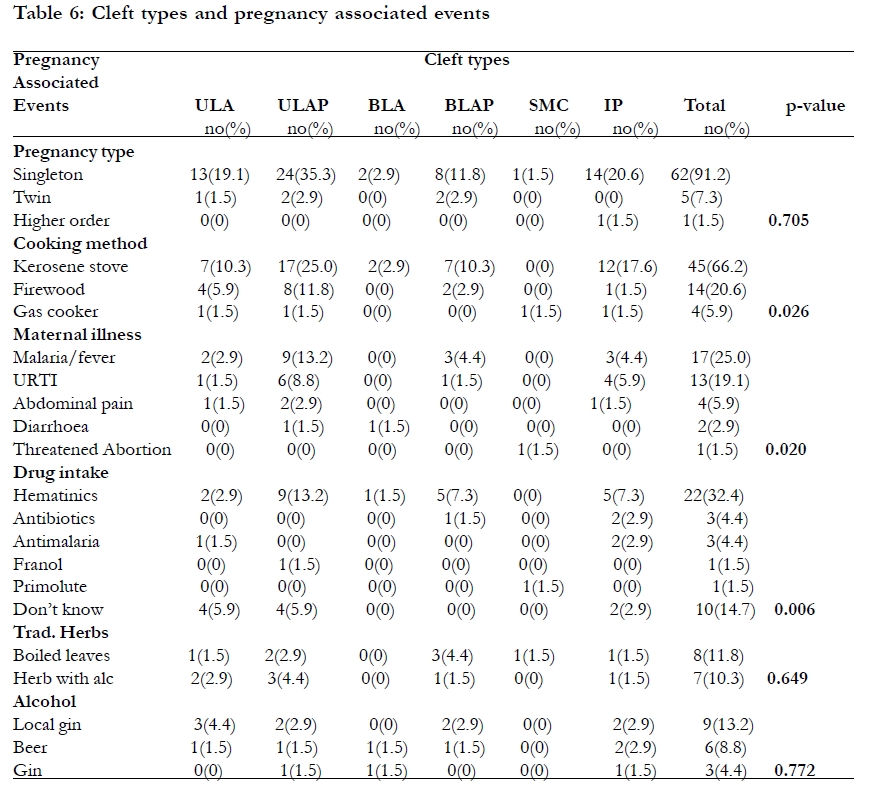
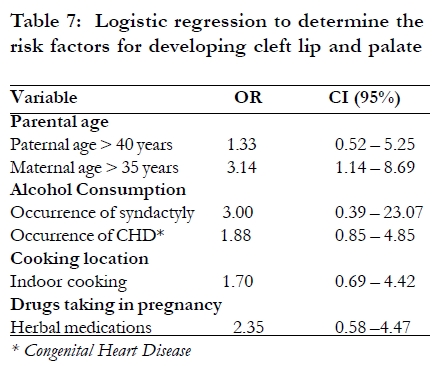
in the burden of orofacial cleft in Nigeria. Key Words: Prevalence, Antenatal determinants, orofacial clefts, Southern Nigeria Introduction Available evidence indicates that cleft lip with or without cleft palate, is the most common serious congenital anomaly that affects the orofacial region1 in humans. These deformities can be seen, felt and heard hence they constitute a serious affliction to those who have them and their families. Reports1,2,3 show that there is higher incidence of cleft in the Asians than in the Caucasians and least amongst the black race. The worldwide incidence is reported to be 1 in 700 among Asians and 1.7/1000 live births amongst Japanese. It is 3.6/1000 live births in a group of American Indians and 1/1000 live births amongst Caucasians. Boys are affected more than girls with a ratio of about 3:21. Clefts of the lip are more frequent in boys (60%) while isolated clefts of the palate are more frequent in girls (59%).4 Although the etiology of cleft lip and palate is uncertain, studies1,2,4 suggest that it is multifactorial with both genetic and environmental factors implicated. In 20-30% of patients with left sided cleft there are associated hereditary factors6. The probability of a child having cleft lip is reported to be 2% if one of the parents has a cleft but this increases to 14% in subsequent children if a child already has a cleft. If neither of the parents has cleft but one child has it, the chances of another child having a cleft are 4.5% and this increases 2, 4 and 40 times in third, second and first degree relatives of affected patients2,3. On the other hand, several reports1,2,4,6 have associated a number of environmental factors with the causation of cleft. Such factors include vitamin deficiencies particularly vitamins A and B, viral agents such as the rubella virus and infestation with toxoplasma gondii the causative agent of toxoplasmosis. Others are exposure to irradiation, cortisone excess and ingestion of drugs like thalidomide, steroids, anticonvulsants (phenytoin), diazepam, amino pectin and nitrogen mustard, subjection to hypoxic situations, ACTH excess, maternal alcohol consumption and cigarette smoking, all in pregnancy especially in the first trimester 1,2,4,6. The care of patients with cleft lip and palate is quite challenging for both parents and the care givers as the patients have to be seen and monitored from birth to early adulthood1,4,6. This is often due to the fact that such children have associated defective sucking, hearing defect and airway obstruction1,2,4,5. Others are speech defect, poor aesthetics, malocclusion, as well as dental abnormalities like missing teeth, rotated teeth and malpositioned teeth1,4,6. Provision of health care for these patients is therefore protracted and expensive as it involves many different specialties. Although the reported incidences of cleft lip and palate in the few published Nigerian works 7,8,9 is less than the Caucasian and Oriental figures, the management and care of the cleft patient still constitutes a substantial proportion of the workload of the Nigerian maxillofacial surgeon and allied specialties. Yet, there are no specific programmes targeted at this group in order to reduce the incidence and offer comprehensive management strategies geared towards optimizing outcome of treatment. The purpose of this study therefore, is to determine the prevalence and associated risk factors of cleft lip and palate in UBTH and Central Hospital, both in Benin City. We believe that the findings of this study is capable of identifying useful interventions for designing programs that will lead to a reduction in the burden of orofacial cleft in Nigeria. Method It was a transverse cross-sectional study that was undertaken from November 1 2006 to October 31st 2007. The study was conducted at the Maxillofacial Units of the University of Benin Teaching Hospital (UBTH) and the Central Hospital (CH), Benin City respectively. UBTH is the largest tertiary center with 575 bed spaces and CH is the largest secondary health institution with 435 bed spaces, in Edo state of Nigeria. They serve as referral centers for Edo, Delta, Ondo and Kogi States with an