 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
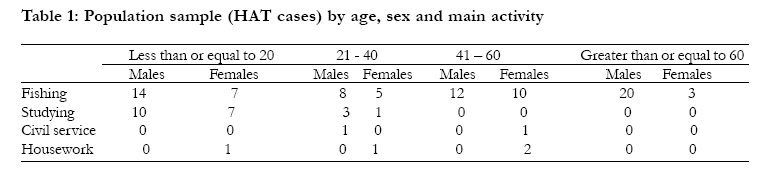
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 349-352 Microbial aetiology and sensitivity of asymptomatic bacteriuria among ante-natal mothers in Mulago hospital, Uganda *Andabati G, Byamugisha J Department of Obstetrics and Gynaecology, College of Health Sciences, Makerere University *Corresponding author: Andabati Gozanga, Department of Obstetrics and Gynaecology, College of Health Sciences, Makerere University, P. O. Box 7072 Kampala, Uganda Telephone number: +256 772 580037 Email: dandabati@yahoo.com Code Number: hs10064 Abstract Background: Asymptomatic bacteriuria in pregnancy is
associated with potential urinary and obstetric complications. However the
prevalence aetiology and antimicrobial sensitivity patterns of asymptomatic
bacteriurea among women attending ante-natal care in our Hospital is not known.
Key words: Bacteriurea, Culture, Resistance. Introduction Asymptomatic bacteriuria refers to the presence of live bacteria in the urine of an individual without symptoms of UTI1. Significant bacteriuria usually determined by urine culture, on the other hand refers to a finding of 100000 pure colonies from one ml of uncentrifuged urine sample cultured10. Asymptomatic colonization of the urinary tract in pregnant women may result in severe medical and obstetric complications1,2,3. If these potential complications are to be avoided asymptomatic bacteriuria must be detected and appropriately treated. Further more with the rampant antibiotic misuse newer and more resistant bacterial strains are likely to emerge as major aetiological agents of bacteriurea thus further complicating the management4. Although the prevalence of asymptomatic bacteriuria is known to vary between populations, generally pregnant women are the most at risk6. However there is lack of information about the prevalence and aetiology of asymptomatic bacteriuria among women attending ante-natal care in our Hospital. We therefore conducted a cross-sectional study to identify the common causes of asymptomatic bacteriuria in ante-natal mothers in Mulago Hospital in Uganda. This information we hope will aid clinicians and health care planners in the management of this potentially disastrous condition in pregnant women. Methods Pregnant women not having any symptoms attributable to UTI (dysurea, frequency, fever) were consecutively invited to participate in this study from May 2009 to Dec 2009. Women who reported recent par vagina bleeding were excluded. Those who had used antibiotics in the preceding two weeks for indications other than urinary tract infection were not excluded but noted (table 1). We obtained informed consent from each participant. After recording information about the socio-demographic and obstetric characteristics of the participant she was then requested to provide clean catch mid stream urine sample for semi-quantitative culture. To obtain the urine sample the participant would first clean the vulva thrice from in front backwards each time with a separate piece of sterile gauze soaked in saline. Then using a wide mouth sterile bottle of 50mls she would collect urine sample starting approximately two seconds from the beginning of the flow. A portion of the urine sample was also examined under microscope and tested with Acon® urine strips. The results of the later have been published else where11. Bacterial growth was considered significant if 100000 of pure colony forming units of single bacteria were obtained from a mililitre of un-centrifuged urine10. Initial culture was done on nutrient agar and sub-culture in differential mKonkey agar. The bacterial isolates were identified using the Epi 120 system Kit. We performed anti-bacterial sensitivity tests of the isolates to the commonly used antibiotics (Amoxycillin, Augmentin, erythromycin, Nitrofurantoin, gentamicin, ampicillin, ceftriaxone, cefuroxime) Results Up to 219 pregnant women participated in this study. One urine sample went missing leaving 218 for testing. Twenty nine of the 218 urine samples (13.1%) had significant bacterial growth. None of the selected socio-demographic characteristics was significantly associated with asymptomatic bacteriurea (Table1). Bacterial isolates and their antimicrobial sensitivities Eschericia coli was the commonest bacterial isolate accounting for 51.2% of all positive cultures followed by Staphylococcus epidermidis(20.2%), Klebsiela (18%) Staph. aureus(6.2%), pseudomonas(6.0%) and