 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 374-385 Gender-based profiling of Quality of Life (QOL) of primary health care (PHC) attendees in central Uganda: a cross sectional analysis *Muhwezi WW, Okello ES, Turiho AK Department of Psychiatry, School of Medicine, Makerere University College of Health Sciences, Kampala, Uganda *Corresponding author: Dr. Wilson Wintsons Muhwezi, Department of Psychiatry, School of Medicine, Makerere University College of Health Sciences, P.O. Box 7072, Kampala, Uganda, Email address: wmuhwezi@chs.mak.ac.ug Code Number: hs10069 Abstract Objective: To analyze gender differences in QOL of
patients presenting at PHC centres and to identify the socio-demographic variables
associated with poor QOL.
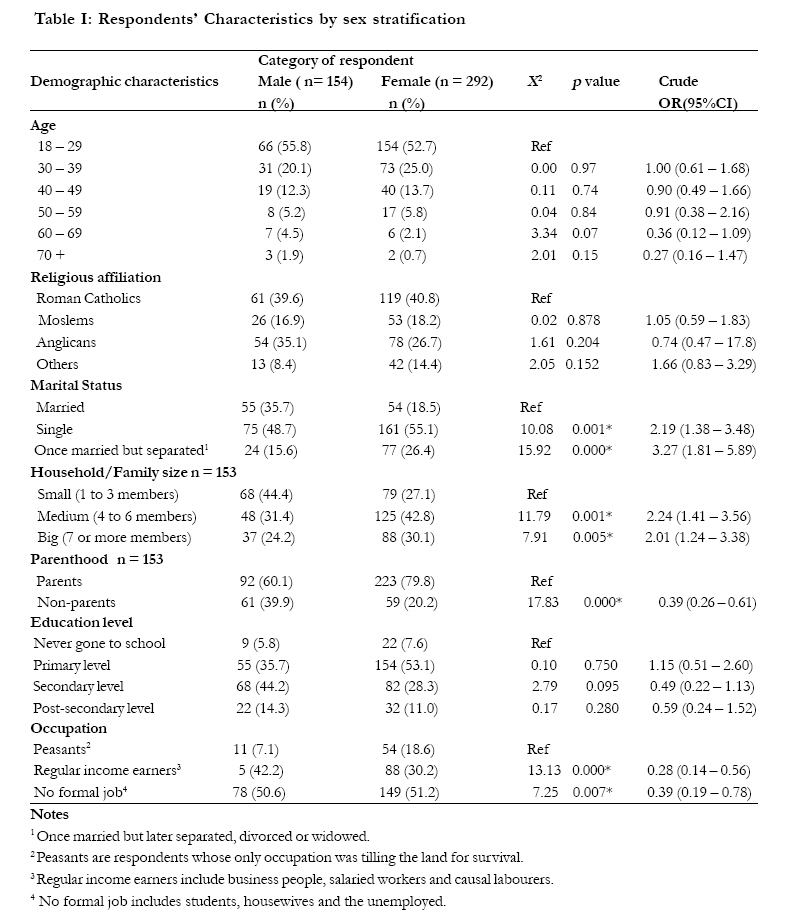
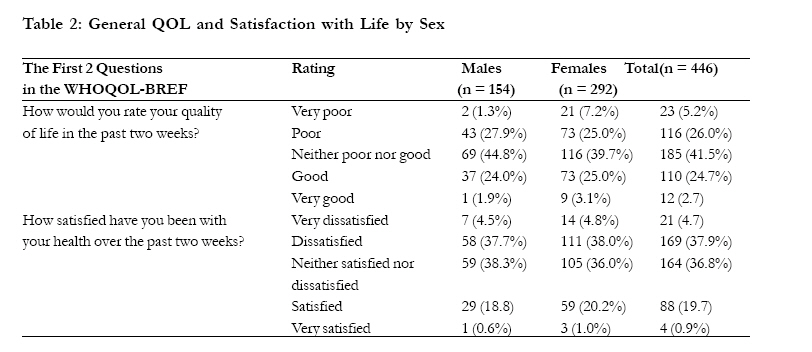
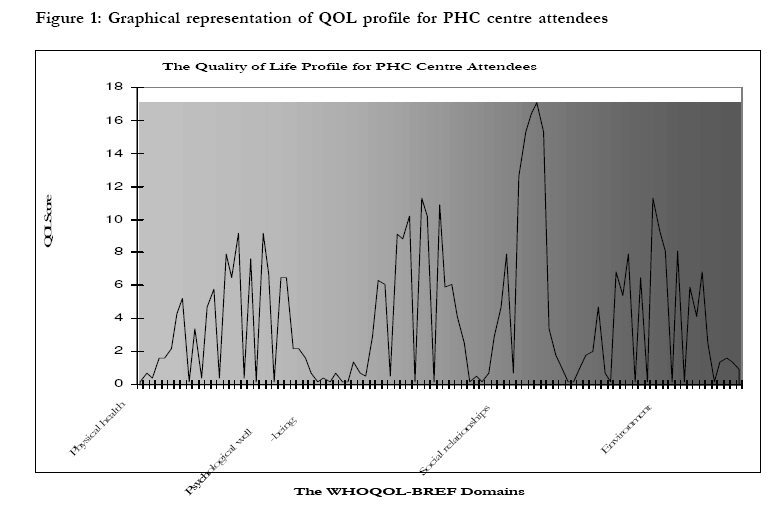
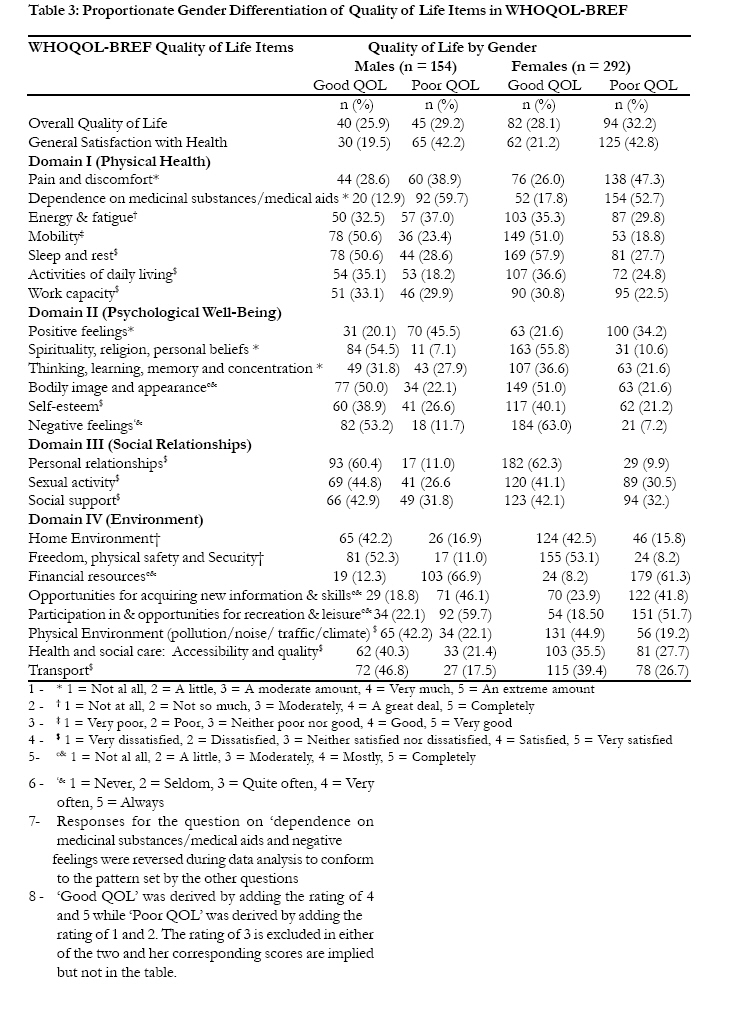
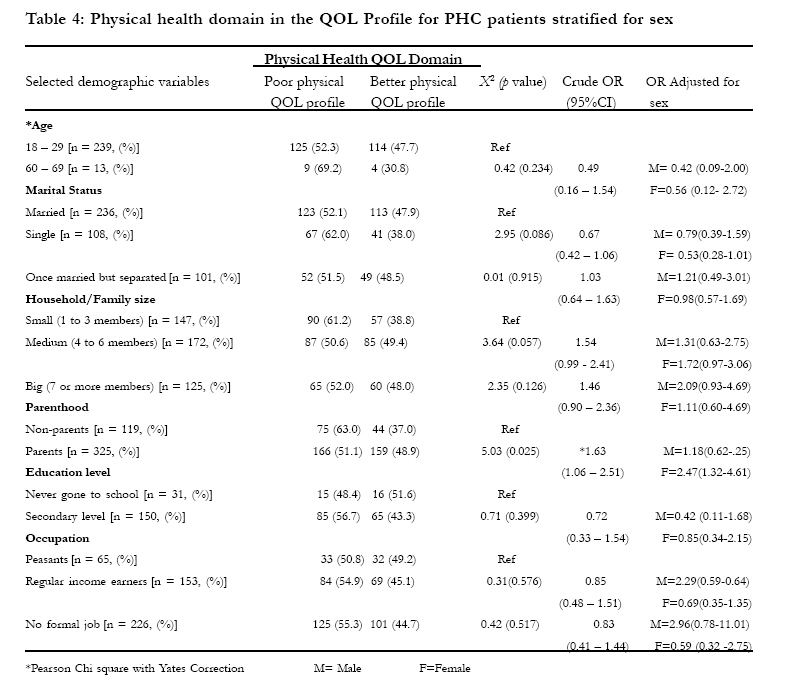
Key words: quality of life, primary health care, Uganda, gender Introduction Quality of life (QOL) research is rare in most of Sub-Saharan Africa. In the developed Western societies, features of the mental state such as symptoms of poor mental health and symptom severity have been used to make inferences about patients' subjective well-being and QOL1, 2. Consideration of QOL issues is important because it allows for a more comprehensive view of the patient's life. The definitions of QOL vary a lot but the World Health Organization (WHO) defines it as individuals' perceptions of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns3, 4. This definition reflects the view that QOL refers to a subjective evaluation which is embedded in a cultural, social and environmental context. Since this definition focuses upon respondents' "perceived" quality of life, it is not expected to provide a means of QOL measurement. Previous research that compared men and women demonstrates QOL differences based on gender-associated disadvantages such as lower socioeconomic status of women and higher rates of widowhood5. The importance of gender in QOL analysis remains a subject of controversy. Studies from Finland, Japan and Israel focusing on gender differences in QOL have reported consistently worse results for women6-11. Paradoxically, women in nearly the whole world show a distinct advantage in survival12, 13. The determinants of these gender differences in QOL are still unclear, more so with regard to the extent to which these differences can be attributed to social or biological factors10. In individual patient treatment, QOL provides a framework by which patients, carers and clinicians may assess the impact of illness and treatment on varying domains, allowing monitoring of progress and comparison between alternative treatments. QOL measures may also allow the burden of illness to be measured and compared across domains in epidemiological research and health economics. In this way, the impact of illness could be studied across cultures, gender, and age groups14. It is generally accepted that ill-health has a significant impact on QOL. In the Medical Outcomes Study15, ill patients rated their QOL as being worse than for those who regarded themselves as healthy. Although it might be reasonable to hypothesize that severity of ill-health is likely to be predictive of poor subjective QOL, the contribution of gender and other socio-demographic factors in such a relationship has been noted but more remains to be explained16-18. Secondly, the sex variable appears to have a modest contribution to the differences in perceptions of QOL19. Other researchers emphasize that the impact of gender in the QOL construct of alcohol