 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 325-331 Clinical and immunological status of a newly diagnosed HIV positive population, in Marrakech, Morocco *Admou B1, Elharti E2, Oumzil H2, Addebbous A1, Amine M3, Zahlane K1, Soraa N1, Zougaghi L1, Haouach K1, Tassi N4, Aajly L 5, Chabaa L1, El Aouad R2. 1Laboratory of Medical Analysis, University Hospital and
Faculty of Medicine and Pharmacy, Marrakech, *Correspondence author: Brahim Admou, Faculty of Medicine and Pharmacy, Cadi Ayad University, Marrakech, Morocco, Email: b.admou@fmpm.ucam.ac.ma Code Number: hs10062 Abstract Objective: To evaluate the clinical and the immune
status of newly HIV diagnosed patients, in Marrakech city and its neighboring
area, in Morocco.
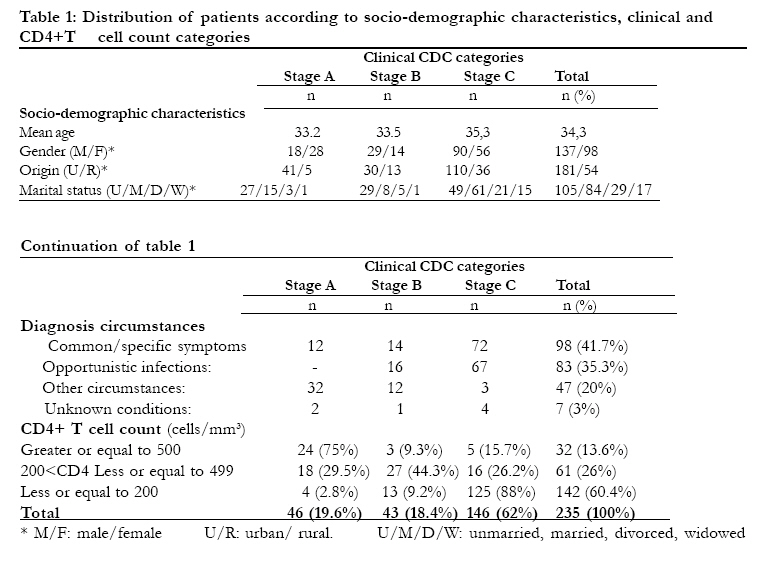
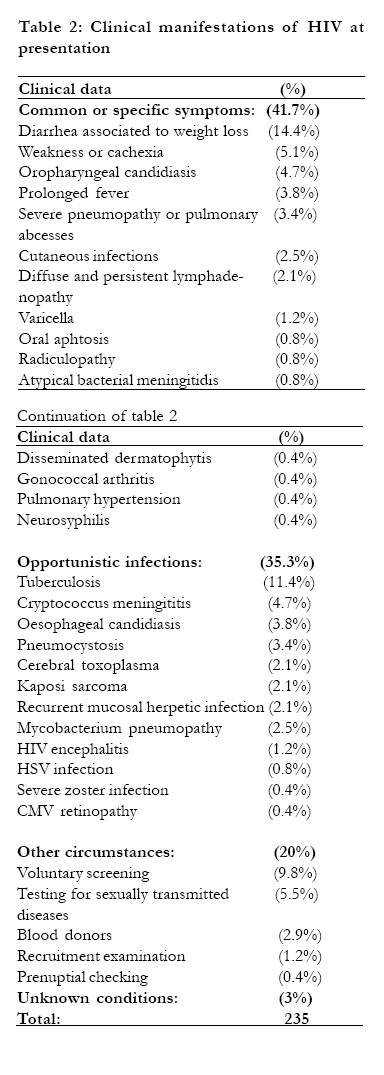
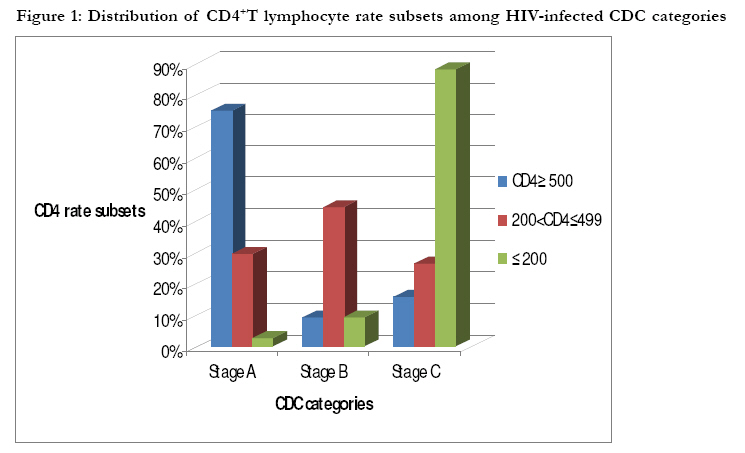
Key words: HIV Infection, CD4T cells count, CDC Classification, Marrakech, Morocco Introduction Human Immunodeficiency Virus (HIV) has a selective tropism for cells which express the CD4+ phenotypic marker: T Lymphocytes, monocytes and macrophages1. The main biological event in HIV infection is the immunity system collapse, especially CD4 T cells gradual destruction that lead to a severe immune depression and consequently a high risk of opportunistic infections and cancers1,2,3. The CD4 count is a useful tool for the initiation and the follow-up of the anti-retroviral therapy response1. The decrease of CD4+ T cells during HIV infection may result from several mechanisms: cytopathogenic effect of the virus on infected cells, CD8+ T lymphocytes mediated cytotoxicity, or abnormality of CD4+T cells distribution or arrest of their renewal2,4. During HIV infection, some authors relate two immunological stages depending on CD4+T cells number: the first stage with less than 400 CD4+T cells/mm3, characterized by a deficiency of mucosal immunity is associated to a deficit of skin delayed hypersensitivity. The second stage with CD4+T cells<50/mm3 includes a systemic immune deficiency, commonly characterized by cytomegalovirus (CMV) and Mycobacterium Avium infections5. Other authors attribute the risk of the opportunistic infections to specific degree of immunosupression6. Thus, herpes simplex virus (HSV), candida and pyogenic infections may occur in asymptomatic persons, while the risk of pulmonary pneumocystis and about 80% of tuberculosis cases increase significantly when the rate of CD4+T cells is less than 200/mm3 6,7. Similarly, non Hodgkin lymphoma and Kaposi sarcoma or Mycobacterium, CMV and toxoplasmosis infections occur typically when the rate of CD4+T cells is inferior to 100/mm3 8,9,10. In Morocco, since the first case of HIV infection has been diagnosed in 1986, there has been a steady increase of HIV/AIDS cases, and currently there is around 20, 000 infected persons.11. The diagnosis is mostly done in severe or acute clinical circumstances, or among risk groups, blood donors, or within voluntary counseling and testing (VCT) facilities. Clinical diagnosis was initially provided in few specialized centres belonging to university hospitals. Since 2004, the HIV screening has been expanded by the introduction of rapid testing in VCT centres affiliated to nongovernmental organizations (NGOs) and within HIV referral centres. Moreover, HIV testing using conventional techniques (ELISA and Western blot tests) was decentralized in 20 regional laboratories. This strategy is aimed at enhancing earlier HIV diagnosis and therefore an early HIV management. In Morocco, Marrakech city and its neighboring area account for 15% of all HIV-infected patients in our country. There are two referral HIV clinical centres, located in the Ibn Zohr regional hospital and in the university hospital center, that are in charge of management