overall approximate population size of about 14 million people (2006 National population census). The sample size of 60 was determined using Taylor's Formula10 and the maximum known prevalence of 0.4/1000 live births reported in Nigerians7, although all 68 consenting patients with Cleft defect seen in the Hospitals within the study period were included in the study. Patients who declined giving their consent and those with previous cleft repair presenting for follow up were excluded from the study. A pre-tested and validated study protocol was used for the data collection. The study protocol which was filled by trained interviewers elicited the following information; socio-demographic profile of the patients and parents, family history surveying both paternal and maternal aspects particularly family history of cleft (we did not evaluate family history of other congenital anomalies), dietary/nutritional history, patient's antenatal and delivery history. Specifically, the protocol explored the following antenatal events parental history of alcohol ingestion, cigarette smoking, cooking method, drug use during pregnancy and exposure to irradiation. Approval for this study was obtained from the Ethics committee of the University of Benin Teaching Hospital. The rights of patients to participate or not was respected, and the study was carefully explained to the patients or their parents and their informed consent obtained before they were recruited into the study. All information obtained was recorded on the data collection sheet designed for the study. The coded data were then fed into the computer using the SPSS statistical software and analysis was conducted. This consisted of univariate and bivariate analysis and comparisons of identified relationships. Test of the statistical significance was based on 95% confidence interval using Chi square test with the Yates or Fischer exact correction where applicable. Odds ratio and confidence interval was then calculated to determine the association between the risk factors and cleft lip and palate. Results Overall, 5,037 patients presented at the Dental Centres of UBTH and CH Benin City for treatment during the study period, and 68 of these patients had cleft lip and palate giving a prevalence rate of 1.35%. There were 33 males (48.5%) and 35 females (51.5%) whose ages (Table 1) ranged from 5 days to 37 years (mean + SD; 3.22+ 6.82 years). The mean age for males was 2.9+ 6.8 years while that of females was 2.9+ 7 years, this difference is not statistically significant (P> 0.05)). Forty patients (58.4%) were children less than a year with 14 (20.1%) less than a month old. Three adult clefts were also seen during the study period (two females and a male). Over half of the cases (58.8%) were delivered at maternity homes, while home deliveries accounted for 5 cases (8.7%), 8 patients (11.8%) were delivered at Traditional birth attendants' homes and 15 patients (22.1%) at general and teaching hospitals. Of the 68 patients, there were 40 cases (58.8%) of unilateral cleft lip with or without cleft palate, 12 cases (17.6%) of bilateral cleft lip with or without cleft palate, 15 (22.1%) of isolated cleft palate and 1 case (1.5%) of submucous cleft as shown in Table 2. The unilateral clefts were equally distributed on the right and left sides of the face but had more male distribution (23 cases). While equal distribution of bilateral cases was observed amongst male and female patients (Table 2), isolated cleft palate in contrast, had more female distribution (11 females and 4 males). Overall, thirty six patients (52.9%) had combined cleft lip and palate defects, 4 patients (5.9%) had isolated cleft lip, 12 patients (17.6%) had cleft lip and alveolus while 15 patients (22.1%) had isolated cleft palate. Of the 12 patients (17.4%) with bilateral cleft, 10 patients (14.9%) had combined cleft lip and cleft palate. The single case of submucous cleft palate presented with bifid uvula, palatal bone dehiscence and covering oral epithelium. Of the 68 patients who presented during the study period, the ages of 61 fathers (89.7%) and 62 mothers (91.2%) were obtained while others failed to volunteer such information. The ages of the fathers ranged from 20 years to 70 years with a median of 37 