dependent patients is not fully known, and that it is probably a variable worthy of further investigation20. Gender differences appear to contribute little in terms of QOL21, 22. For instance, using alcohol abuse as indicator of poor QOL, gender difference did not significantly impact upon any of the 12-week outcome measures in a study of inpatients at a voluntary sector alcohol detoxification unit in South London. In the same way, there was no significant difference in relapse rates or time taken to relapse between men and women. The only significant total sample change was a reduction in the amount of alcohol consumed in a typical week 19. The same study goes on to observe that women score poorly on QOL measures yet they are more socially advantaged than the men, albeit not to a statistically significant level, which seems difficult to reconcile. Therefore, more research to explain the findings is proposed19. Ultimately, the relative paucity of research from Sub-Saharan Africa involving gender-based profiling of QOL in patients at primary health care (PHC) centres is a reality. Hence, this paper seeks to present a gender-based profiling of the QOL of PHC attendees in Central Uganda. The aim of the study was to analyze gender differences in QOL of patients presenting at PHC centres and to identify the socio-demographic variables associated with poor QOL in Central Uganda. Methods The study setting The study was conducted in three PHC centres in three different districts of central Uganda. These were; (i) Naguru Health Centre, then located in one of the eastern suburbs of Kampala, the capital city of Uganda, (ii) Mukono Health Centre, a rural-based facility in Mukono District, to the east of Kampala and (iii) Mpigi Health Centre, located in semi-urban/semi-rural setting of Mpigi Town in Mpigi District, to the south-west of Kampala. People seeking services at Naguru Health Centre could be better described as urbanites, speaking a number of languages, with Luganda and English being the most common. Those found at health facilities in Mpigi and Mukono districts could be described as rural and their main language was Luganda. The study was conducted in the selected government-funded PHC centers providing free healthcare services. These services were predominantly accessed by those with no or low incomes in the community. Whereas this study could have been done in any other setting or at a bigger scale, a decision to focus on three PHC centers in the central region was made due to resource constraints23. Study design This was a descriptive cross-sectional research design. The target population were outpatients presenting with a variety of illnesses at PHC centres. A trained psychiatric clinical officer and the first author, assisted by a psychiatric nurse and a clinical social worker, interviewed all those patients who gave informed consent. The first author trained all members of the research team on how to use the study instruments and in conduct of ethical research. The training and pre-test of the study procedure and instruments lasted for 4 days. Research assistants were unaware of the research questions of the study to minimise interviewing errors associated with bias. Sample size Sample size was calculated using the OpeniEpi open source calculator for proportions or descriptive studies. The source population for PHC centre patients in the study areas was assumed to be above 1,000,000 people. The hypothesized percentage frequency of poor QOL in the population was assumed to be 50% (plus or minus 5%), Confidence Limits were set at 95%, and Design effect was set at 1. Using these parameters, a sample size of 384 was derived. During