 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 66-70 Anaemia in pregnancy: associations with parity, abortions and child spacing in primary healthcare clinic attendees in Trinidad and Tobago Uche-Nwachi EO, *Odekunle A, Jacinto S, Burnett M, Clapperton M, David Y, Durga S, Greene K, Jarvis J, Nixon C, Seereeram R, Poon-King C, Singh R. Department of Preclinical Sciences, Faculty of Medical Sciences, The University of the West Indies, St. Augustine,
Trinidad and Tobago Code Number: hs10012 Abstract Objective: To determine the prevalence of anaemia in antenatal clinic attendees; to investigate the effects of parity,
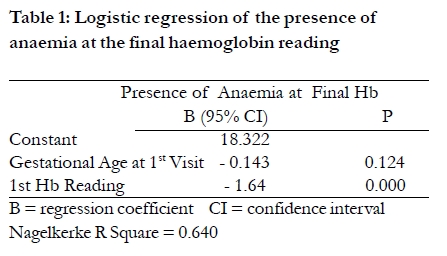
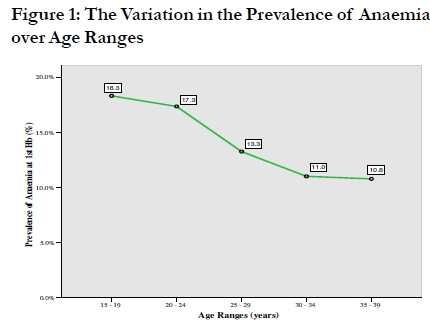
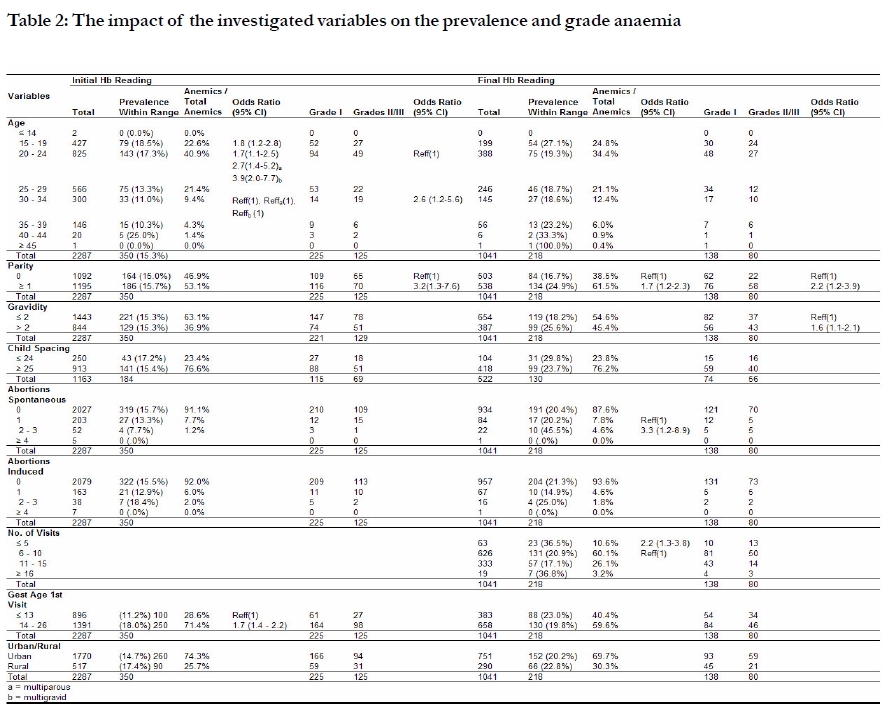
age, gravidity, previous abortions, child spacing and other factors on the prevalence of anaemia in pregnancy. Keywords: Anaemia, Pregnancy, Prevalence, Risk factors, Trinidad and Tobago Introduction Pregnancy is a period of drastic physiological change which places extreme stress on various systems of the body. Approximately 51% of pregnant women are anaemic before delivery1. Anaemia in pregnancy has a multifactorial aetiology2 and has been found to be associated with a higher risk of prolonged labour, abnormal delivery and low birth weight3. The World Health Organization identifies anaemia in pregnancy as a haemoglobin (Hb) reading of < 11.0 g/dl. However, an Hb reading of < 10.0 g/dl is the level widely utilized at health centres throughout Trinidad. Additionally, it is the point at which a patient is likely to become symptomatic and at which therapeutic intervention becomes critical4 Records from the public healthcare centres were used since the majority of the births in Trinidad and Tobago (86.5%, Central Statistical Office (CSO) 2000), occur in the public healthcare system. Thus, trends found can be applied to the majority of the pregnant population of the country. The last study of anaemia in pregnancy in Trinidad and Tobago was conducted forty years ago by Chopra et al who identified a prevalence of 34%5. This present study sought not only to update this prevalence but to also identify the risk factors for anaemia in pregnancy and assess the degree to which certain risk factors contribute to this condition. Methods For this retrospective cross-sectional study the target population was antenatal patients in the primary healthcare system in Trinidad and Tobago during the period January 2000 to December 2005. Those with first haemoglobin estimations after the end of the second trimester were excluded. A multistage sampling method was used to represent the distribution of the pregnant population of women in the public health system in Trinidad. Forty clinics were randomly selected across the eight Community Health districts. The number of health centres sampled in each county reflected the countrywide distribution of clinics by county. The sample was also representative of the urban and rural (CSO definition, 2000) distribution of health centres in each county. Furthermore, in each county the quantity of records sampled was representative of the national proportion of antenatal attendees. Records were then divided based on the urban to rural record ratio within the county. Within the urban and rural classifications the records were equally distributed. No further weighting proportions were done as populations within a given clinic classification were considered to be similar. Finally, equal numbers of antenatal records were taken from each year. A sample size of 2117 was calculated (95% CI; w = 0.03; prevalence of anaemia, p = 14.5%). The actual sample collected was 2287 records. The variables recorded and analyzed were Hb and PCV levels, age, county, child spacing, date and gestational age at: first visit, Hb and PCV readings, and the number of: clinic visits, pregnancies, abortions and living children. Potential confounders considered included race, socioeconomic status, chronic infections, chronic renal disease, bleeding or haemoglobin disorders, eating disorders, dietary differences, substance abuse, private clinic visits and gestational age at prior abortion. These variables as well as demographic data concerning marital status, occupation and religion were not consistently available in the records. Analysis was done using Statistical Package for Social Sciences v. 15.0. Variables were investigated for their association with the presence and grade of anaemia. In order to assess the degree of anaemia among anaemic persons for the variables investigated, grades of anaemia were statistically classified as: Grade I: 9.0-9.9 g/dL; Grade II: 8.0-8.9 g/dL; Grade III: d" 7.9 g/dL. Means, standard deviations, chi-square tests (á = 0.05) and odds ratios were calculated. Where