of HIV-infected individuals of this area. Furthermore a clinical laboratory, within university hospital centre, which is supervised by the national reference laboratory for HIV, assures the HIV diagnosis as well as CD4 counting. The aim of this study was to evaluate the clinical and the immune status of newly HIV diagnosed patients of this region according to their clinical stages. Methods We performed a retrospective study on 235 newly HIV diagnosed patients, corresponding to all patients admitted over the time between January 2006 and December 2008, within two referral HIV health care centres, located in Ibn Zohr regional hospital and the university hospital centre, in Marrakech. The patients are addressed to the HIV diagnosis and management facilities, since they have symptoms and or risky behaviors. Individuals that screened within the framework of VCT are addressed to these referral HIV care units, as well. The patients mostly came from urban areas and from rural areas. All these patients have been confirmed for HIV infection, within the laboratory of the University Hospital Centre, by using an enzyme immunoassay test (ELISA HIV/1-2, Genscreen plus®) as a screening test, followed by a confirmatory technique i.e. the Western-Blot test (HIV BLOT 2.2 Genlabs Diagnostics®), and patient's samples met the World Health Organization (WHO)13 Western blot test positivity criteria. According to the clinical symptoms recorded during the first visit, data were recorded in the medical file, and HIV specialist physicians used CDC (Centre for Disease Control) classification system12 to categorize the clinic stages for all HIV-infected individuals. Finally, to assess the immune status of these patients, a CD4 count is prescribed at the initial visit, and it is measured within a week following the visit. The measurement is preformed by the FacsCount instrumentation, which gives an absolute count of CD4 T cells/μ l (FacsCount, Becton Dickinson®). Results Seventy seven percent of patients (n=181) came from urban area, versus 33% (n=54) who was originate from rural districts of Marrakech surroundings. The mean age was 34.3± 8,4 years (range:14-55 years), with a slight male predominance (sex-ratio M/F=1.4). The most age range concerned by the HIV disease was 25-34 years (40%, n=94) followed by 35-44 (35.3%, n=83), 45-55 (16.6%:n=39) and 14-24 (8.1%, n=19) years range respectively. Unmarried individuals were the predominant proportion (44.7%, n=105) in this series (Table 1), and homosexual or bi-sexual behavior was noticed in 19 patients (8.1%) versus 206 patients (87.7%) who were generally heterosexual. The sexual status was not declared by 10 patients (4.2%). Furthermore, 38% of patients (n=89) avowed sexual connection with many partners and the age of the first sex could not be significantly determined. Clinically, in 41.7% of cases (n=98), the infection was revealed by various common or specific symptoms, primarily diarrhea with weight loss or cachexia (Table-2). Opportunistic infections were the form of HIV disclosure in 35.3% of cases (n=83), from which tuberculosis was the most frequent. Moreover, the disease has been uncovered in many other circumstances such as voluntary screening at VCT facilities or others similar conditions (Table 2) among 20% of patients (n=47), while, diagnosis conditions could not be reported in 3% of cases (n=7). The clinical data showed that 19.6% (n=46) of patients were diagnosed in stage A, 18.4% (n=43) in stage B, while 62% (n=146) were in stage C of the infection according to CDC classification. We noticed a predominance of female patients among CDC category A (sex-ratio M/F=0.6), and male gender among in B (sex-ratio M/F=2.1) and C (sex- ratio M/F=1.6) categories. Patients originate from rural area were more frequent in category C than