 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 367-373 Prevalence of overweight and obesity in young adults in Uganda *Baalwa J1,2, Byarugaba BB2, Kabagambe KE,3 Otim AM1 1 Department of Internal Medicine, Makerere University Medical
School, Kampala, Uganda *Correspondence author: Dr. Joshua Baalwa, Department of Internal Medicine, College of Health Sciences, Makerere University, P.O Box 7072, Kampala, Uganda, Email:joe05@uab.edu Code Number: hs10068 Abstract Background: Obesity in young adults is rising and predicts
diabetes and cardiovascular diseases later in life. Data on prevalence and
determinants of obesity in developing countries are needed for primary prevention.
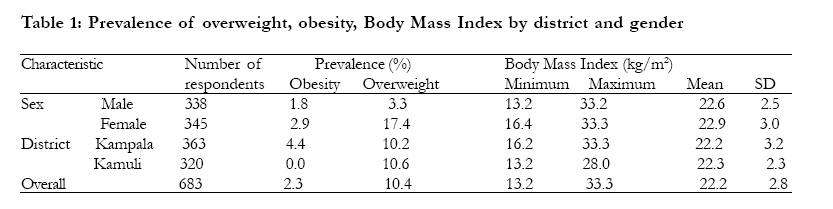
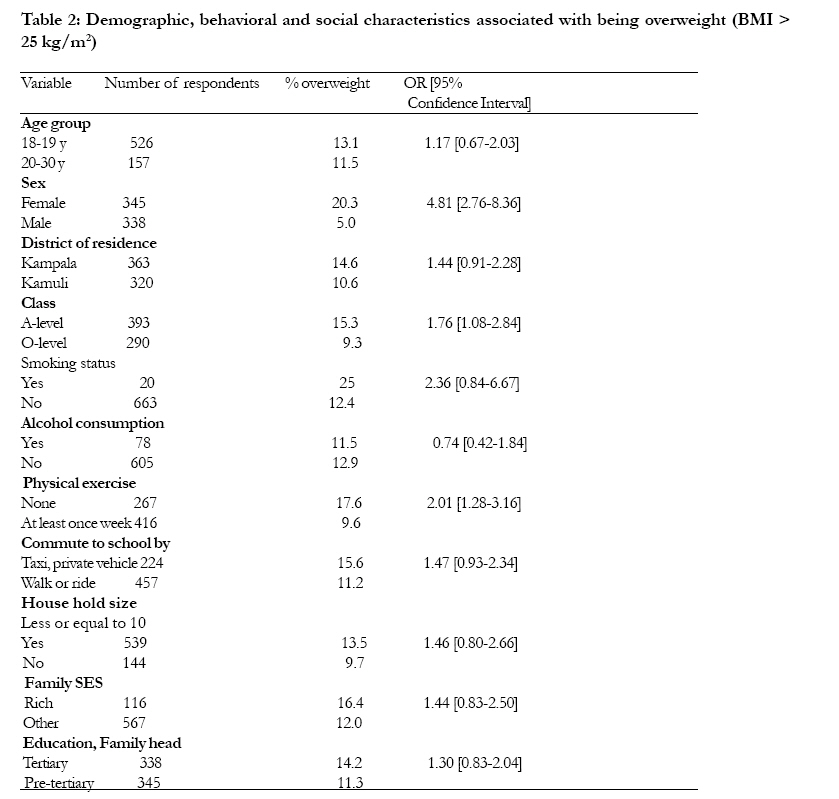
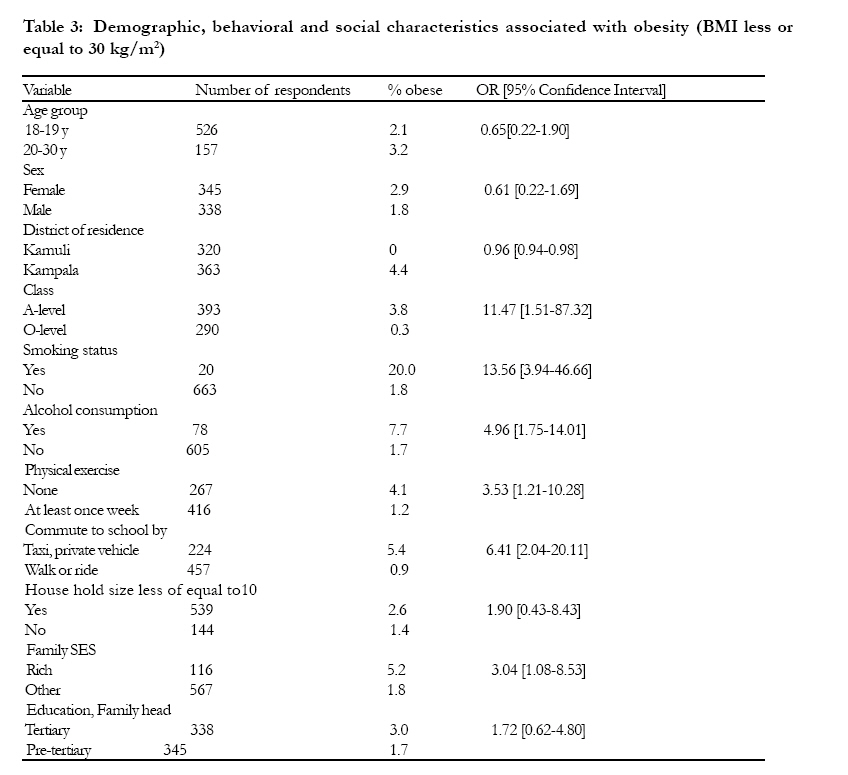
Keywords: Obesity; overweight; prevalence; Uganda; young adults Introduction The World Health Organization estimated that by 2005, at least 1.6 billion and 400 million people aged above 15 years were overweight and obese respectively. It further projected that by 2015, these statistics will increase to 2.3 billion for overweight and 700 million for obesity, unless drastic measures are taken to mitigate this burgeoning problem1. In Africa, despite a high prevalence of under nutrition, the prevalence of overweight is increasing at an alarming rate. It is estimated that 25% to 60% of urban women are overweight2. The prevalence of overweight and obesity is also rapidly increasing among children. The International Obesity Task Force estimates that about 155 million school-going children globally, are either overweight or obese3. Obesity and overweight in childhood and young adulthood is not a benign problem. It is often associated with the presence of the metabolic syndrome and asymptomatic cardiovascular disease4,5. Indeed, children and young adults who are obese, are more likely to have clustering of cardiovascular disease risk factors such as; dyslipidemia, hypertension, increase in left ventricular mass, type 2 diabetes mellitus and elevated fasting and post-load insulin levels4,6-10. In addition, according to the Pathobiological Determinants of Atherosclerosis in the Young study (PDAY), obese young adults who had elevated glycosylated hemoglobin of > 8% had an increased likelihood of having atheromata in the aorta and coronary arteries11. Furthermore, childhood obesity and overweight strongly predict the risk for obesity and metabolic syndrome in later adulthood12-17. Therefore if unchecked, obesity in childhood and young adulthood represents a continued snowballing risk for the development of cardiovascular disease, especially in developing countries with poor secondary prevention. The increase in obesity calls for accelerating programs that target primary prevention in developing countries, a practice that requires local data on the magnitude of the problem and associated risk factors. Presently, there is limited data in Uganda on the magnitude of overweight and obesity and their associated risk factors among young adults, and this represents a significant gap in knowledge. In this study, we sought to determine the prevalence of overweight and obesity and their associated factors among young adults enrolled in schools in rural and urban Uganda. Methods Study design We undertook a cross-sectional descriptive study to determine the prevalence of obesity and overweight and their associated factors in school-going young adults in rural and urban areas of Uganda. This study was approved by Makerere University faculty of Medicine, ethics and research committee prior to its implementation. Study sites The study was conducted in randomly selected secondary schools in Kampala city and in Kamuli district in Uganda, the former and latter representing urban and rural settings. Kamuli district is located approximately is 80 miles north-east of Kampala city, with more than 95% of its population living a rural peasantry lifestyle and with 70-80% of the population living below the national poverty line18. For Kamuli, the selected schools were at least two kilometers away from the nearest urban center. On the other