fieldwork, the total number of respondents was increased by 16% to realize the actual study sample of 446 to take care of non-response. Besides, it is suggested that the WHOQOL-BREF should be used with a sample of at least 300 adult respondents for proper analysis 24. Study subjects The selected PHC centres (`Level IV') were providing free healthcare to mostly people with no or little incomes. Consecutive adult patients seeking healthcare at the outpatient departments (OPD) of each of the three PHC centre were eligible and asked to participate in the study. Study participants from selected health centres were ordinary people facing high levels of resource constraints23. Patients were recruited in the study as long as they met the inclusion criteria of; (i) being 18 years of age or older, (ii) being in position to talk in spite of the illness, and (iii) giving informed consent. Study instruments 1. Socio-demographic questionnaire All participants completed a demographic data sheet, which had questions on sex, age, marital status, religious affiliation, number of children, family size, educational attainment, occupation, and parenthood. 2. The World Health Organization Quality of Life Measure (The WHOQOL-BREF) The WHOQOL-BREF used in this study was developed as a brief tool for assessment of quality of life in field conditions. The WHOQOL Group initially developed a quality of life assessment instrument with 100 items, and tested it simultaneously in 15 field centres around the world. The best way of asking about quality of life was determined based on statements made by patients with a range of diseases, by healthy people, and by health professionals from various cultures. The WHOQOL-100 was rigorously tested to assess its validity and reliability in each of the field centres 25. Although the older WHOQOL-100 allows for a detailed assessment of each individual facet relating to quality of life, it was found to be too lengthy for practical use. The WHOQOL-BREF provides a valid and reliable alternative to the WHOQOL-100 for the assessment of domain profiles. The high reliability and validity of the WHOQOL-BREF has been documented for several populations worldwide26-28. The WHOQOL-BREF contains 2 items from the overall quality of life and general health facet and 1 item from each of the remaining 24 facets making a total of 26 question items. The 24 facets of QOL make up the four domains namely: physical health (Domain I), comprising 7 items; psychological well-being (Domain II), comprising 6 items; social relationships (Domain III), comprising 3 items; and environment (Domain IV), comprising 8 items. Question responses are rated on a five-point Likert scale (1-5). In this study, all items that were rated with a higher score indicating a higher or better QOL. Domain scores were calculated by multiplying the mean of all facet scores included in each domain by a factor of 4 in order to make the domain scores comparable with the scores used in the WHOQOL-100 24. Potential scores for each domain ranged from 4 to 20. The scoring was done in such a way that it produced a quality of life profile. Question item 1 which asks about an individual's overall perception of quality of life and question 2 which asks about an individual's overall perception of his/her health were examined separately because they do not fit in any of the four domains24. This instrument was used following the prescribed guidelines. Although the WHOQOL-BREF is supposed to be self-administered, it was interview-administered in this research since most of the respondents were either illiterate or semi-literate. The suggested reference time frame of QOL experienced within two weeks was