years (mean + SD; 37.13 + 8.51 years), while that of the mothers as shown in Table 5 ranged from 15 years to 45 years with a median of 28 years (mean + SD; 29.19 + 5.86 years). The difference was statistically significant (p <0.05). Among the various paternal age groups, 41.2% were within the 30-39 year age group and they accounted for a significantly high proportion of patients (22.1%) with unilateral cleft lip and palate while a greater percentage of mothers (54.4%) where in the 25-34 age group and they accounted for a significantly high proportion of patients (14.5%) with isolated cleft palate. A family history of cleft was obtained in 9 patients (13.2%) with cleft palate either in isolation, or with cleft lip. Of the 61 fathers and 62 mothers, there were positive family history in one father (1.5%) and 4 mothers (5.9%) respectively (Table 5). Additionally, there was a positive family history from 6(8.8%) maternal relatives and one paternal relative. Four patients (5.9%) had siblings with a cleft. Bilateral cleft lip and palate was the cleft type noted to be most commonly associated with family history (5 cases) while patients with cleft lip alone or cleft lip and alveolus had no family history of cleft. Three mothers had van der woude syndrome and this was replicated amongst two of their children. Although nine patients had positive family history, some patients had multiple family history with the highest record of a patient whose mother had bilateral cleft lip, and also additional maternal and paternal family history of cleft lip and palate. Thirty-seven patients (54.4%) had a positive history of maternal illness during their pregnancy course with 17 (25%) being febrile illness/malaria, followed by upper respiratory tract infection in 13 mothers (19.1%). Others were abdominal pain in 4 cases (5.9%), diarrhoea in 2 cases (2.9%) and 1 case (1.5%) of threatened abortion (Table 6). A total of 40 mothers (58.8%) ingested orthodox medications during their pregnancy and another 15 mothers (22.1%) took herbal medications. Twenty two (32.4%) of such mothers ingested routine antenatal hematinics, three mothers (4.4%) took antibiotics while 3 others (4.4%) ingested antimalarials. Other drugs taken include one each of primolut injection and franol while a significantly large number of mothers (14.7%) took unspecified medications as shown in Table 6. None of the mothers volunteered a positive history of cigarette smoking or tobacco consumption. However, majority of them (66.2%) cooked with kerosene stove followed by firewood in 14 (20.6%) cases and gas in 4 (5.9%) cases (Table 6). Thirty four patients (50.0%) had their kitchens located outdoor, 30 (44.1%) cooked indoors while kitchen location could not be ascertained in 4 (5.9%) cases. This difference was not statistically significant (p>0.05). Eighteen mothers (26.5%) ingested alcohol during their pregnancy with 9 cases (13.2%) taking local gin, thus making local gin the most frequently ingested type. Seven mothers (10.3%) suffered one form of trauma or the other while 13 mothers (19.1%) had radiographic exposure during pregnancy. The highest incidence (10.3%) of radiographic exposure was in the third trimester. Of the study population, 6 (8.8%) were products of multiple gestation with five sets of twins and a set of triplet. Among the twin pregnancies, there were 2 cases of monozygotic twinning and 3 cases of dizygotic twining. The only set of triplets was monozygotic. Of the affected dizygotic twins, 2 (2.9%) were females and one was a male while the monozygotic twins were all boys. In all cases of multiple gestations, only one of each set was affected. Majority of the patients (92.6%) were delivered at term while one each of preterm birth (34 weeks) and postdated delivery (45 weeks) was recorded. The mean gestational age in this study was 37.64 + 1.82weeks. We further subjected the key risk factors for cleft development to logistic regression analysis to eliminate the impact of chance and or other confounding variables, and the positive findings noted are shown in Table 7. Discussion This study showed an overall prevalence rate of cleft lip and palate in the two Benin City hospitals to be 1.35%. Interestingly from the literature search, it was difficult to