enterococcus(0.8%) Most bacterial isolates (62%) were resistant to amoxicillin but sensitive to ceftriaxone and augmentin The sensitivity of E. coli the most prevalent isolate was highest (100%) to ceftriaxone followed by augmentin, ampicillin and erythromycin (Fig 1). Previous use of an antibiotic in the preceding two weeks for any indication other than treatment of UTI was not significantly associated with anti-microbial resistance (OR=1.3 CI 0.54- 3.40). Antimicrobial use in the previous two weeks We investigated the use of oral or injectable antibiotics in the previous two weeks among the participants for indications other than UTI. Eleven (5%) of the participants had used antibiotics. The commonest reason was to treat cough (6/11). Three participants used antibiotics for unknown reasons, one to treat skin infection and another to treat diarrhea. The majority used cotrimoxazole except one who had used metronidazole tablets for treating diarrhea. Previous antibiotic use was not significantly associated with resistance (p =0.435) Discussion We found a 13.3% prevalence of asymptomatic bacteruria in the ante-natal mothers in Mulago Hospital. Anayet et al5 found a similar prevalence among Bangaladesh women. However Obibgolu et al reported a four fold higher prevalence among pregnant women in rural Nigeria6. In most populations the prevalence of UTI (both symptomatic and asymptomatic) is relatively higher in pregnant women compared to the non-pregnant counter parts. This could be attributed to the anatomical and physiological changes that occur in the urinary system of pregnant women. During pregnancy the rising levels of progesterone and mechanical obstruction of the distal ureters by the gravid uterus causes urinary stasis thus promoting bacterial colonization7. Our study only investigated pregnant women. Like in other studies else where, E.coli was the commonest cause of asymptomatic bacteriurea in our ante-natal mothers. This could be due to its inherent virulence for urinary colonization particularly the adhesive abilities of E.coli. It could also be explained by the fact that lower gastro-intestinal tract (GIT) where E.coli is a normal flora is the main source of infective agent for asymptomatic bacteriurea in ante-natal mothers and hence the commonest cause of urinary tract colonization5,6,8,9,10. We found higher overall level of resistance of the isolates to the commonly used antibiotics. Anti-biotic resistance was not significantly related to history of recent antibiotic use. This might be so because the mechanisms of anti-biotic resistance involve bacterial mutations in response to repeated exposure to the antibiotic in question. These mutations take time and are therefore unlikely to occur within two weeks of exposure as in the study period. Recommendation All ante-natal mothers in our unit should be screened and treated for asymptomatic bacteriuria. There is need to revise and establish antibiotic policy so as to guide against the emergence of resistant organisms that cause asymptomatic bacteriurea in ante-natal mothers. Implications of the study This study is the first of its kind to demonstrate that asymptomatic bacteriurea is prevalent among ante-natal mothers in Mulago Hospital, thus uncovering this potentially hazardous and yet least recognized infection among our ante-natal mothers. The study has also demonstrated, although on few positive samples the high resistance of the bacterial isolates to amoxicillin,gentamicin and ampicillin (the antibiotics commonly used for the treatment of urine tract infections in our unit) thus calling for action to cab this resistance. Limitations of this study The number of participants was so small that the possible factors associated with resistance could not be satisfactorily assessed with statistical methods. Conclusion Asymptomatic bacteriurea is common in ante-natal mothers in Mulago Hospital and E.coli is the commonest organism involved. The majority of the bacterial agents that cause asymptomatic bacteriurea in the ante-natal mothers are resistant to the commonly used anti-biotics. Acknowledgements This work received full financial support from Sida SAREC through the competitive grants round-6 to academic staff of Faculty of Medicine, MakerereUniversity. We also wish to express our sincere gratitude to all those who participated in sample collection and analysis. Reference
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10065t1.jpg] [hs10065f1.jpg] |
| |||||||||

{kind=link}
{kind=link}