relationships were found, a backward stepwise method was used to perform a binary logistic regression for the presence of anaemia. Results There were 350 cases of anaemia at the first Hb reading (Grade I: 64.3%; Grade II: 25.4%; Grade III: 10.3%). The prevalence of anaemia at the first Hb reading, i.e. the national prevalence, was 15.3 % (95% CI 13.4%, 16.6%). At the final Hb reading, the prevalence was 20.9 % (95% CI 18.4%, 23.4%). The annual prevalence of anaemia at the first Hb reading did not vary significantly (p= 0.484). The mean (SD) of the first Hb reading was 11.3 g/dL (1.5). In the model as shown in Table 1, the first Hb reading and the gestational age at first visit were useful predictors for the development of anaemia by the final Hb reading. Only 46% of the sample had final Hb readings, with a mean (SD) of 11.0 g/dL (1.4). Twelve percent of the women who were not anaemic at admission developed anaemia. Of those initially diagnosed with anaemia, 195 cases (55%) had subsequent Hb readings. One hundred and thirteen (58%) of these remained anaemic at their final Hb reading. It was more likely to resolve anaemia than to develop it by the final blood profile (OR 5.17 95% CI 3.64, 7.33). The county or clinic type (urban or rural) did not affect the presence or grade of anaemia. Nariva/Mayaro County had the highest prevalence of anaemia whereas St. George East County had the lowest (22.3% (95% CI 14.8%, 29.8%); and 12.9% (95% CI 9.0%, 16.8%)). The prevalence of anaemia in rural and urban clinics was 17.4% (95% CI 14.1%, 20.7%) and 14.7% (95% CI 13.0%, 16.3%) respectively. The mean age of women for this study was 24.8 years (95% CI 24.6-25.0). The prevalence of anaemia at the first Hb reading decreased with age as indicated in Figure 1. At the first Hb reading, there was no significant difference between the prevalence of anaemia in women aged 15-19 and 20-24 (p = 0.608), but women in each of these age groups were more likely to have anaemia than 30-34 year olds. However, the grade of anaemia increased with age at the first Hb. 30-34 year olds were more likely to have Grades II to III anaemia at the first Hb reading than 20-24 year olds. These associations were maintained when controlled for parity and/or gravidity. Parity had a mean of 1.0 birth (95% CI 0.9, 1.1). At the final Hb reading parous women were more likely to have anaemia than nulliparous women. At both Hb readings, the grade of anaemia increased with parity. An anaemic woman with at least one previous birth was more likely to have Grades II to III anaemia, than a nulliparous anaemic woman at first and final Hb readings. Gravidity had a mean of 1.4 (95% CI 1.3, 1.5). At the final Hb reading the presence of anaemia increased with gravidity such that a multigravid or grand multigravid woman was more likely to be anaemic than a primigravid or secundigravid woman. The mean child spacing was 57.3 months (95% CI 54.9, 59.6). At the first Hb reading, the mean child spacing for anaemics was about 11 months less than that for non-anaemics [46.7 months (95% CI 41.2, 52.3) and 58.2 months (95% CI 55.2, 61.3)] Child spacing was not associated with the presence or grades of anaemia at the first (p = 0.500; p = 0.870) or final Hb readings (p = 0.196; p = 0.303). Of the 618 abortions studied, 55% were spontaneous and 45% induced. The presence of anaemia at the first Hb reading was not associated with spontaneous (p = 0.119) or induced abortions (p = 0.312). No association existed between the presence of anaemia at final Hb and induced abortions (p = 0.400). However, at final Hb reading persons with 2-3 spontaneous abortions were more likely to have anaemia than those who had one. Furthermore, presence of anaemia was not significantly different between persons who had no spontaneous abortions and those who had one (p = 0.963). The gestational age at first visit was inversely related to the presence of anaemia at the first Hb reading. Women whose first visit was during the second trimester (60.8%) were more likely to be anaemic at the first Hb reading than those who had their first visit during the first trimester (39.2%) The mean number of clinic visits was 7.9 (95% CI 7.8, 8.0). The presence of anaemia at final Hb reading decreased with the number of visits. At the final Hb reading, a woman with 5 or fewer visits was more likely to have anaemia than a woman with 610 as shown in Table 2. Discussion The prevalence of anaemia in pregnancy in women attending primary healthcare centres in Trinidad and Tobago (January 2000 to December 2005) was 15.3% (95% CI 13.4%, 16.6%). This prevalence decreased by 18.7% from the 34% reported in 1967 by Chopra et al5 and can be attributed to advancements in the quality of antenatal care and living conditions. Further research