B and A categories. Likewise, the proportion of divorced or widowed patients was significantly more important in category C than B and A categories (p=0.01). The CD4 subset immunophenotyping showed that 60.4% of the patients (n=142) had a CD4 rate inferior to 200/mm3 of which 88% were categorized as stage C, 9% as stage B and 3% were included in stage A. In 26% (n=61) of cases, the number of CD4+T cells was between 200 and 499/mm3. Forty four percent fell into category B, 29.5% in category A, and 26.2% in category C. Only 13.6% (n=32) of the patients had a number of CD4 superior or equal to 500/mm3 of which 75% were at stage A, 15.7% at stage C and 9.3% at the stage B (Table 1 & Figure 1). The CD4+T cells average for all the patients was 225/mm3. Discussion The results of this series show that 48% of HIV infected population had less than 35 years, and the majority had symptoms of AIDS disease that indicate the onset or existing opportunistic infections. Also, more than half of patients were diagnosed in an advanced stage of immunosupression linked to HIV disease, since 60.4% of them had less than 200 CD4+Tcells/mm3, 26% had a CD4+T cell number ranging between 200 and 499/mm3 and only 13.6% kept a rate of CD4+ T superior or equal to 500/mm3, with an average of 225 CD4/mm3. As shown in the results, 88% of cases with less than 200 CD4+T cells/mm3 were matching with category C of CDC classification system. In fact, a lower CD4 rate in HIV infected individuals may give evidence that the patient has been infected for a long time as compared to those with higher CD4 count14. However, primary HIV infection can be accompanied by a profound transient lymphocytopaenia including low CD4+T cells, and opportunistic infections may occur at this stage, but these infections should not be confused with clinical staging events developing in established HIV infection15,16. This fact might explain the low rate of CD4+T cells in 4 (2.8%) of patients belonging to category A in our series. Moreover, in acutely HIV-infected patients 46 weeks post-infection, there is usually a depletion of the gut associated lymphoid tissue (GALT) limited to a predominantly CD4+T cell subsets exhibiting a memory phenotype [CD45RA-/CD45RO+]. This depletion is attributed to preferential replication of HIV-1 in the GALT where CD4 are the predominant residing T cells17. Likewise, Diagbouga showed that the early depletion of CD4+T cell is mainly due to a decrease of CD4+CD29 high subset, whereas CD4+CD45RA+ phenotype is unaltered in CDC-A stage of the disease. But, in the later stages (B and C), both CD4+CD29high and CD4+CD45RA+ subsets contribute to CD4 T cell depletion18. In all of cases, individuals with less than 200 CD4/mm3 may have both poorer response to anti-retroviral therapy and worse prognosis than those with higher CD4 count at the time of therapy initiation19. In Morocco, even with the current availability of HIV testing program, expansion of testing in medical settings and VCT centers, the delay in diagnosis was noticed in our population. This might be related to a weak adhesion to these efforts, and to difficulties to access health care system for some populations, especially who come from rural area. A late diagnosis may also be due to a relatively weak knowledge among medical staff towards HIV associated diseases. Moreover, the adverse image of HIV infected person in our society usually leads to some reticence towards both the diagnosis and the monitoring on regular basis. It is worthwhile noting that regarding to HIV epidemic, the HIV/AIDS program department in the Moroccan health ministry has set up a national strategy aimed to curb the epidemic in the kingdom. This strategy primarily encompasses prevention and strengthening of the early HIV diagnosis as well as treatment of HIV-infected