 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 320-324 A review of compliance to anti tuberculosis treatment and risk factors for defaulting treatment in Sub Saharan Africa *Castelnuovo B Infectious Diseases Institute, Mulago Hospital, Kampala, Uganda *Correspondence author: Dr. Barbara Castelnuovo, Infectious Diseases Institute, Mulago Hospital, Kampala, Uganda, Email: bcastelnuovo@idi.co.ug Code Number: hs10061 Abstract Background: The aim of this study is to assess anti
TB treatment compliance and the factors predictive for poor adherence in Sub-Saharan
Africa in the last 10 years.
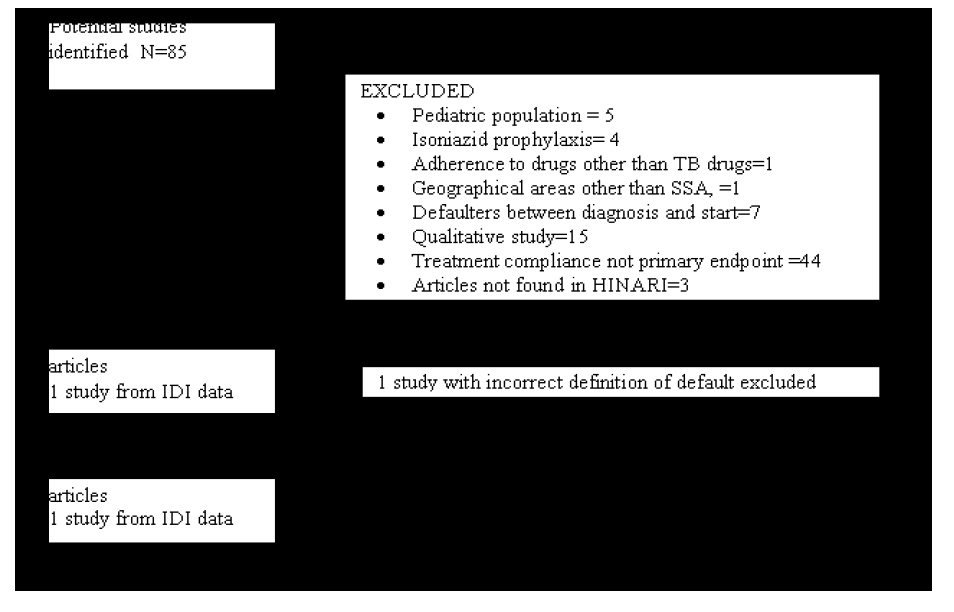
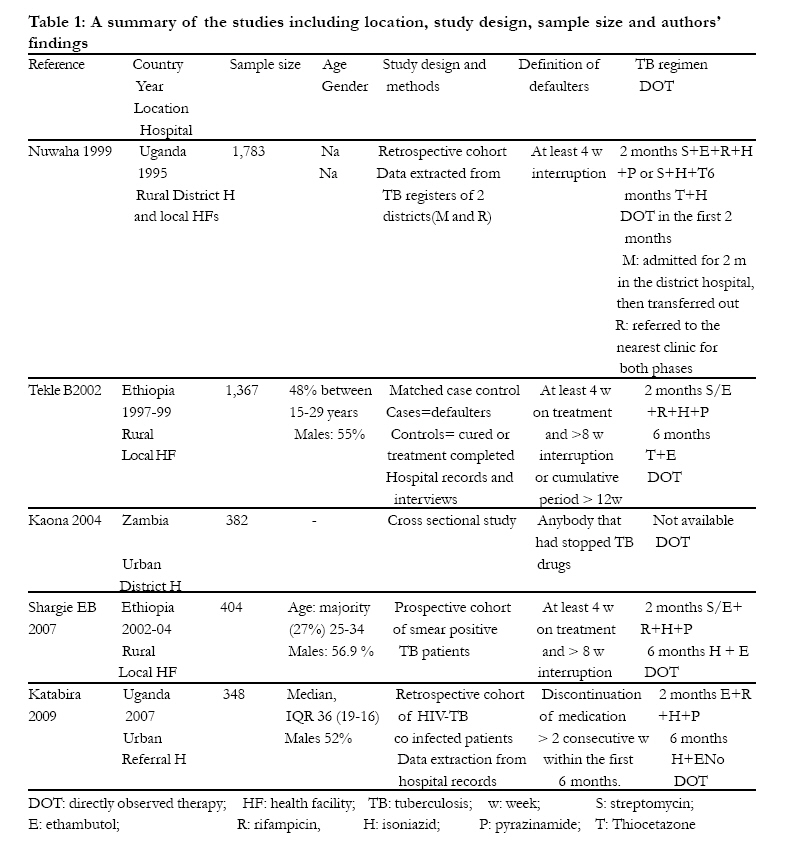
Introduction In 2007, nine miilion new cases of tuberculosis (TB) were diagnosed worldwide, and in the same year TB has killed 1.8 million people1. In Sub Saharan Africa TB cases have markedly increased as a consequence of the HIV epidemic2,3. TB treatment usually consists of 2 phases: an intensive phase with a combination of four drugs for 2 months and a continuation phase with 2 drugs for 4 to 6 months. Drugs used for treatment and the duration of the intensive and continuation phases may vary within TB programs. In Africa the cure rate is lower than the global cure rate (54%-74% in Africa for smear positive pulmonary TB as compared to 84% world wide) due to adherence issues and the emerging of multi-drug resistant strains of Mycobacterium tuberculosis3. Poor compliance and patients defaulting anti TB treatment contribute to the increase of multi-drug-resistant mycobacteria in the continent4. Default is defined by the WHO as a treatment interruption of two consecutive months or more after at least one month on treatment5 but the definition of defaulters can vary within national programs. The aim of this study was to assess anti TB treatment compliance and the factors predictive for poor adherence in Sub-Saharan Africa in the last 10 years. Methods Data sources We searched Medline (http://www.ncbi.nlm.nih.gov/mesh?itool=sidebar ) for articles using the terms: "Patient Compliance"[Mesh] OR "Medication Adherence"[Mesh])) AND "Tuberculosis"[Mesh]) AND "Africa South of the Sahara"[Mesh]. We searched for articles written in English and we restricted the search to articles from the last 10 years (1999 May 2009). Conference abstracts were not searched. Selection criteria Studies were excluded if the population was pediatric, if adherence described in the study regarded tuberculosis prophylaxis, if the adherence evaluated was to drugs other than tuberculosis drugs, if patients were lost to follow up between diagnosis and treatment start, if the research was conducted in geographical areas other than Sub Saharan Africa, if the primary endpoint was not treatment default, if studies were qualitative, and if articles were not found in HINARI. One study from the Infectious Diseases Institute (IDI), Kampala, Uganda, was included; the data was presented at the Implementers Meeting 2009, Windhoek, Namibia, and although the publication did not fulfill the inclusion criteria described above, the author felt this data was valuable, as it was the only study on TB-HIV co-infected patients. Outcome measure We assessed adherence to TB treatment as the proportion of patients defaulting anti TB drugs; we also looked at the factors predictive for non compliance to anti TB drugs. Data