locate any Nigerian study that documented the prevalence of cleft lip and palate amongst patients seen in any of our maxillofacial centers. The only study that reported on population incidence (prevalence at birth) was by Iregbulem7 from Enugu in eastern Nigeria when he found a prevalence rate of 0.04% after he examined 21,624 consecutive infants born at the University of Nigeria Teaching Hospital over a 5-year period. However, in this study setting prevalence of 1.35% is at variance with other studies with a known range of 0.06% 0.2%11-13. The studies from which these prevalences were derived had larger sample sizes as compared to this study conducted on patients who attended the dental clinics. Although the overall prevalence of cleft lip with or without cleft palate has been reported to be commoner in males than females,9,14-22 this study revealed the contrary with a slight female preponderance which was however not statistically significant (p-value = 0.103). Similarly, isolated cleft lip was commoner in males than females this being similar to other study setting16-22 as was isolated cleft palate in females as widely reported.9,23-27 While there has been no consensus on the most common type of cleft lip and palate,14,15,28-31 this study revealed combined unilateral cleft lip and palate as the commonest type of cleft in Benin City with no side predilection but commoner in males than females. A high prevalence of cleft palate either in isolation or in combination with cleft lip (75%) was also noted in this study which agrees with reports from West Scotland, Northern Ireland and Finland.24,25 Varied literature32-35 reports suggest that both genetic and environmental factors interact in the aetiology of orofacial clefts. This fact is clearly replicated in this study as family history is positively associated with the risk of cleft deformities in 13.2% of the study population which is in keeping with previously reported incidence of 10-20%32. Lack of 100% genetic factor34,35 in the aetiology of cleft in twins was also identified in this study as only one each of all patients of multiple gestation in this study had cleft. This further gives credence to the fact that environmental factors play a significant role in the aetiology of orofacial cleft deformities. In fact, it is likely that environmental factors probably were the major agents at play in those twin patients that were seen in this study. Certainly further study in this regard is advocated. Although the highest incidence of genetic factor in cleft aetiology has been reported in females with bilateral clefts 33,36 this study recorded a higher proportion of males with bilateral cleft lip and palate. While the role of both maternal and paternal ages in the aetiopathogenesis of cleft remain contentious,37-40 maternal and paternal ages greater than 35 years and 40 years respectively were observed as significant risk factors for the development of specific cleft types. Paternal age greater than 40 years is specifically more associated with isolated cleft palate (OR=1.33 CI=0.52-3.25) in agreement with previous report by Bille et al.37. Likewise, maternal age greater than 35 years was significantly more associated with bilateral cleft lip and palate and unilateral left sided cleft lip and palate (OR=3.14 CI=1.14-8.69; OR=1.35 CI=0.75-3.05) respectively. Although the effect of socioeconomic class as an aetiologic factor in the development of cleft lip and palate is still in contention,32 well over half (69.1%) of the study population came from low socioeconomic class. The exact import of ethnicity on the risk of development of cleft deformities in this study is not certain, even though it was noted that various ethnic groups were associated with different types of cleft. The Urhobo's of Delta State who made up the largest single ethnic group of this study commonly had unilateral left sided cleft lip and palate, unilateral right sided cleft lip and alveolus and bilateral cleft lip and alveolus. While amongst the other ethnic groups in Delta State, the commonly encountered cleft deformities were cleft palate, either in isolation or with cleft lip and alveolus. The reasons are inexplicable bearing in mind that all the ethnic groups live within same environmental