used in the study24. Data collection Face-to-face interviews of respondents were conducted using Luganda, the commonly spoken Bantu dialect in the study area. All research instruments were translated from English to Luganda and blind back-translated by Luganda-speaking practicing psychiatric nurses. The nurses were also fluent in English; hence content validity was ensured and conceptual equivalence and cultural sensitivity were achieved. To attain face validity, the instrument was pre-tested on a sample of articulate respondents (not part of this study), that had similar demographic characteristics as the study participants. Appropriate changes were made after the pre-test. Conducting of interviews Interviews were conducted from July to October 2004. Interviewers were all professional mental health workers with prior experience in interviewing patients. They were given more training about the study, field surveys, data collection methods especially the interview method, dynamics of fieldwork, content of research instruments, and their ethical obligations as interviewers. All respondents were interviewed in private environments to avoid interruptions and to ensure confidentiality. Interviewers were tasked to ask questions audibly and to record responses. Ethical considerations Ethical clearances were obtained from the following sources: the Research and Ethics Committee of Makerere University Medical School (Uganda), the Human Research and Ethics Committee of Karolinska Institutet (Sweden), the Uganda National Council for Science and Technology Committee on study of Human Subjects, District Directors of Health Services in concerned districts, and the authorities in charge of the selected PHC centres. Conduct of the research team during the study adhered to the Helsinki Declaration. Participants in need of specialist attention were accordingly referred. Data management and statistical analyses Data was entered in EpiData Version 3 and exported to the Statistical Package for Social Scientists (SPSS) version 10.0 for cleaning and analysis. At a descriptive level, we compared males and females on the socio-demographics of age, marital status, religious affiliation, number of children, family size, educational attainment, occupation, and parenthood using a 2-way contingency table analyses (Pearson's chi-square statistic). We developed the four profiles of QOL using proportion scores for each. The Pearson's chi-square test and the Student's t-test were used to explorerelationships between variables. Stratified and multivariate backward stepwise logistic regression analysis was used to adjust for confounding of socio-demographic variables while evaluating the association between gender and quality of life assessment of patients across each of the four domains. Quality of life assessment for each of the four domains was entered as; poor = 1, good = 0. For all continuous variables, Means and Standard Deviations were generated. Level of significance was set at p < 0.05 and corresponding Odds Ratios were also generated. Results Demographic Description of Respondents This study had 446 respondents aged between 18 and 84 years (Mean = 31.9; SD = 12.1). Out of the total sample, females were 292 (65.5%) aged 18 to 70 years (Mean = 31.5; SD = 11.1) while males were 154 (34.5%) aged 18 to 84 years (Mean = 32.8; SD = 13.8) giving a female to male ratio of 1.7:1. There were few significant differences between male and female respondents (see Table 1). Concerning marital status, female respondents (35.7%) were married compared to 18.5% of male respondents. Compared to being married, both male respondents (48.7%) and female respondents (55.1%) were single