abstraction Data abstraction was done by the author. Study characteristics In this review we describe the following characteristics: reference, country and location (urban/rural), type of health facility, sample size, demographics of study patients (age, gender), study design and methods, definition of the primary outcome (treatment defaulter), drugs used, use of direct observed therapy (DOT), proportion of patients completing anti TB treatment, timing of default, risk factors for defaulting treatment. A meta-analysis was not performed because the studies were too heterogeneous and used different definitions of TB treatment defaulter. Results We found a total of 85 published articles. After reviewing the abstracts, 80 papers were excluded: 5 assessed pediatric population, 4 regarded compliance to isoniazid and 1 to drugs other than anti TB drugs, 1 study was conducted in Israel, 15 described patients defaulting between diagnosis and treatment start, 15 were qualitative studies, in 44 treatment compliance was not primary endpoint, and 3 articles were not found in HINARI. We remained with 5 papers and data from the IDI study for a total of 6 studies (Figure 1). One of the papers was excluded after reading it because it had an incorrect definition of defaulters. A summary of the studies including location, study design, sample size and authors' findings are presented in Table 1 Study characteristics Two studies were from Uganda6,7, two from Ethiopia8,9 and 1 from Zambia10. Three studies were conducted in rural areas6,8,9 and two in an urban setting7,10; three studies were conducted in local health facilities6,8,9, one in a district hospital10 and one in the referral national hospital7. Regarding the study design, two studies were retrospective cohorts6,7, one a prospective cohort9, one a cross-sectional study10 and one a case control study 8. The definitions of defaulters were different across the studies, with two studies using the WHO definition8,9 and three studies defining treatment defaulters with more stringent criteria6,7,10. In only one study DOT was not used as the strategy to deliver TB treatment and a treatment supporter was instead used to enforce adherence7. Proportion and timing of defaulting The proportion of patients defaulting varied from 11.3% (8) to 29.6% (6). In four studies the majority of the patients defaulted treatment during the continuation phase6,8-10, while in one study 59% of the patients were lost to treatment during the first 2 months intensive phase7. One study assessed seasonality of defaulting and found an association with the rainy season7. Determinants of default Risk factors for defaulting treatment were: distance from the hospital7,9, not being on the first course of TB medications6, lack of repeated smears (6), unit transfer after the intensive phase6, experiencing side effects8, having no family support8, poor knowledge about TB treatment8, being more than 25 years old9, and use of public transport9. Discussion This review shows overall a high proportion of patients defaulting TB treatment in Sub-Saharan Africa. Four out of the five studies report proportion of default above 20%6,7,9,10 with 3 studies close to 30%6,7,10. The use of DOT6,8,9,10 or the introduction of newer, better tolerated regimens in the last years7,9,10 don't seem to improve this alarming rate of patients defaulting TB treatment. The