 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 362-366 Skin diseases among children attending the out patient clinic of the University of Nigeria teaching hospital, Enug *Emodi IJ, Ikefuna AN, Uchendu U, U Duru A University of Nigeria Teaching Hospital, Enugu, Nigeria *Correspondence author: Emodi Ifeoma, Consultant/Senior Lecturer, University of Nigeria Teaching Hospital, Enugu, Nigeria, Email: ifeoma_emodi@yahoo.com Code Number: hs10067 Abstract Background: The prevalence of skin diseases varies
worldwide and information regarding local prevalence of its various causes
may help the development of policies towards better management.
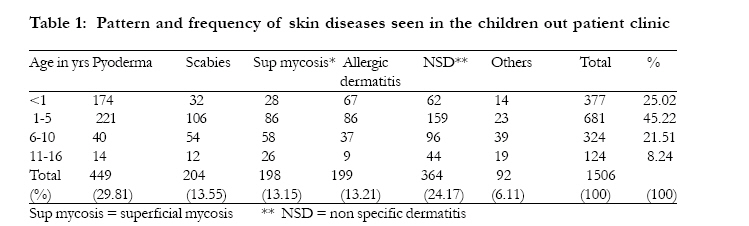
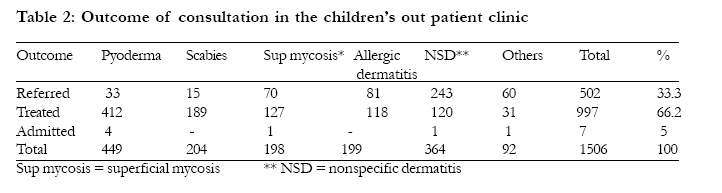
Key words: profile, childhood, skin diseases, Enugu (Nigeria) Introduction The incidence of paediatric dermatological problems varies from one part of the world to another.1 Skin diseases, though very common in many developing countries, are not often regarded as a significant health problem2-5 even when serious diseases may be heralded by skin changes.2 Studies carried out among children have indicated that the infective disorders mainly pyoderma and scabies are major causes for visit to primary health care facility in developing countries.1,4,6 Prevalence studies from the community, 5,7,8 dermatology clinics 9-11 general out patient clinics6 and primary health centers 4 have indicated some differences in the types of diseases found in the different settings. Community studies have shown the high burden of dermatophytosis among school children in both urban 7,8 and rural5 areas in Nigeria while dermatology clinics have reported higher incidence of atopic disorders.9 -11 It has been shown in other parts of the world that there is generally poor health seeking behaviour in individuals with skin disease.12,13 This behaviour might depend on how severe the ailment is perceived to be and the availability of assistance. Patients withscabies and pyoderma are more likely to seek medical attention probably due to the more severe symptoms experiences with these conditions.1,14 as these disorders may cause severe discomfort. The ready accessibility of drugs across the counter in this country also lends to self medication and decreases the attendance of the patient to a health care facility. The ability of the attending doctor to manage the ailment depends on the skills and knowledge acquired during the undergraduate training and/or his/her exposure to specialist training. The WHO (World Health Organization) in a workshop in 2004 has advocated for strengthening of community dermatology for developing countries 2 while others have called for training of health workers in the diagnosis and management of skin diseases.15 These efforts may help address the problem of misdiagnosis and management of these disorders. Presently the Faculty of Paediatrics in the National Post Graduate Medical College has not enforced the elective postings in other departments eg dermatology as part of the requirements for fellowship. This paper was undertaken to explore the pattern of skin diseases seen at a general urban paediatric out patient clinic and the ability of the consulting doctor to manage such problems. Furthermore, this is expected to provide evidence to support the development of a dermatology education programme for general paediatric doctors in training in order to improve their skills and reduce diagnostic uncertainty. When this occurs the patient will benefit from the services of the health care facility. Methods The University of Nigeria Teaching Hospital is a tertiary institute serving Enugu state, Nigeria and its environs. It also serves as a primary health facility as patients can and do walk in for consultation and treatment. The department of paediatrics in the hospital provides care for children through consultant out patients, special referral clinics and the Children Out Patient (CHOP) clinic. The latter clinic is manned by resident doctors who are in training with a consultant paediatrician available for immediate consultation when the need arises. The dermatology clinic within the hospital complex accepts only referred cases from within and outside the hospital The register of patients attending the CHOP department of UNTH Enugu was used to extract data on children who presented with skin problems between January 1996 and December 2005. The clinical note of every child that is seen in the clinic is used by the nursing staff to record the biodata of the child, the diagnosis made and the outcome of the consultation. The data extracted from the register included the age, sex, diagnosis and outcome of consultation which could be whether the child was admitted, treated by the physician or referred to the dermatology clinic