by marital status. However, female respondents were more likely to be single. Compared to 15.6% of males, 26.4% of female respondents had been once married but separated as opposed to being married. In terms of family size, 42.8% of female respondents were from medium as opposed to 27.1% from small-sized households. For male respondents, 31.4% were from medium as opposed to 44.4% from small-sized households. Similarly, compared to 24.2% of males, more female respondents were from large households (30.1%). Although most respondents were parents, more male respondents (39.9%) tended to be non-parents compared to 20.2% of female respondents. In terms of occupation, more male respondents (42.2%) compared to 30.2% of female respondents tended to be regular income earners as opposed to peasants. There was no statistically significant gender difference on number of children in a home; male respondents had a mean number of 3.82 children (SD = 3.52) and female respondents had a mean number of 3.82 children (SD = 2.93) (t = 1.03; p = 0.99). The statistically significant sex difference was on number of other people in respondents' households; male respondents lived with a mean number of 4.46 other people (SD = 3.22) and female respondents lived with a mean number of 5.52 other people (SD = 3.22) (t= 3.3; p = 0.001). General QOL and Satisfaction with Life by Sex Comparison between male and female respondents shows no significant differences in terms of the way they rated their over all QOL and general satisfaction with health. On a range of 4.57 to 20.00, the mean score for the physical health domain of QOL was 12.34 (SD = 2.63). The range for the psychological well-being domain was 6.67 to 18.67 with a mean score of 13.04 (SD = 2.28). The range for the social relationships domain was 5.33 to 20.00 with a mean score of 12.90 (SD = 2.89). The range for the environment domain was 6.50 to 17.50 with a mean score of 11.9 (SD = 2.08) (Figure 1). Using the Independent-Samples t-test for equality of means, no statistically significant gender difference on each of the QOL domains was found. Males had a mean score of 12.09 (SD = 2.66) on the physical health domain, 12.47 (SD = 2.32) on the psychological well-being domain, 12.97 (SD = 2.86) on the social relationships domain, and 11.84 (SD = 2.13) on the environment domain. On the other hand, females had a mean score of 12.47 (SD = 2.60) on the physical health domain, 13.16 (SD = 2.25) on psychological well-being domain, 12.86 (SD = 2.91) on the social relationships domain, and 11.87 (SD = 2.06) on the environment domain. Contents of Each of the Domains of QOL Comparison of the individual domains of WHOQOL-BREF was reinforced by comparing individual question items on the basis of gender of respondents and the findings are presented in Table 3. For those who responded to the question on the extent to which physical pain and discomfort had limited their functioning, the proportion of females with a score of poor QOL was as high as 47.3% compared to 38.9% of male respondents. Conversely, the response to the question about whether respondents had had enough energy for everyday life, theproportion of males with a score of poor QOL was as high as 37% compared to 29.8% for females. Similarly, for those who responded to the question on how much respondents felt that they had enjoyed their lives, the proportion of male respondents that had a score of poor QOL was 45.5% compared 34.2% of the females. Looking at whether respondents often had negative feelings such as a blue mood, despair, anxiety or depression, the proportion of female respondents that had a score of good QOL was 63% compared to 53.2% of male