studies used different definition of defaulters. Of note, the studies that used the WHO definition of TB treatment defaulter, registered a lower rate of defaulting8,9. The WHO definition, (being off drugs for more than 8 weeks after completing at least one month of treatment), is an operational definition to guide health workers in the decision of using a re-treatment/second line regimen if the patient comes back to the health facility after defaulting; three studies found this definition not enough stringent and formulated their own definition of treatment default, resulting in higher proportion of patients defaulting6,7,10. In most of the studies the majority of the losses to follow up occurred during the continuation phase6,8-10; only the study by Katabira et al7 shows that most of the patients default during the intensive phase. This could be explained by the fact that this study was conducted in a clinic in the national referral hospital; many patients discharged from the wards, if HIV positive, are referred to the clinic for treatment. It is likely that the patients that come from other areas, after starting the treatment and getting healthier, move back to their original location without informing the clinicians and getting referral forms. Four studies looked also at risk factors for treatment default7,7,9; each study included different characteristics, therefore the factors identified are heterogeneous. A big role in this rate of patients lost to follow up is distance, money for transport or logistic in referring and transferring patients6,7,9; other challenges in adhering to treatment are side effects, poor knowledge of the disease and insufficient family support9. This study has several limitations. The search was restricted to English written papers and abstracts of conferences were not searched. After searching, studies that were not available through HINARI were also excluded; we attempted to obtain the manuscripts from the John Hopkins University Library with no success. Also, due to the heterogeneity of the TB programs, the study designs, and findings on risk factors these results cannot be generalized. There is need for new research studies with the main aim of identifying risk factor for defaulting TB treatment. Conclusion This review of studies on patients' adherence to TB treatment reveals high rate of losses to follow up in Sub-Saharan Africa; the information currently available is too heterogeneous to draw conclusions on the reasons for this high rate of defaulters. It is imperative to understand predictive factors for treatment default so that programs can implement specific measure to target the population at risk, since other strategies such simpler treatment regimens and DOT have not given enough satisfactory results. Since distance from the clinics plays a big role in influencing adherence to TB treatment, national programs should consider making drugs more widely available, by either providing the TB treatment to smaller health centers, or organizing mobile TB clinics, especially in rural areas. Acknowledgement The author acknowledges the organizers of the course in Applied Clinical Research and Evidence Based Medicine (ACREM) for their suggestions regarding the manuscript. References
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10061f1.jpg] [hs10061t1.jpg] |
| |||||||||

{kind=link}
{kind=link}