 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 58-65 Integrating cervical cancer and genital tract infection screening into mother, child health and family planning clinics in Eldoret, Kenya *Were E1, Nyaberi Z 2, Buziba N3 1. Department of Reproductive Health, Moi University. Code Number: hs10011 Abstract Background: Visual inspection, with acetic acid (VIA) and with Lugol's iodine (VILI), has been demonstrated to have
test characteristics comparable to those of Pap smear but are more affordable and easier implement. It also presents an
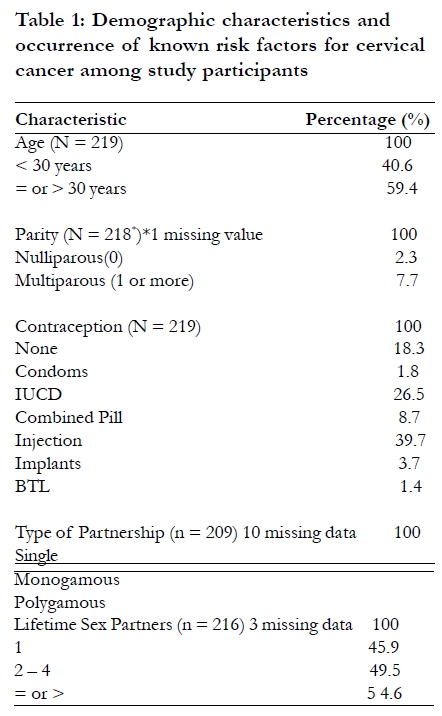
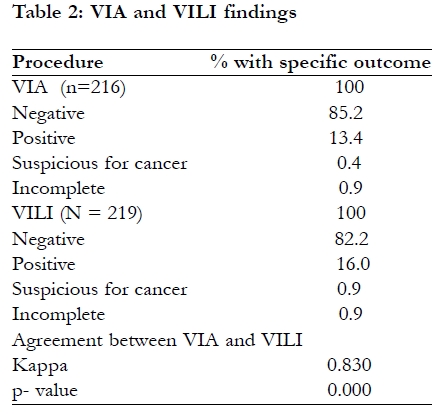
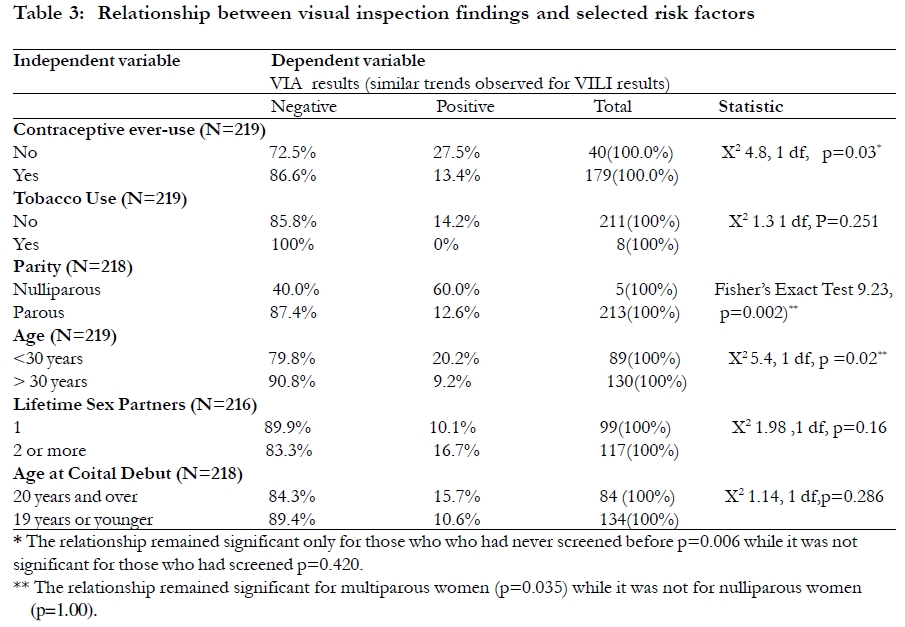
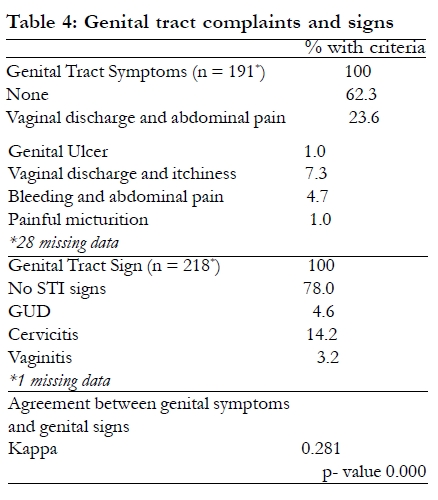
opportunity for management of female genital tract infection. Introduction Cervical cancer is the commonest female genital tract cancer seen at the Moi Teaching and Referral Hospital (MTRH). Over 80% of the cases present to care with stage 2B invasive cancer when only palliative care is feasible1. Besides, the only radiotherapy facilities in Kenya are located in Nairobi further constraining the access to definitive treatment. This situation is replicated elsewhere in Kenya and the developing world. Cervical cancer is a disease whose etiology and natural history is now well understood. The proximate causative factor is infection with high risk human papilloma virus notably types 16, 18, 33, 45. Other apparent, though somewhat controversial, independent risk factors for development of cervical cancer include use of oral contraceptives, smoking, age of menarche, menopause, sexual debut and number of lifetime sexual partners2. In the absence of immunosuppression, the precancerous stages of the disease, represented by low grade squamous intraepithelial lesion (LGSIL) and high grade squamous intraepithelial lesion (HGSIL), follow a predictable course spanning 10-15 years during which the disease is confined to the squamous epitheliumand has not breached the basement membrane. Due to the impact of HIV infection on HPV persistence and clearance, women who are co-infected with the two viruses tend to have a more rapid transition from intra-epithelial lesion to invasive cancer2, 3. Where routine screening is available, as in developed countries, the condition can be discovered in the precancerous stage when a simple, cheap outpatient procedure, such cryosurgery or loop electro-excision procedure, is curative. Such routine population based screening programs have been demonstrated to significantly reduce the incidence of squamous cell carcinoma of the cervix but have relatively less effect on adenocarcinoma4. Pap smear which is the long time mainstay of screening is unavailable in all but the most opportunistic circumstances in the Kenyan health care system, due to its sophisticated manpower and infrastructure requirements. Recently developed simpler approaches using visual inspection with either acetic acid (VIA) or Lugol's iodine (VILI) appear promising and are being adopted in resource challenged settings5,6. While the test characteristics of these visual inspection methods are similar to those of cervical cytology (Pap Smear) they carry the advantage of being simple to learn and implement by middle level health workers, they are relatively more affordable, and allow for the screening results to be availed to the woman same day. To further reduce the risk of loss to follow-up of women with positive test results, strategies that enable treatment to be completed during the same visit the "see and treat" approach have been developed7. Cervical cancer screening presents a unique opportunity to also examine the female genitalia for genital tract infection. Currently, these are treated based on symptoms which are grouped as syndromes with clear guidelines on how to recognize and treat each syndrome. The syndromes include: vaginitis, cervicitis, PID, genital ulcer disease. Clinical examination allows identification of cases where there are clinical signs but the patient has no symptoms or does not recognize their significance. Available evidence shows that genital tract infections are fairly common but their identification is hampered by the fact that, especially among female populations, the infections can be quiescent. Even where there are symptoms, women tend to not volunteer the information to health providers unless specifically probed for the symptoms8. The MCH-FP clinic is a setting that offers the opportunity for the health provider to add value to the visit for the woman through cervical cancer screening and also identification and treatment of any