would be required to identify aetiology. It was more likely to find 15-19 or 20-24 year olds with anaemia at the first Hb reading than 30-34 year olds. Likewise, studies conducted in the United States of America (2005) have alluded to an inverse relationship between age and anaemic status up to the age of 356. Conversely, women of all ages were equally susceptible to anaemia in pregnancy by the final Hb reading, as no association was found between age and final anaemic status. At the final Hb reading, it was found that women with at least one previous birth or pregnancy were more likely to have anaemia than women without any. This suggests that the behaviours and attitudes of pregnant women with children may differ significantly from those of nulliparous women with respect to the current pregnancy. However, no association was found between the prevalence of anaemia at the first Hb reading and parity or gravidity, contrary to the findings of a 1993 South-western Ethiopia study7. No association was found between child spacing and the prevalence of anaemia. Analysis may have been affected by the limited cases with child spacing of less than two years. However, a study in Westmoreland Jamaica (1999) identified child spacing of less than two years as a major factor associated with anaemia in pregnancy8. Further research is required to investigate this relationship in Trinidad and Tobago. Abortion did not affect the prevalence of anaemia. This finding was comparable to a 1979 study in India9. The social stigma attached to abortion may have limited the number and/or types of abortions reported. Despite this, there was a positive correlation between the number of spontaneous abortions and the likelihood of developing anaemia at final Hb reading. Women who made their first visit in the second trimester were 1.7 (95% CI 1.4, 2.2) times more likely to be anaemic (18.0%) than those who made their first visit within the first trimester (11.2%). It has been reported that women who had their first visit within the first trimester demonstrated higher compliance with recommended antenatal care10. The present study also found that women with 5 or less antenatal visits were 2.2 (95% CI 1.26, 3.76) times more likely to have anaemia at the final Hb reading as opposed to women who made 6-10 visits. Those with more visits may have had more exposure to antenatal services. Although, it was more likely to resolve anaemia than to develop it by the final blood profile (OR 5.17 95% CI 3.64, 7.33), only 42% of the anaemic cases were resolved. This suggests the need for reassessment of the current measures for managing anaemia in pregnancy. Anaemic women with at least one birth were 3.2 (95% CI 1.3, 7.6) times more likely to have Grades II to III anaemia than anaemic nulliparous women. Prior births may deplete maternal iron stores due to the increased nutritional demands of pregnancy and puerperal blood loss11. Moreover, 30-34 year olds were 2.6 (95% CI 1.2-5.6) times more likely than 20-24 year olds to have Grades II to III anaemia rather than Grade I. This may be due to the decrease of serum ferritin values with increasing age 12 and the association between low serum ferritin values and iron deficiency4. Conclusion and recommendation The prevalence of anaemia decreased by 18.7% from 1967 when it was 34%. Despite this positive indication, women under 24 years and those commencing antenatal care after the first trimester are still at a higher risk for developing anaemia. The benefits of early commencement of antenatal care must be advocated in public health education programmes, since a greater proportion of women coming into antenatal clinics late in their pregnancy presented with anaemia. Emphasis should be placed on younger women since they were particularly at risk. Additionally, more efficient antenatal practices and community partnerships must be fostered in conjunction Government policies to further improve antenatal care. Acknowledgements Completion of this study would not have been possible without the invaluable contributions of Professor Omer Mohammed (Chairman of the Ethics Committee of the Faculty of Medical Sciences , U.W.I) for granting ethical approval for this study; the Regional Health Authorities, County Medical Officers of Health, District Health Nurses and staff of the visited health centres for granting access to patient records under their jurisdiction; the Ministry of Health of Trinidad and Tobago for providing preliminary figures; Dr. Legall (Statistician, Department of Primary Care and Community Health) for his advice and Dr. Van Eenwyk for her comments on the initial draft. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10012t2.jpg] [hs10012t1.jpg] [hs10012f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}