respondents. For those who responded to the question on how satisfied they were with their transport, the proportion of female respondents that had a score of poor QOL was 26.7% compared to 17.5% of male respondents. Gender-based Stratified Analysis of QOL Looking at scores for each of the domains of the WHOQOL-BREF scale, the mean for each of the domains was used to determine good versus poor QOL. All respondents that scored above the mean were taken to have a good QOL on each of the four domains. In a stratified analysis, the association between each of the domains of QOL in terms of poor QOL or good QOL profile and demographic characteristics with a p-value of < 0.1 at bivariate analysis was analyzed by looking at whether Odds Ratios differed significantly. The stratification variable for this analysis was sex. There were no statistically significant differences between profiles of QOL for psychological well-being, social relationships and environment domains. The only exception was that for the physical health domain, there was a statistically significant difference on the variable of parenthood (Crude OR 1.63: 95 % CI: 1.06 2.51, p = 0.025) (see Table 4). Most patients at PHC centres that were parents appeared to perform poorly on this domain of WHOQOL-BREF. It was found that the likelihood of performing poorly on the physical health domain of WHOQOL-BREF was positively associated with female gender (Adjusted OR 2.47: 95 % CI: 1.32 4.61). Demographic Factors Associated with QOL Multivariate analysis was done to assess the association between different demographic variables (p < 0.10 at bivariate analysis) as probable predictors of poor QOL on each of the four domains in the WHOQOL-BREF. The demographic variables of being single, married, once married but separated, peasants, regular income earners, having no formal job, small family size (1 to 3 members), big family size (7 or more members), age category of 18-29 years, age category of 60-69 years, parenthood status, having no formal education and having secondary education were entered in a binary logistic regression. For psychological well-being, social relationships and environment domains of WHOQOL-BREF, none of the demographic variables appeared to be significantly associated with poor QOL. However, some demographic variables showed a statistical trend towards a positive association with the physical health domain. The final step in the logistic regression model for the physical health domain as an outcome showed that being in the age range of 18 to 29 years (Adjusted OR 1.74; 95% CI: 1.13 2.68, p = 0.012) and being a parent (Adjusted OR 2.12; 95% CI: 1.27 3.55, p = 0.004) had a positive association. Other probable predictors in the final step of the logistic regression like belonging to a small family of 1 to 3 members (Adjusted OR 0.66; 95% CI: 0.43 1.02, p = 0.060) and being male by sex (Adjusted OR 1.43; 95% CI: 0.0.95 2.18, p = 0.090) showed a positive trend. Discussion The aim of this study was to analyze the QOL in patients presenting at PHC centres and to identify gender differences. In a resource-constrained society like Uganda, QOL assessments have been proposed as a good source of outcome measures for care and support programs as well as assessing patients' satisfaction with health services 29. Our findings suggest that there was no statistically significant difference between male and female profiles of QOL in the domains of psychological well-being, social relationships and environment, which is consistent with research done elsewhere 2, 5. This was also comparable to a finding of subtle differences on the economic dimension of living between men and women in another