co-existing genital tract infections. Treatment of such genital tract infections could be beneficial in many ways including a reduction in HIV transmission rates. We carried out a pilot project to explore the issues related to the possible adoption and implementation of cervical cancer screening by visual inspection at MTRH and its catchment area. In this paper, we report on the characteristics of participants in the pilot project that aimed at integrating cervical cancer screening using visual inspection approaches with identification and treatment of common genital tract infection syndromes in the setting of on-going Maternal and Child Health and Family Planning (MCH-FP) services at MTRH. Methods Study design This was a cross sectional descriptive study with the goal of drawing lessons from the typical programmatic environment in which a broader visual inspection screening program could be implemented. Setting The study was carried out between May 2005 and January 2006, at Moi Teaching and Referral Hospital. MTRH is Kenya's second national referral and teaching hospital and is located in the town of Eldoret, in the North Rift Area of Western Kenya. The hospital hosts a Maternal, Child Health and Family Planning (MCH-FP) clinic for reproductive health services including family planning combined with the well baby clinic. Our study population was derived from women accessing this clinic either for well baby services or family planning services. We did not include women seeking antenatal care or immediate postpartum services. Reasons for coming to the clinic (whether for well baby clinic or contraception) were not recorded. Training for study procedure Two nurses working in the MCH-FP unit of MTRH were trained on the technique of VIA and VILI using the curriculum developed by Program for Appropriate Technology in Health (PATH) 20. The training involved three days of didactic training followed by two days reviewing cervigrams incorporating use of VIA and VILI to familiarize the trainees with the interpretation of the gross appearance of the cervix without and with acetic acid or Lugol's iodine applied. The nurses were also trained to recognize clinical features of common genital infections using the same curriculum. One of the authors (EW) then supervised the trainees on the procedure and interpretation of VIA/VILI using patients coming into the MCH-FP clinic of MTRH. Once deemed competent, the nurses were allowed to continue the pilot project work on clients coming to the hospital for family planning and well baby services. Study population The study population consisted of women seen at the MTRH MCH-FP clinic either for family planning services or well baby clinic. Women attending the clinic were invited to participate in a questionnaire survey about previous cervical cancer screening experiences, their perception about risks of developing cervical cancer and issues related to access to the screening services. The questionnaire survey was conducted by a suitably trained female research assistant who normally did not work at the MCH-FP. The results of the questionnaire survey will be reported in a subsequent paper. Women consenting to participate in the questionnaire survey were invited to have free cervical cancer screening using the visual inspection approaches of VIA and VILI. The women were informed of the various available approaches including VIA and VILI and informed that the latter technique while cheaper than Pap smears was still being evaluated. Those consenting to have VIA/VILI were then subjected to the procedure as part of the pilot project. The project did not offer women Pap Smear test but they were free to access it at a hospital for a prescribed fee, if they so wished. All women attending the MCH-FP clinic were approached and offered the opportunity to participate. Cervical cancer ccreening procedures In this study women had both VIA and VILI procedures. Due to the staining characteristics, VILI was performed after VIA. VIA procedure With the patientin lithotomy position, the cervix was exposed by use of a single use disposable bivalve speculum. 