 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 54-57 Ophthalmic admissions in a tertiary hospital in Nigeria *Onakpoya OH, Adegbehingbe BO, Adeoye A O, Adewara BA Ophthalmology Unit, Department of Surgery, College of Health Sciences, Obafemi Awolowo University, Ile-Ife, Nigeria Correspondence author: *Dr Onakpoya Oluwatoyin Helen, Ophthalmology Unit, Department of Surgery, College of Health Sciences, Obafemi Awolowo University, Ile-Ife. Email:uvtoyin2@yahoo.co.uk; ufuoma@oauife.edu.ng Tel : +2348037194945. Code Number: hs10010 AbstractBackground: Hospitalization for eye care is required for different reasons. The pattern of admissions into the
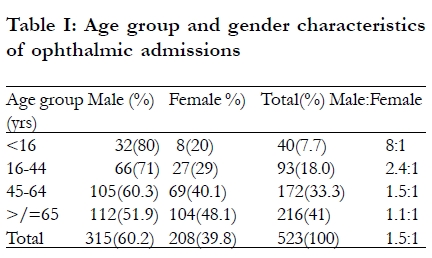
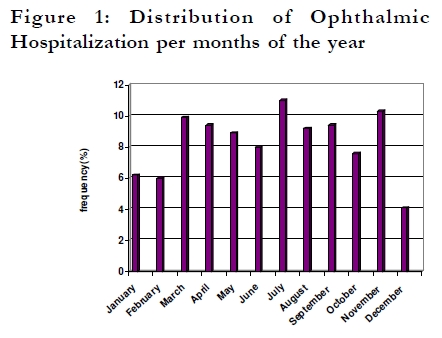
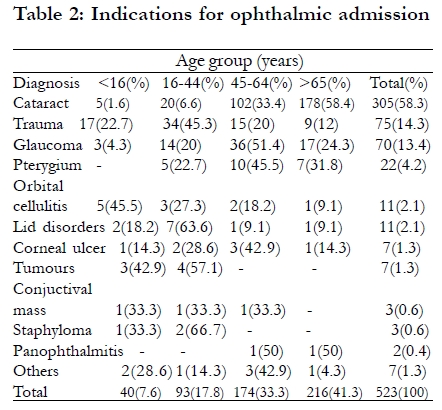
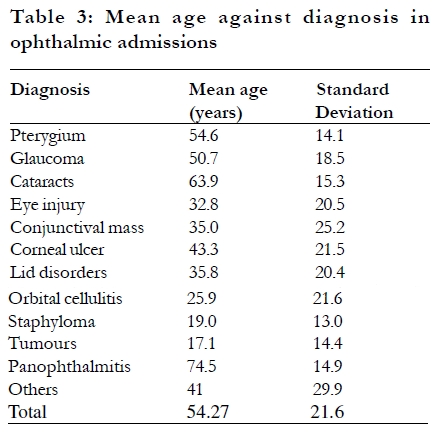
ophthalmic wards of a sub-urban tertiary hospital was studied. Keywords: Hospitalization; Eye care; Daycare; Cataract; Glaucoma; Nigeria Introduction Traditional hospitalization for in-patient care remains an integral part of specialist eye care globally. In-patient eye care is required for different reasons and eye diseases.1-7 Medical reasons, surgeons preference, ocular surgeries, presence of home support and distance of patients domicile from the hospital are among the factors guiding ophthalmic admissions.1-4,8 Medical reasons for ophthalmic admissions range from the need for intravenous medications, frequency of monitoring or application of topical medications, vision threatening disorders to head positioning.1 In- patient care is costly for the health system and the patient; the necessity for admission must be justified since out-patient eye care reduces the cost.2 The indications for admission varies in different centres; infection and trauma were the leading indications for ophthalmic admissions in southwestern Nigeria while retinal detachment and trauma were the leading indications in Paris.1,9 The rates and duration of admissions for ophthalmic care may be influenced by ethnicity and may be indicative of the level of efficiency of ophthalmic care and management in the region studied.5 In sub-saharan Africa, there is maldistribution of the few available Ophthalmologists;10 this in combination with the many isolated rural communities translates to many patients living far from the available ophthalmic centres. Studies on pattern of ophthalmic admissions in sub saharan Africa is sparse; those available deal with specific subsets like trauma and children.9,11 The characteristics of ophthalmic admissions have important implications for ophthalmic health care planning.5 This study of the pattern and indications for ophthalmic admission was carried out in a tertiary hospital located in a sub-urban city in Nigeria to provide data which will be informative in planning efficient eye care for the area served and the next phase of development plan for the Ophthalmology Unit. Methods A retrospective study of the patients managed as in-patients in the Ophthalmology wards of the Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, from January 2004 to December 2007 was conducted. Patients who were admitted for 24 hours or more were considered as inpatients and constituted the study population.2 Patients who were admitted for observation for less than 24 hours or for day-case surgeries were excluded. The tertiary hospital is located in a sub-urban city and serves as a referral centre of eye care for patients in Ife-Ijesa zone of Osun State and some parts of Ondo, Ekiti, Oyo and Edo States; self reporting patients are also managed. Information on the age, sex, diagnosis and duration of hospital stay were retrieved and recorded for each patient and diagnoses were further grouped for easy presentation. Data was imputed into SPSS version13 and analyzed for simple descriptive statistics. Variables were further compared using chi square and ANNOVA as appropriate and statistical significance inferred at P<0.05. Results Five hundred and twenty three patients admitted during the study period formed the study population. Most of the patients 315 (60.2%) were males while 39.8% were females (p<0.0001). The male preponderance becomes less prominent with increasing age (P=0.001). The number of patients admitted in the ophthalmic wards increased with increasing age with 388 (74.6%) aged forty- five years and above while 40(7.6%) were children (Table 1). The duration of admission ranged between 2 and 24 days with