 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
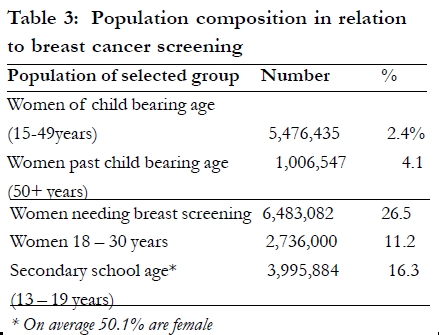
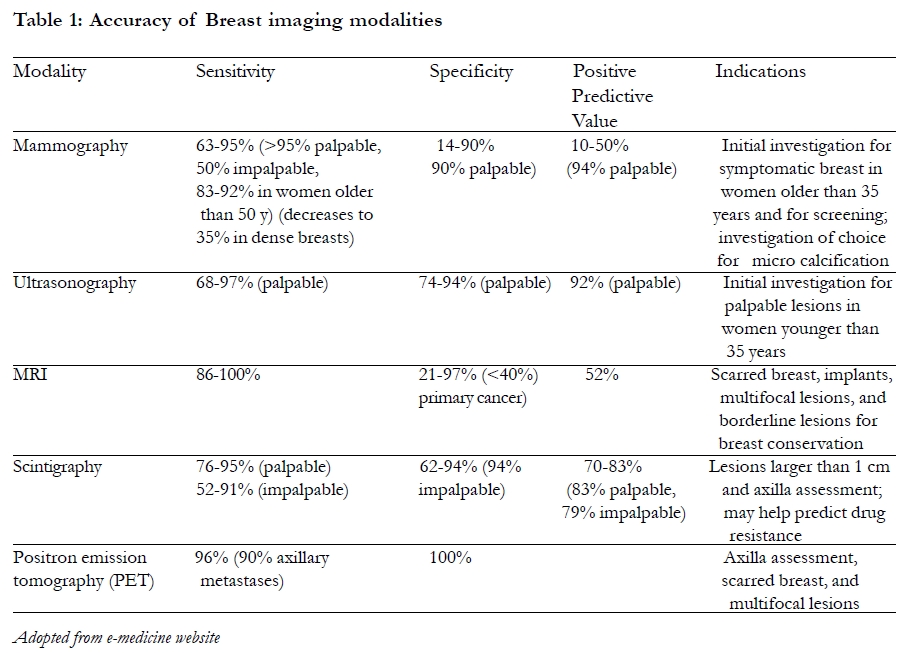
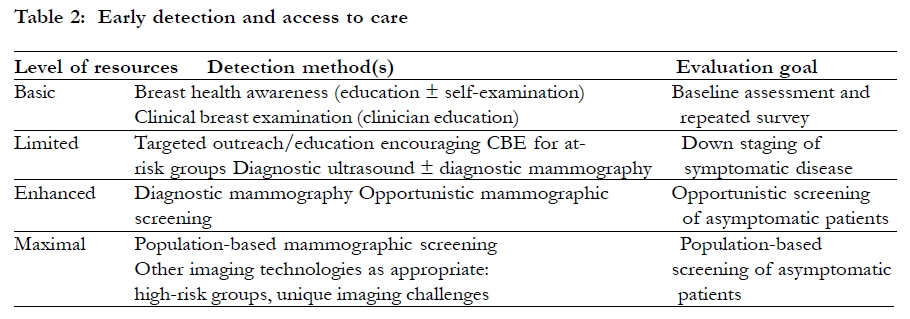
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 89-92 Rethinking breast cancer screening strategies in resource-limited settings *Galukande M1, Kiguli-Malwadde E2 1. Department of Surgery, College of Health Sciences, Makerere University * Correspondence author Dr. Moses Galukande, Department of Surgery, College of Health Sciences, Makerere University, P. O. Box 7072, Kampala, Uganda Email: mosesg@img.co.ug Code Number: hs10016 Abstract The incidence of breast cancer in sub-Saharan nations is increasing. There is a worsening scarcity of Human Resource for Health in Uganda in particular and Sub Saharan Africa in general. Resources available for health care are predominantly spent on infectious disease care such as (HIV/AIDS, Tuberculosis and Malaria). These factors and more make the future of breast cancer care including screening in Sub Saharan African grim. Although mass breast cancer screening by mammography has been proved to be efficacious in the developed nations of the world, this has not been replicated in the developing nations because mass screening is not yet possible for the reasons stated. This paper proposes an alternative to mammography mass screening. Breast health programs for the most part are adhoc or non-existent in Uganda. The challenge of mass screening is not only limited to less readily available mammogram machines and trained human resources but also to the fact that the targeted population is of relatively young women in their 30s, implying that screening should commence earlier than it is practiced in nations where breast cancer peaks among women in their 50s. Mammography is not efficacious in young women with dense breast tissue. Ultra sound scans are not only up to 10 fold more available than mammography machines but are half the cost per examination. Although using ultra sound Scan for screening for non-palpable lumps is not up to par with standard breast cancer care mammography. It may be better than nothing, may be beneficial in aiding early cancer diagnosis. This concept is akin to the `task shifting' advocated by WHO. It is worth investigating use of ultra sound scan for mass screening for breast cancer in resource-limited environments. This is not in any way lowering standards of oncologic diagnosis but filling the otherwise unattended to gap, the unmet need. Key words: breast, cancer, screening Introduction The use of mammogram in screening for breast cancer is a well established efficacious practice that is responsible for significant reduction of late presentation of breast cancers in women in the developed nations of the world1, 2. This practice of mass screening has been so effective that it is been strongly recommended for use in the developing nations and many work and look forwards to the day this will be possible. However it is difficult to predict when exactly this will be, yet there is an urgent need to screen as evidenced by increasing rates of up to 5% per year 3, 4. The emerging picture Breast cancer in sub-Saharan Africa runs a very aggressive course and has higher fatality rates compared to those in the western world; breast cancer occurs 10-15years earlier in black women compared to their white counter parts6, 7, 8 a similar story is found among UK's Black women9. The resources available for Health Care in general are far less than the $ 15 per person per year recommended to governments by WHO as the minimum. Overall projections indicate a worsening picture of cancer epidemiology for the developing nations of the world, in terms of incidence and mortality10. In a recent Ugandan study11 the peak age for patients with breast cancer in Uganda is 30 -39 years, the majority of patients 77% presented late as stage III and IV. The incidence rate is going up in Uganda; it has tripled in the past three decades from 11 per 100,000 to 39.2 per 100,00012 while it has levelled out and now mortality is decreasing in North America and Europe. Constraints Mammogram screening may not be wholly appropriate, since close to half of Ugandan women who need screening are 30 years and below (see Table 3 ). The average age for Ugandans is 15 years13. Mammography is generally not recommended for women below 35 years because women of this age and younger