4% acetic acid was applied to the cervix. One minute later, the cervix was visually inspected, under bright illumination, for the presence of discrete aceto-white lesions near to or abutting the transformation zone. The nurses conducting the screening procedure marked the location of the lesions on a diagram of the cervix for records. Where the squamo-columnar junction could not be clearly identified, the procedure was recorded as incomplete. VILI procedure The same activities were carried out as described in the VIA procedure except that instead of applying acetic acid, Lugol's iodine was used. The precancerous lesions appeared as saffron yellow discrete patches in the background of mahogany brown staining normal epithelia, near to or abutting the transformation zone. Again the lesions were documented as described under VIA procedure. Screening for genital tract infection signs Apart from the cervical cancer screening procedures, the nurses were required to examine the lower genital tract (vulva, vagina and the cervix) in all participants and record all inflammatory abnormalities including discharges, ulcers and any other evidence of inflammation before embarking on the VIA or VILI procedure. The nurses had been trained to recognize these abnormalities using the PATH manual for visual inspection. No laboratory microbiological evaluations were performed. Ethical considerations The study was approved by the ethical committee of MTRH and permission to carry it out granted by the Director of MTRH. Only women providing written consent participated and only de-identified participant information was used for research purposes. The linked screening information was used for referral for follow-up and treatment as needed. All subjects and their partners with clinical evidence suspicious for genital tract infection were offered treatment using the syndromic management protocols in the STI clinics already functional in the hospital. VIA and VILI positive cases were referred to MTRH Colposcopy clinic for further evaluation. Colposcopically directed cervical punch biopsies were obtained if the abnormal visual inspection findings were still persisting during the visit to the colposcopy clinic. The biopsies were only obtained if the participant gave a separate written consent for the procedure. The tissues were sent for histopathologic examination by the pathologist (NB) in the team. The histopathologic confirmation was further constrained by the fact that patients were expected to pay for the service according to the existing hospital cost-sharing policy. Those with confirmed cervical lesions were referred for definitive management at the MTRH Gynecology clinic. Data analysis and presentation Data was entered into an SPSS data base and analyzed by determination of proportions and simple cross-tabulations between variables. Chi-square statistic was calculated for the cross-tabulations, where appropriate, with significance declared at a p-value of <0.05. All the p-values were two sided. Agreement between various VIA and VILI and between clinical signs and presence of genital symptoms was assessed by use of the Kappa statistic and the p-value. Results Between June 2005 and January 2006, we invited 435 women accessing the well baby and family planning services at the MCH-FP clinic at MTRH, Eldoret into the project. Of these, 219 women accepted while 216 women declined to participate in the pilot project. The 219 women who accepted to participate form the basis of our paper on the prevalence of abnormal visual inspection findings and on the frequency of genital tract infection. Table 1 presents the demographic characteristics and occurrence of known risk factors for cervical cancer among study participants. The participants had a mean of 31.3 years with a standard deviation of 6.8 years. Only 2.3% had not had a child before, while the rest had had at least one child. The mean parity was 3.1 with a standard deviation of 1.9. The traditional risk factors for development of cervical cancer were observed in a substantial proportion of the study participants. Of note was the large proportion (over 54%) of study participants who on self report had multiple sex partners. While use of tobacco was uncommon at less than 4%, sexual debut earlier than 20 years was rampant reported by nearly 62% of participants. The high rate of contraceptive use was not surprising since this was a selected population derived from the MCH-FP clinic. Table 2 shows the VIA and VILI findings for the participants who accepted visual examination screening. 