hand, Kampala city is the capital of Uganda. It is the most appropriate prototype of an urban milieu in Uganda. Study population Seven schools in Kampala city and 7 in Kamuli District were randomly selected for inclusion in the study. For both study sites, only day scholars were invited to participate in this study since they are uninstitutionalized and therefore likely to have dietary and other behavioral habits that are representative of the majority of the general population of young adults in the selected districts. Day scholars 18 to 30 years old who gave informed consent for inclusion into this study were recruited. We did not encounter a shortage of participants equal or older than 18 years of age to enroll into the study for any given school. This could mainly be explained by the fact that approximately 75% of children in Uganda commence primary school later than the expected age of 6 years and that the average age of a child attending primary seven is 14.7 years19. Individuals were excluded from this study if they had a chronic illness, were pregnant, physically disabled or taking contraception or neuroleptics. Participant enrollment A three stage sampling procedure was used to select participants for the study. For stage one, names of all secondary schools from the two study sites, were obtained from the school inspectorate division of the ministry of education headquarters and this comprised the sampling frame. All the schools in the sampling frame were considered as clusters and were subjected to simple random sampling. Briefly, each school in the sampling frame was given a code number which was written on a small piece of paper and placed in a basket. From the basket, clusters were randomly selected one at a time until seven Kampala city and seven Kamuli district schools were obtained. Participants from each of the 14 schools were then stratified according to their classes and from all strata, a final list of eligible participants per school was obtained. Finally, for stage 3, at least 46 participants fulfilling the eligibility criteria were randomly selected from each school. Data collection and Procedures Data collection was executed by means of a questionnaire, which was designed with the guidance of a biostatistician, clinical epidemiologists and endocrinologists. The questionnaire tool was initially validated prior to formal implementation of the study. Research assistants who assisted with data collection and anthropometric measurements received rigorous training and assessments prior to commencement of the study. During data collection, the assistants received continued technical support and supervision from the principal investigator. Participant weights were taken using standard hospital-adult lever weighing apparatuses which had been recalibrated and certified by a biomedical engineering technician prior to use in the study. A vertical rule with a sliding arm attached to the weighing apparatus was used to take height measurement. Students stood erect, upright and barefooted or in stockings and had extra clothes such as coats and sweaters removed while weight and height measurements were being taken. Weight and height measurements for each participant were used to calculate the Body Mass Index (BMI) as previously described1. Data collection lasted a period of three months from February to April 2004. Key Informant interviews The purpose of key informant interviews was to obtain additional information on the factors associated with overweight, given the surprising finding of similar prevalence rates for overweight among young adults in rural and urban settings. Additional qualitative data was collected by face to face interviews of key informants who constituted parents and teachers from the study schools during the data dissemination exercise. Fair gender representation at the interviews was always realized. Parents and teachers were selected as key informants because they were presumed to have first hand knowledge about their local community social and health practices. Four face to face interviews from four schools, two from each study site were held to obtain deeper insights on local