milieu, have similar dietary pattern, alcohol intake and cultural norms. On the other hand, the Bini's who constituted the second largest ethnic group are more likely to have isolated cleft lip and bilateral cleft lip with bilateral cleft palate. In keeping with existing data41-43 on the impact of alcohol consumption on the risk of developing cleft deformities, a positive association was noted between alcohol intake and development of cleft palate with or without cleft lip in mothers who took alcohol occasionally or regularly. Also, it was noted that there was an increased risk of having a child with other congenital defects in mothers who drank alcohol during pregnancy especially syndactyly (OR=3.0 CI 0.39-23.07) and congenital cardiac anomalies mainly ventricular septal defect, atrial septal defect and patent ductus arteriosus (OR=1.13, p=0.011and OR=1.88) respectively. Cigarette and tobacco smoking are well documented risk factors for orofacial cleft.42-52 However, in this study there was no history of smoking in any form by the mothers of our cleft patients. But what gives an indication of the relationship between smoking and risk of developing cleft deformities in this study was the evaluation of the cooking method and the location of their kitchens. It was noted that there was an increased risk of unilateral left sided and bilateral cleft lip and palate (OR=1.70 CI=0.69-4.42; OR=1.42 CI=0.42-4.80) respectively in those who cooked indoors as compared to those who did their cooking outdoors. The implication of this being that those who cooked indoors were more likely to have inhaled smoke from the cooking source that can be likened to cigarette smoking. An increased relative risk (OR=2.35 CI= 0.58-9.47) was also noted in isolated cleft palate and unilateral left sided cleft lip and palate (OR=1.08; CI=0.39-2.94) in mothers who took herbal medications during their pregnancy. The potential limitations of this study was the fact that part of the information/data collected were based on history from the patients and or their parents and therefore there was the possibility of concealing facts or information and indeed may even have recall bias. However, efforts were made to overcome this difficulty by counseling the patients/parents appropriately. The importance of volunteering accurate information/data was emphasized vis-à-vis the patient's management and identifying preventive strategies that will avoid a recurrence in future conceptions in the family. Additionally, efforts were made to determine the associated environmental risk factors for the development of clefts and not genetic factors, which was only indirectly inferred from the family history due to lack of facilities for DNA testing at both centers. Conclusion In conclusion, this study revealed that cleft lip and palate are encountered often in clinical practice in Benin City with prevalence higher than the overall worldwide prevalence and those from other regions of the world. Also, this study revealed that orofacial cleft lip +/- palate were commoner in females and that the combined unilateral cleft lip and palate was the commonest entity in the study. A number of risk factors that were associated with the risk of development of cleft lip and palate were recorded they include paternal age >40years, maternal age >35years, genetic/family history, low socio-economic status, alcohol consumption and indulgence in the intake of herbal medications in pregnancy. Certainly a larger country case control study is advocated to conclusively document a national prevalence of orofacial cleft and the associated risk factors/aetiology in Nigeria. This will help in quantifying the burden of orofacial cleft and also identify national strategies that will help reduce the incidence and improve its management. There is the need for public health education programmes and advocacy activities on the identified risk factors from this study for the development of cleft lip with or without cleft palate and preventive measures to obviate the occurrence amongst the populace. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10007t6.jpg] [hs10007t5.jpg] [hs10007t4.jpg] [hs10007t7.jpg] [hs10007t3.jpg] [hs10007t2.jpg] [hs10007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}