tend to have denser breasts making it more difficult to distinguish abnormal from normal tissue on the x-ray film8. For this reason mass screening is not entirely possible with mammogram use alone since nearly half of the eligible women would be left out because they are below 35 years. Only four mammogram machines exist for a population of 6 to 7 million eligible women (see Table 3) 11, 13. Three of which are privately owned and attract a fee of $ 25 per examination, a cost unaffordable by the average Ugandan woman or the government for that matter. The cost of a breast ultrasound scan is a little less than half the cost of a mammogram in the private sector. We may need to use the task-shifting concept5, can we then have USScan take on the task for screening, and can we take it away from the radiologist to the sonographer (non physician health worker)? Sonographers are less expensive, more likely to accept deployment out of the capital city, even though additional training for breast screening may be necessary. There are atleast 30 radiologists in Uganda making a radiologist to patient ratio of (1:300,000) and at least 60 sonographists making a ratio of 1:150,000 14. USScan may have a relatively low sensitivity and specificity (see Table 1) but this would be better than no screening at all. Isn't it prudent then to use it in the interim until such a time as when mammography will be widely available? But even if mammography were available to all women in Uganda, what about the half for which it may not be appropriate? (Until proven otherwise by research) Limited access to standard screening is a scenario not only unique to Uganda but common within the African sub continent. Global initiatives The Breast Health Global Initiative (BHGI) 15 (Anderson et al, 2006) strives to develop evidence based, economically feasible and culturally appropriate guidelines that can be used in nations with limited health care resources to improve breast cancer outcomes. Table 2 highlights the proposed framework to fit the level of resources available to the different nations. Early breast cancer detection improves outcome in a cost effective fashion assuming treatment is available. The BHGI group recommends future research to better determine the best way to implement guidelines in limited resources settings. Possible country specific initiatives Uganda has close to 2,000,000 girls in the 13-19 age bracket who are in school. The figure shown in Table 3 for secondary school age 13-19years is for both sexes. A little more than half of which are female (50.1%) if these two million girls were to be screened it would not be with mammography. Taking away the burden of imaging from the four available mammography machines to at least 60 US scans that exist in the country and mostly situated in or near district hospitals, is plausible and it is not meant to lower standards of oncological diagnosis but narrow the gap that exists. Using US Scan for screening in this scenario is the major stopgap measure this opinion paper emphasizes. School campaigns for BSE (Breast Self Examination), for all girls are the other possibility16. The feasibility and subsequent impact of this ought to be investigated and documented. Table 1 indicates how the different investigating modalities compare in terms of sensitivity and specifically in places where they are available for use (a western nation). Gathering accurate data about breast cancer in Uganda is critical for problem characterization and subsequent evidence based solutions as indeed recommended by BHGI. Conclusion Breast Cancer screening, as we know is mostly by the use of mammograms; mammograms are few in Uganda as in many sub Saharan poor countries and won't be enough in the foreseeable future to cover the unmet screening need. In the meantime the next best options include use of USScan and Breast Self Examination (though little evidence to support efficaciousness for both is lacking). Other unexplored options in resource limited settings are, task shifting by the involvement of non-physician cadre in Breast Health Care. There is therefore a need to investigate efficacy of ultrasound in breast cancer screening in resource-limited environments as well as a lower cut off age for mammography screening. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10016t3.jpg] [hs10016t2.jpg] [hs10016t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}