community dietary practices and temporal trends in obesity and dietary habits. An interview tool encompassing questions related to these two themes was used by the principal investigator and two assistants to collect qualitative data, which mainly comprised taking notes. Questions specifically asked included; trends in sedentary habits, major dietary constituents, size of food portions and changes in local staple foodstuffs over time. Data obtained was categorized under these questions and for each question an impression and conclusion of what the data meant was arrived at after iteratively examining and discussing the interview notes among the study authors. Measurements The primary study outcomes were: obesity, defined as a participant having a body mass index of e" 30 kg/m2 and overweight, defined as a BMI e" 25kg/m2 but <30 kg/m2. Level of physical activity was determined by asking participants how many times in a week they engaged in exercise and sports lasting at least 30 minutes per day and by asking by what means they commuted daily to school. Weight and height were measured using an adult hospital lever balance with participants wearing light clothing and no shoes or extra articles. Participants' social economic status (SES) was determined using a modified Home Affluence Scale as previously described(20). Briefly, car ownership and housing tenure were maintained in the modified SES assessment tool because from past studies other parameters such as parental education, occupation and fiscal income tend to be incorrectly answered by youths. Other independent variables determined included participants' socio-demographic characteristics like age and gender, and whether participants routinely smoked cigarettes or consumed alcohol at least once per week. Statistical analysis Sample size was determined using the Kish Leslie formula and considering the prevalence of overweight of adult Uganda women as reported in the Uganda Demographic and Health survey of 200121. Data was entered into SPSS. Unpaired t-test for independent samples was used to compare means of continuous variables while the chi-square test was used for categorical variables. Differences were considered significant if the p-value was less than 0.05. Results Overall 683 participants were enrolled into the study. The mean (SD) age was 19.0 (1.4) years and females represented 50.5% of the study population. The prevalence of obesity and overweight by gender and district of residence is shown in table 1. The mean BMI was 22.2 kg/m2 and ranged from 13.2 to 33.3 kg/m2. Tables 2 and 3 show the distribution of overweight and obesity by demographic, behavioral and social characteristics. Kampala was not significantly different from Kamuli District with regard to the prevalence of overweight (p=0.12). Females were 4.81 times (95% CI: 2.76-8.36) more likely to be overweight than males. Important findings from interviewing key informants were that rural youths were still less sedentary compared to their urban counterparts as they were required to walk or ride longer distances to school and engage in household activities such as farming and fetching water a distance away from home. It however, clearly emerged from the interviews from rural informants that the majority of individuals in their communities routinely consumed large food portions of mainly carbohydrate diets. In contrast, we found from urban informants that urbanization had ushered in a nutrition transition and was promoting sedentary lifestyles. Discussion Our data show that more than 10% of young adults in urban or rural areas are overweight and that compared to males, females are more likely to be obese and overweight. Contrary to our expectation, we did not observe significant rural-urban differences in the prevalence of overweight, which we found to be 10.6% and 10.2% respectively. This finding was against the typically held norm in Uganda that rural inhabitants are more likely to be of normal weight or even malnourished because they tend to be less sedentary, walk long distances to school and indulge less often on fast and highly processed foods compared to their urban counterparts. In