 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
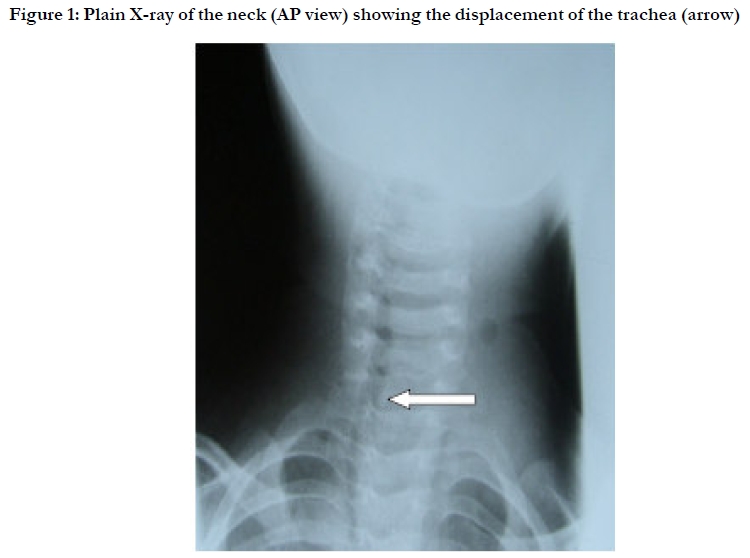
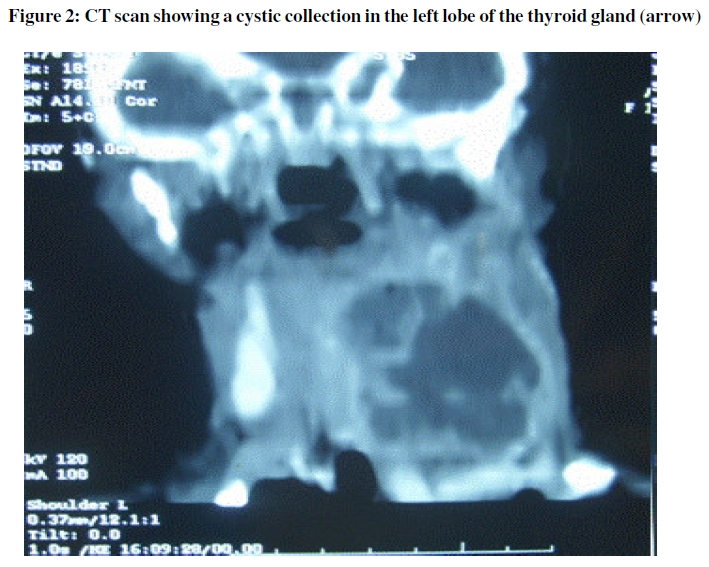
African Health Sciences, Vol. 10, No. 1, March, 2010, pp. 101-103 Case report Unusual cause of thyroid abscess *Adeyemo A1, Adeosun A2, Adedapo K3 1. University of Ibadan, Institute of Child Health *Correspondence author: Adeyemo, Adebolajo, Institute of Child Health, University of Ibadan Email:adebolajo@yahoo.com, aadeyemo@comui.edu.ng Code Number: hs10019 Abstract Thyroid abscess is a rare condition of the thyroid gland. The common causative organisms responsible for thyroid abscess are Staphylococci and Streptococci species. We described a case of thyroid abscess due to Klebsiella pneumoniae in an infant. The patient was successfully treated with open surgical drainage and appropriate antimicrobial agents. Keywords: Thyroid, Abscess, Klebsiella Pneumoniae, Acute Suppurative Thyroiditis Case report A 14 month old female child was admitted with a two week history of high grade fever which did not resolve with use of analgesics or anti-malaria drugs, and an enlarging, painful neck mass. Physical examination showed an acutely ill patient with axillary temperature of 38.4°C, tachycardia, a large tender, warm, and fluctuant anterior neck mass with no further extension. The trachea was shifted to the right. The haemoglobin level on admission was 9.6 g/dl and plain radiographs of the neck and chest in frontal and lateral views showed a homogenous soft-tissue density anterior to the trachea, displacing it to the right. (Figure 1). A cystic non homegenous collection in the left lobe of the thyroid gland was seen on computed tomography scan. This extended into the superior mediastinum without any distortion of the mediastinal structures (Figure 2). Thyroid scintigraphy also showed a cold spot in the left thyroid gland and a retroviral screening for Human Immunodeficiency Virus was non reactive. A diagnosis of thyroid abscess was made and she underwent an incision and drainage procedure under general anaesthesia that yielded 150mls of greenish pus. She was treated with intravenous ceftriazone at a dose of 250 mg twice a day and metronidazole at a dose of 90 mg three times a day. Cultures of the drained pus yielded Klebsiella pneumoniae. After two week course of intravenous antibiotics; she improved symptomatically and was discharged home 14 days after admission. On review at the out-patient clinic she had sustained clinical improvement. Discussion Acute suppurative thyroiditis (AST) is a rare clinical event1 and an uncommon form of thyroiditis2. The progression of the condition to thyroid abscess is equally unusual3. Both AST and thyroid abscess represent 0.1 to 0.7% of thyroid lesions managed surgically.4 A tender thyroid lesion is the hallmark of AST but other causes of a tender thyroid includes de Quervain thyroiditis (the commonest cause of a painful thyroid), acute hemorrhage into a cyst or thyroid nodule, a rapidly enlarging thyroid carcinoma, or radiation thyroiditis 5,6. The thyroid gland possesses some characteristics that help to make thyroid abscess an uncommon clinical event. These include: total encapsulation of the gland, its secluded anatomic position, an iodine-rich environment, extensive lymphatic drainage, and good blood flow from bilateral anatomising superior and inferior arteries. These provide protection by hindering the invasion of bacteria and its subsequent growth. Haematogenous spread from a distal site of infection is believed to be a common cause of thyroid infection; however the exact infectious source or