for expert management. Ethical clearance was obtained from the ethical review board of the hospital For the purposes of this paper the disorders were broadly classified into pyoderma, superficial mycoses, allergic dermatitis, benign viral tumors, non specific dermatitis and others.1 The term pyoderma was used for those diagnoses termed impetigo, skin infection, carbuncle, pemphigus, furunculosis, pustular skin eruptions, septic skin lesions, and cellulitis. Superficial mycoses was used to designate diagnosis that included tineasis, tinea corporis, tinea capitis, pityriasis versicolor, skin mycosis and fungal infection. Diagnoses that were termed allergic dermatitis included infantile eczema, allergic dermatitis, urticaria, contact dermatitis, irritant dermatitis papular urticaria and atopy. The patients whose recorded diagnosis were rashes, dermatitis, dermatosis, body rash, and skin disease were grouped as non specific dermatitis in this study. Onchorcerciasis, vitiligo, albinism, mulluscum contagiosum, warts, fixed drug eruption, keloids, and milia were grouped as others. Unfortunately referred patients were not followed to the skin clinic to ascertain the final diagnosis when they were reviewed at the dermatology department. In addition we did not include subjects that were referred directly to the dermatology department. Data collection and analysis were performed using the software SPSS (Statistical Package for Social Sciences, Chicago, I1, USA) Version 11.0. frequency tables were used to describe the categorical variables. Results During the period under review, one hundred and sixteen thousand, three hundred and thirty seven (116,337) children were attended to in CHOP. Of this number one thousand five hundred and six (1.3%) had a skin lesion as their primary complaint. There were eight hundred and thirteen (54%) males with a male: female ratio of 1: 0.85. The age range was one week to sixteen years with a mean age of 3.89years (SD 3.8). One thousand and fifty eight (70.24%) of the children were 0 - 5 yrs old, and three hundredand twenty four (21.5%) were 6 10 yrs. (Table 1). The diagnosis of pyoderma was made in 449 (29.81%), non specific dermatitis 364 (24.17%), scabies 204 (13.55%), allergic dermatitis 199 (13.21%), superficial mycoses 198 (13.15%), and others 92 (6.11%). The other diagnosis were vitiligo (n=20), pityriasis rosea (n=11), oncocerciasis (n=9) hyperkeratosis (n=8), puritis (n=6) naevi (n=5) and drug reaction (n=3). There were 4 diagnoses each of warts, alopecia, and hypersensitivity reaction while keloids, Molluscum contagiosum and lichen planus were 2 each. There was 1 diagnosis each of heat rash and cutaneous larva migrans. The highest cutaneous disease burden was seen in those children aged 1 - 5 yrs followed by those less than one year old. Superficial mycosis was least common among those less than 1 year of age and those aged 11 - 16years. Majority (24.17%) of the patients with a diagnosis of non specific dermatitis majority were between 1 and 10 yrs. With regards to scabies it was most common in those aged 1 5yrs (n=106) then 6 10yrs (n=54). It was present in several members of the same family and some of the lesions had superimposed infections. Viral warts were found in only those aged more than 15 yrs. When the incidence of disease was observed from January to December it was noted that there was a clustering of pyoderma during the warm wet season of April to September. The other diseases did not depict an obvious seasonal variation. The doctors in CHOP were able to treat 66.2% of patients, 33.3% was sent to the specialist dermatology clinic in the hospital while 0.5% was admitted. The latter were mainly neonates with severe pyoderma (n=4) while the other patients that were admitted were for other non dermatological diagnosis namely bronchopneumonia (n=2) and gastroenteritis (n=1). Among the 502 patients referred to the dermatology department 243(48.4%) had non specific dermatitis." Instead of 4%) had non specific dermatitis. The least referrals were for those patients with scabies and pyoderma. Discussion The health seeking behaviour for skin diseases in this environment is low but is comparable with some industrialized countries 13 where 90 out of 129 students with symptomatic skin disease did not seek medical assistance. In the Netherlands about 1% of consultations to the General practitioners were for skin diseases14 which is comparable to our own figure of 1.3%. In contrast to our own experience, workers in Mali have shown that 11.7% of consultations to 8 health centers studied were for a skin disease and this might also be the case in our environment.16 This behavior might also be an indication that the burden of other diseases like malaria and respiratory tract infection over shadows that