study 30. However, male and female patients in this study never significantly differed in physical health complaints presented at the health centres. This was contrary to a study of women living with HIV/AIDS in India who scored significantly lower than same sero-status men on the Mean of psychosocial well being 29. In the Indian study, men and women reported similar scores only in dimensions of physical well-being, satisfaction with health care, and relationship with a partner. Although it is possible that that some of the study participants in our study could have been living with HIV/AIDS, many of them had other physical health complaints, notably; fevers, sexually transmitted infections, body aches, respiratory infections like coughs, abdominal pains like ulcers, allergic reactions like itchy skin, worries about hypertension, dental problems, injuries and many others that bothered them as earlier noted 31. Therefore, the main concern could justifiably have been physical health rather than any psychological well-being. In a qualitative study of caregivers' experiences with major depression concealed by physical illness in patients recruited from central Ugandan PHC centres, complaints of patients were reported to be more on the physical health spectrum 32. There was a statistically significant difference between males and females on the physical health domain QOL profile. Female respondents reported a poorer QOL on the physical health domain compared to males. This finding agrees with the observation that women consistently report poorer health-related quality of life (HRQoL) than men in patients found in primary care, and patients with chronic conditions in the US population 33. After adjustment, it was found that the likelihood of reporting poor physical health had a positive association with the female sex. This in a way supports the assertion of a gender perspective of health determinants and justifies the need for health-related QOL to often be taken into account 5. Likewise, females study participants reported that they had significantly bigger families compared to men, possibly due to their magnanimous attitude towards care-giving. Although this explanation may not be definitive in this study, one can speculate that women reach out more to many extended family relations. Secondly, females were more likely to be either single or once married but separated, more likely to belong to either medium-sized or large-sized households, more likely to be parents and more likely to be either peasants or without a formal job. The explanation could be that; traditionally it is easier for separated or widowed men to remarry, to determine the size of their families and to have an income generating activity compared to females. The implication could be that female patients reported their physical health to be poorer because as traditional caregivers in households, they not only hadphysical ill-health but were also bothered by the likelihood of supporting many dependants as earlier reported 34. In logistic regression, belonging to the age category of 18-29 years was positively associated with a poor physical health domain of QOL. Similarly, being a parent was positively associated with poor a physical health domain QOL. Given the societal trends in Uganda, rural females are more often less educated, more likely to fall in the age range of 18-29 years, to be parents, and to have comparatively more children than those from other societies 35. Therefore, poor physical health found among female attendees of PHC centres could have been a result of the stresses and pressures associated with such dynamics. This study has a number of methodological