order to decipher the cause of this paradox, we interviewed key informants who included teachers and parents from the two study settings during dissemination of our study findings. From their views, we established that true to the norm, rural inhabitants were less sedentary but routinely consumed large portions of high carbohydrate diets whereas their urban counterparts were more sedentary and had more access to fast and highly processed foodstuffs that are often high in energy. These findings, highlight potential differences in the aetiological associations of overweight in rural and urban settings, and call for a differential approach to preventing the problem. Furthermore, we found that female students were 5 times more likely to be overweight and obese compared to their male counterparts. This has been reported in several previous studies and is known to be related to gender differences in metabolism and hormonal balance22,23. Additionally from our key informants, we established that female students were increasingly susceptible to excess weight gain because they were less likely to engage in regular exercises or sporting activities partly due to lack of facilities that are gender sensitive but also to some degree due to the fact that they are culturally constrained to taking care of domestic chores after school hours, which leaves them with less time for roles that include vigorous physical exercise. Female students were also unlikely to go to schools that required them to walk a long distance away from home. Other important findings of this study include the statistically significant relationships between obesity, smoking and alcohol consumption. These were found to be problems mainly among urban students. This is contrary to findings from some studies showing that smoking and alcohol consumption are inversely associated with weight gain24. We found that students who smoked were more likely to be obese and less likely to engage in regular physical activity including sports. Again this highlights smoking as another public health problem that should be addressed in obesity prevention programs especially in urban settings where smoking is more prevalent among young adult school-going individuals. The main strength of this study is that it is the first of its kind to examine the prevalence of overweight and obesity in rural versus urban inhabitants and their associated factors, among a large population of school-going young adults aged between 18 and 30 years in Uganda. This age group which has been termed the transition period by socio-epidemiologists is a critical one because it is when individuals become of legal age, join higher institutions of learning, complete their education, become employed, get married or join parenthood. As a result, this period is associated with significant lifestyle changes some of which are beneficial and others deleterious to health, and therefore represents an important timing for laying strong primary prevention interventions for public health problems such as overweight and obesity. However, our study also had limitations. Our findings are purely descriptive and lack tertiary statistical analysis to explore the possibility of confounding among statistically significant relationships. Another study limitation is that alcohol and cigarette smoking were not quantified and therefore their association with primary study outcomes could have resulted purely by chance. Acknowledgements This study was supported with funding from the Hamilton Mountain Seventh Day Adventist church in Hamilton, Ontario, Canada. We thank Dr. Harriet Mayanja and faculty from the Department of Medicine, Makerere University for their critical review of this study; and Annette Namunhana, Joseph Bifamengo and Simon Terwane for assistance with data collection. We thank Drs. Ziraba Abdullah Kasiira and Charles Wamboga for assistance with statistical analysis. We thank all the study participants and the school administrations involved in this study. References
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10068t2.jpg] [hs10068t3.jpg] [hs10068t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}