pathway is frequently unknown. In our patient the exact cause of infection was not known. Congenital thyroid gland pathology such as pyriform sinus fistula can also lead to acute suppurative thyroiditis3 other causes includes trauma such as fine-needle aspiration7 and foreign bodies. None of this was however demonstrated in the index case. AST has also been associated with immunosuppression, especially human immunodeficiency virus 6, however a retroviral screen in our patient was negative. Although Staphylococci and Streptococci have been described as the most frequent causes of AST,7 many other organisms such as Aspergillus, Brucella, Klebsiella, Eikenella, Salmonella, and Acinetobacter have been identified in infection of the thyroid gland and oftentimes the infection is polymicrobial.6 Thyroid abscess have been observed to be more usual in females than males7 with a wide age range of 16 days to 79 years,8 with the left side of the gland more commonly involved. Our patient is 14 months old and she developed the lesion on the left side,but the reason for the commoner involvement of the left lobe is not known. Thyroid abscesses usually start after upper respiratory tract, pharynx, or middle-ear infections.9 Clinical signs include tenderness of the gland, dyspnea, pain, hoarseness, dysphagia, fever, and chills. The unexplained fever which did not resolve despite usage of analgesics or anti-malaria drugs might have suggested the onset of AST in our patient. Although some patients may be asymptomatic laboratory results indicating infection such as leukocytosis, elevated erythrocyte sedimentation rate and thyroid scintigraphies showing hypo-functional areas with reduced uptake, may also be present.10 Plain x-rays of the neck may show tracheal displacement, ultrasonography and computerized tomography may identify the underlying structure and extent of the abscess. A fine-needle aspiration to confirm the diagnosis of thyroid abscess and to determine the responsible organism and its antibiotic susceptibility can be performed. The management of a thyroid abscess is surgical, consisting of incision and drainage, combined with culture and appropriate antibiotic therapy. Broad-spectrum antibiotic therapy covering aerobic, anaerobic, and oral flora should be started early after obtaining a specimen for microbiological studies and this can be changed when sensitivity profile is available. Complications such as destruction of the thyroid or parathyroid glands, internal jugular vein thrombophlebitis, local or hematological spread to other organs, sepsis, and even abscess rupture or fistula formation into the esophagus or trachea can follow thyroid abscess.9 The index case was caused by Klebsiella pneumoniae. K. pneumoniae is a common hospital-acquired pathogen though it may also be a community-acquired pathogen. Only four other cases of thyroid abscess due to K. pneumoniae have been reported in the English literature.11 The antibiotic treatment should be based on the antibiotic susceptibility testing of individual isolates. This case exemplifies a rare lesion of thyroid abscess due to an unusual causative agent: Klebsiella pneumoniae. It also illustrates the need for high index of suspicion in cases of fever of unknown origin in children and the relevance of excluding less common causes (such as Gram-negative bacilli like Klebsiella species) in the management of thyroid abscess. References
Copyright © 2010 - Makerere Medical School, Uganda The following images related to this document are available:Photo images[hs10019f2.jpg] [hs10019f1.jpg] |
| |||||||||

{kind=link}
{kind=link}