of the skin which might not be viewed as being life threatening. The ability of the parent to purchase any drug over the counter would also contribute to the self medication that occurs resulting in late presentation by patients. It is possible that patients might also have been referred directly to the dermatology clinic without being seen in our children's clinic. Infective conditions were the most frequent condition for seeking health care which is similar to the finding in the General out Patient of the University College Hospital (UCH) Ibadan and other health facilities 5, 4 but is different from that seen in specialist dermatology clinics.9-11 These differences might be because these latter studies did not only review children and the influence of the diseases found in the older members of the population might have influenced the proportions. These centers also serve areas where there are many health facilities unlike in Sokoto north-western Nigeria 16 where it was documented that the infective causes dominated the visits to this specialist centre. The ability of other non specialist doctors to identify and treat pyoderma and scabies might also contribute to the non referral of such cases. The diagnosis of pyoderma made in 29.8 % of our patients is less than that of impetigo (33.4%) and boils (7.0%) from Ibadan 5 south-western Nigeria. There was no obvious peak age for scabies but an increase in incidence was seen between those aged 1 5 years. The prevalence of 13.5% in this study is higher than of 2.2% 11 reported from the same hospital in 2005. This difference could be due to the fact that the patients had secondary lesions which were not identified by the non specialist and hence the referral. The value of 13.5% was also higher than the figures from Ibadan6 which could be a reflection of the falling health and personal hygienic practices in the community and environment The diagnosis of superficial mycoses(SM) was made in 13.15% of our patients was more than the 10.4% in the Ibadan6 series from GOP. The majority of these patients were aged 1 5 yrs and this also differs from other reports that SM is more common in those aged 13 years and above.1 The figures in this study were relatively low considering the data from community studies6 and school children.3,7,8 This could be a reflection of the poor health seeking behaviour of persons for this disorder seen even in developing countries or reflect the fact that many Africans consider scalp ringworm as normal and would not seek treatment in a health facility.12, Allergic dermatitis seen in 13.2% of the children was more common in those less than 5 years which is in keeping with the study from Ibadan.6 A majority of the children with allergy had infantile eczema which is usually seen at a lower age bracket. Non specific dermatitis was the diagnosis made in 24.2% of patients and might reflect the inability of the doctor seeing the patient to make a definite diagnosis as this classification was used for those patients where the attending doctor made a diagnosis of dermatosis, skin disease, or unclassified dermatitis etc. This diagnosis was also made in 37.9% of the patients aged 11years and above. The increased prevalence of pyoderma seen in April to September which is the rainy season in Nigeria has been documented by other studies 1 and is thought to be due to the increased humidity in these months. We did not find an obvious increase in allergic dermatitis in the dry months of October to March. This being a retrospective study the attending physician may not have adhered to the standardized guidelines for skin diseases thus creating the possibility of a variation in diagnosis. The problem associated with incomplete data entry commonly found in retrospective studies is appreciated. It is noteworthy that 48.4% of patients referred to the skin clinic had a diagnosis of NSD. This highlights the potential need for additional dermatology training for paediatric residents to improve their diagnostic confidence and management skills of common childhood dermatosis. In addition, the call made by WHO 1 and others 14 for training of health workers in the diagnosis and management of skin diseases is quite apt and should be adopted by all nations. Conclusion From this study it is clear that the burden of skin disease seen among children less than 16 years is still infective in origin with bacterial causes being highest. The high level of diagnosis of NSD suggests a limited understanding of dermatology and further training such as a rotation through dermatology may improve diagnostic accuracy and lead to more appropriate cost effective first line management References
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10067t1.jpg] [hs10067t2.jpg] |
| |||||||||

{kind=link}
{kind=link}