limitations, which should be borne in mind while interpreting the findings. Taking the whole of Uganda into perspective, the study areas were relatively few and the sample size was relatively small thereby limiting the power of the study. Therefore, the likely generalizability of the findings is limited since the study was done in the central region of Uganda with largely one predominant ethnic group. Future researchers would do well by studying bigger samples. The research design was cross-sectional; hence no inferences about the direction of the observed relationship between QOL and gender could be made. This was a convenience sample of consecutive patients presenting themselves at PHC centres; thus the group had characteristics of a referred (self or otherwise), rather than an epidemiological sample. However, the data collected and the consequent interpretation of findings are reasonably valid and reliable and should be taken as a starting point for further research. Future studies should be interventional and should adopt a longitudinal research design to the assessment of QOL in order to identify potentially modifiable risk factors for poor QOL. Since Ugandan women play an important role as nurturers and caregivers within the family setting, future studies should examine the impact of ill-health on their social roles as wives, daughters, daughters-in-law and mothers. The WHOQOL-BREF used in this study is a cross-cultural tool that has been validated in several societies 26-28. Although not yet validated in Uganda's multicultural setting, a consistent and rigorous adaptation process was employed to take care of cultural differences. This included translation of the tool into Luganda and blind back-translation to English in a way that ensured conceptual equivalence, cultural sensitivity and validity as explained in earlier publications 31, 36-38 Conclusion Evidence suggests that QOL constitutes an important area of research. Our findings suggest that the WHOQOL-BREF can be successfully administered and responded to by people seeking healthcare at PHC centres in Uganda. Although women that go to PHC centres in central Uganda reported comparatively similar QOL as men, it is important to note that women appeared to report poorer physical health. Although it is important to design interventions to improve the QOL of especially women, there is need to appreciate the complexities of physical, psychological and cultural factors affecting the QOL of Ugandan women, particularly those that have physical illnesses. Health workers in Uganda need orientation and/or training to appreciate the role of gender in healthcare. Whether psychosocial or pharmacological, interventions aimed at improving the QOL of patients seen at PHC centres should take a gender-based perspective and recognize the special vulnerability of women with respect to poor physical health. Acknowledgements This article is from a dataset on "Profiles of Depressive Illness in the Lake Victoria basin" (Uganda), which was a collaborative research project between the Department of Psychiatry at Makerere University and the Department of Clinical Neuroscience, Section of Psychiatry, at Karolinska Insitutet (Sweden). We thank the Swedish Government for funding the project through Sida/SAREC. We thank Professor Hans Ågren for his insights in planning the research protocol, fieldwork and data analysis. We also wish to thank interviewers and all study participants for having made this research possible. References
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10069t2.jpg] [hs10069t1.jpg] [hs10069t4.jpg] [hs10069f1.jpg] [hs10069t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}