patients20. Generalizing free access to HIV testing throughout the country represents the main priority, since 2008. In this regard, and with the efforts of the Moroccan Ministry of Health, the HIV testing is being available in many basic health care points, in Morocco. The results of our study are relatively comparable to some African studies, which also display a delay in the diagnosis of HIV infected patients. Thus, in a Benin study including 136 initially diagnosed and monitored patients between 2001 and 2002, 46.3% of them were in stage C, and 69% of cases had less than 200 CD4 T/mm3 21. Furthermore, a French study carried out in Saint-Antoine hospital in Paris between 2002 and 2003 concerning 300 new cases of HIV infection, from different origins: 43% Caucasian, 44% African, 8% North African and 3% Asian. The average of CD4+T cell was 374/mm3. Only 23.3% of the French had less than 200 CD4/mm3 versus 40% among patients coming from Sub-Saharan Africa. It was concluded that the delay of HIV diagnosis is important among African emigrants in France, and may be favored by cultural and socioeconomic context22. Likewise, a multicenter study carried out in the United Kingdom in 2003, has found similar results. In fact, a significant number of emigrants originated from sub-Saharan Africa who are diagnosed at an advanced HIV infection stage, with less than 200 CD4/mm3 22,23. On the other hand, our results reflect an obvious delay in the management of patients in comparison with European and North American studies. A multicenter study conducted in 17 hospitals of the North and North East of France regarding about 595 newly HIV diagnosed patients, displayed that the majority of those patients (75%) were totally asymptomatic (category A), 10% belonged to the category B and about 15% had AIDS-defining conditions (category C) 24. In addition, it was suggested that the variation of virus subtypes may also contribute to some discrepancies in HIV progression between continents25. Some authors suppose that subtype E commonly seen in some Asian countries like Thailand and India seems to be a lot more virulent than subtype B which is predominant in Europe and United States of America25,26. In a series of 235 newly HIV diagnosed Thai patients with 96% of recombinant A/E form and 4% of subtype B, Ruxrungtham and al24 showed an average of CD4+T cells inferior to 200/mm3, with a 5-year survival of 82% for group A/E, versus 90% for group B26. A Moroccan study carried out between 1993 and 1996 has shown a predominance of sub-type B (93.5%) which is in accordance with the occidental pattern of HIV diversity. Nevertheless, another study conducted between 2001 and 2005 displayed a large genotypic diversity of HIV subtypes in Morocco with emergence of non B subtypes (34%) and recombinants circulating forms 27,28. In our present work, the assessment of HIV diversity consequence on the progression of HIV infection and its immunologic impact has not been studied. Such impact may be important to be explored. Conclusion The results of our study showed a delay in the diagnosis of HIV infected patients and confirm the need for intensifying prevention actions, expansion and promotion of HIV testing in healthcare facilities and within voluntary counseling and testing centres affiliated to NGOs. Further studies assessing the role of other factors (cultural, psychological, socioeconomic) may help understanding the cause of late HIV diagnosis, and should be undertaken in order to improve the management of HIV infection in our country. Acknowledgments We thank Mr Abdelmoula Laâdimi and Mrs Hafida El Bellal for help in biologic analysis. References
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10062f1.jpg] [hs10062t1.jpg] [hs10062t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}