a mean of 2.86± 1.95 days; 63% were admitted for 3 days. Ophthalmic admissions peaked in the months of July (11%) and November (10.3%) while it was lowest in December (4.1%). (Figure 1) The main indications for admission were for surgical management of cataract (58.3%), ocular trauma (14.3%) and for surgical management of glaucoma (13.4%). Eye injuries were more common (68%) among children and young adults while cataract and glaucoma were the leading indications in middle aged and elderly as indicated in Table 2. The mean age of patients admitted for trauma and tumours were significantly lower than for cataract and glaucoma (P <0.0001) as shown in Table 3. Discussion Male preponderance is similar to the male to female ratio of 1.3:1 reported in a tertiary hospital in Midwestern part of Nigeria.6The reduction in the degree of male preponderance with increasing age in this study may be related to the differences in the indications for admission in the different age groups. Ocular trauma had been previously associated with male preponderance;11-13 trauma was the most prominent indication for admission amongst children and young adults in this study thus accounting for the marked male preponderance in the younger age group. Prevalence of blindness increases with increasing age and cataract is the leading cause blindness in Nigeria.14,15 Cataract was the leading diagnosis amongst the patients studied; thus accounting for the trend of increasing number of admission with increasing age. Ferguson et al16 reported an increase in age specific ophthalmic admission rates among the elderly with increase in cataract procedures being a major contributory factor; a decrease in admission rate for children was also accounted for by decrease in admission for strabismus. In our series, no patient with strabismus underwent surgery during the study period hence the absence of strabismus as indication for admission. Sixty three percent of patients were admitted for three days while the mean duration of admission was 2.86± 1.95 days. Gaujoux et al in Paris reported a mean duration of admission of 3 days while Onabolu reported a mean stay of 2.87 days.1,9 Prolonged length of stay may be a reliable surrogate measure of disease severity.2 In our study, patients that were admitted for cataract or glaucoma surgeries usually stay for three days. Although the advantages and safety of daycase cataract surgery are known,3,17,18 this practice remains restricted to well selected few in our environment. Hospitalization for cataract surgery is still required as many patients live far from the hospital in numerous isolated communities with poor road network such that it becomes more expensive and painstaking for the patient and escort relative to travel to and from the hospital for a daycase cataract surgery compared to being hospitalized. Moreover, the absence of outpatient-housing,1 adequate home support including ease of communication with health facility makes traditional hospitalization for cataract surgery to remain relevant for many patients in our setting. Ocular trauma may require in-patients care especially when severe, open, and associated with hyphaema or with other injuries requiring admission. Longer hospitalization periods are reported for traumatic eye admissions with 65% staying longer than seven days.11 Glaucoma was responsible for 8.1% of all ophthalmic admissions in Pakistan 4 as compared to 13.4% in our series. While there is a decline in the rate of glaucoma surgery in advanced countries due to the availability of newer topical medications to lower intraocular pressure,7 surgery still remains the mainstay of treatment for glaucoma especially among black African patients due to poor compliance with medical therapy for various reasons especially from the unavailability and high cost of topical therapy.19 In conclusion, ophthalmic hospitalizations tended towards male bias, short period of stay and were largely for cataract, trauma and glaucoma. Infrastructural development should be considerate of provision of more bed space for males in the ophthalmic wards especially for young adults and children. Personnel capacity development of the ophthalmology team should lay emphasis on the more prevalent needs to enhance effective and efficient management of these diseases. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10010t3.jpg] [hs10010t2.jpg] [hs10010t1.jpg] [hs10010f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}