13.8% of participants had positive VIA results with 0.4% or one participant being suspicious for cancer while 16.9% had positive VILI results with 0.9% or 2 participants with suspicious for cancer. Of the 40 participants who had positive VIA and or VILI, 24 accepted to undergo further evaluation with colposcopic examination. Fourteen of these had negative examination, 6 had low grade squamous intraepithelial lesion (LGSIL) and 3 had high grade squamous intraepithelial lesion. These participants were referred for further evaluation and treatment at the gynecology outpatient clinic of MTRH. The rest of the participants (195) had negative visual examination findings and were thus not invited to undergo colposcopic evaluation. VIA and VILI showed "very good agreement" in identifying abnormal visual inspection findings, Kappa =0.830, p = 0.000. Table 3 shows that women who had never used contraception were significantly more likely to have a positive visual inspection test result both by VIA and VILI (p=0.03). This relationship remained significant for women who had never had cervical cancer screening before (p=0.006) while it was not significant for women who had screened for cervical cancer before (p=0.420). Further, significant associations were identified between abnormal visual inspection findings and parity and between abnormal visual inspection findings and age. Unexpectedly, 60% of nulliparous women compared to 12.6% of multiparous women had abnormal visual inspection findings(p=0.002). Similarly, 20.2% of women aged less than 30 years compared to 9.2% of women older than 30 years had abnormal visual inspection findings (p=0.02). The association between age and parity was considered potentially confounded by their individual relationships with visual inspection findings. The relationship between age and VIA finding only remained significant for multiparous women (Fishers Exact 4.904, p=0.035) while it disappeared for nulliparous women (Fisher's Exact 0.667, p=1.00). Table 4 shows that about 38% of the participants had genital tract symptoms. The commonest genital complaint was vaginal discharge and abdominal pains reported by 23.6%. When the participants were examined, signs related to STIs were identified in about 22% of all participants. The commonest sign recorded was evidence of cervical inflammation cervicitis. There was "fair agreement" between clinical examination findings for genital tract infections and genital complaints for the same, Kappa =0.281, p=0.000. Discussion We examined the feasibility of integrating the cervical cancer screening, using VIA and VILI, and clinical evaluation of participants for genital tract infections into existing MCH-FP services at MTRH. The participants were drawn from a population that was sexually active. However, it is significant that 54% of the women reported having more than 1 life time sex partners. Given the likelihood of social desirability bias in self reports, it is conceivable that the true figures are much higher and therefore this was a population with a critical risk factor for development of, not only cervical cancer, but also of acquisition of other genital tract infections, including HIV. This was even more significant given a very low rate of self reported condom ever-use of less than 2%. Another participant risk factor of interest was the age at sexual debut. Up to 62% of the participants had commenced sexual activity before the age of 20 years. The early sex debut may in itself lead to multiple partners before the woman is married. Smoking was an uncommon independent risk factor for cervical cancer observed in this study population. There is evidence to suggest that demographic and lifestyle related risk factor profiles are correlated with risk of high grade intraepithelial lesions to a degree comparable to use of molecular hybridization assays for HPV screening and may be a simple and economical alternative9. The finding, in our project, of a significant relationship between positive visual inspection findings and contraceptive never-use and lack of previous screening suggests that targeting screening naïve women might lead to a high yield of abnormal cervical findings. We also found a significant relationship between multiparity and positive VIA findings after controlling for age. Taken together, these significant relationships suggest that women, who were multiparous, perhaps due to contraceptive never-use, were more likely to have positive VIA findings if they were younger than 30 years and had not had any previous screening. This observation is driven, first, by the fact that younger women were less likely to have previously screened compared to over 30 year olds (18.5% vs 81.5% of those reporting previous screening X2 6.247 p=0.012 (data not presented). Secondly, younger and multiparous women are likely to have been sexually active earlier and hence at higher risk. We found a VIA test positivity rate of 13.8% while VILI test positivity rate was slightly higher at nearly 17%. There was "very good agreement" between the two screening methods. These figures are comparable with those reported in other studies that showed VIA positive rate of 13.2% in Ghana7 and VIA positive rate of 16.1% and VILI positive rate of 16.4% for pooled data of five African country studies and one Indian study involving 56,939 women 25 65 years10. It is recognized that while VIA and VILI have high sensitivity for identifying both low and high grade squamous intraepithelial lesions, they are relatively less specific, compared to cytology, and hence, ideally, there is need for confirmatory testing10,11,12. Colposcopic examination and directed biopsies for confirmation of VIA or VILI positive lesions is constrained by lack of infrastructure, personnel, cost of the procedure and fear of the procedure by patients. We only offered colposcopic evaluation to participants with positive visual inspection results as it was not our goal to assess the VIA or VILI test validity in this project13. Only 60% (24 of 40) of the participants accepted to undergo colposcopy. Of the 24 participants accepting colposcopy, 9 (37.5%) had squamous intraepithelial lesions 6 LGSILs and 3 HGSILs. Colposcopic evaluation and directed biopsy was further constrained by low acceptance of biopsy procedure to obtain tissue for the confirmatory histopathological evaluation. Due to the significant attrition in the diagnostic cascade, a one stop strategy of "see and treat" has been recommended for the resource challenged environment7,11. Based on our experience, we are convinced that the "see and treat" strategy would be the rational approach for our setting. We also examined the possibility of integrating genital tract infection management into the cervical cancer screening program. Based on participant complaints, vaginal discharge and low abdominal pain were the most common complaints among the women accepting the screening service. This was reported by nearly 24% of women. The overall frequency of complaints attributable to genital tract infection was about 38%. When the women were examined, the commonest clinical impression attributable to genital tract infection was cervicitis, identified in 14%, while the overall frequency of clinically identifiable genital tract infection was 22%. The clinical finding of a predominance of cervicitis is consistent with vaginal discharge and low abdominal pain as the preponderant participant complaint. Participant complaints appeared to be suggestive of genital tract infection slightly more frequently than clinical impression. There was, however, a "fair agreement" between the genital complains and clinical findings (Kappa 0.281). This suggests that women with genital signs were asymptomatic, a finding in consonance with a high rate of subclinical infections previously reported in a Tanzanian study14 . The glaring limitation of the study in this area was that no microbiological confirmation of clinically suspected genital tract infection was carried out. None the less, these findingare comparable with those from a study in India that reported genital tract morbidity, specifically, pelvic inflammatory disease in nearly 25% of women while STIs accounted for about 10% of the morbidity. Mucopurulent cervicitis and bacterial vaginosis were the commonest conditions identified through laboratory evaluation15,16. Cervicitis is a common finding in cases misclassified as a positive visual inspection finding. However, in our study, none of the cases of cervicitis were found to be either VIA or VILI positive. It is clear that by including content related to recognition of clinical features of genital tract infections including STIs in the training on visual inspection procedures for cervical cancer screening, health workers can be empowered to identify and avail treatment for genital tract infections as part of an integrated reproductive health service to women in MCH-FP settings. At the service delivery or technical level, the integration appears feasible. It is recognized that there are substantial policy, and established vertical program demands in terms of reporting and manpower issues that constrain implementation of integration in programmatic settings Conclusion Integration of cervical cancer screening and genital tract infection identification and treatment into the existing MCH-FP appears feasible. Acknowledgement This work received support from AICAD under Contract Number: AICAD/04/A/011. We are grateful to the Director of MTRH for permitting this project to be carried out in the hospital and to the participants for their role in the project. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10011t2.jpg] [hs10011t1.jpg] [hs10011t3.jpg] [hs10011t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}