 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
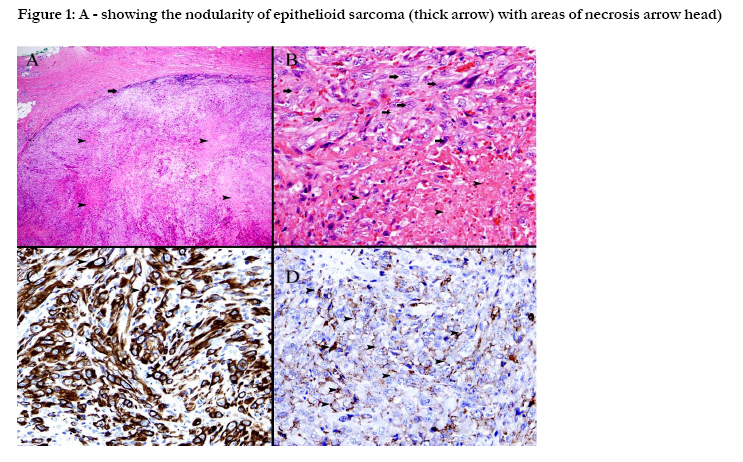
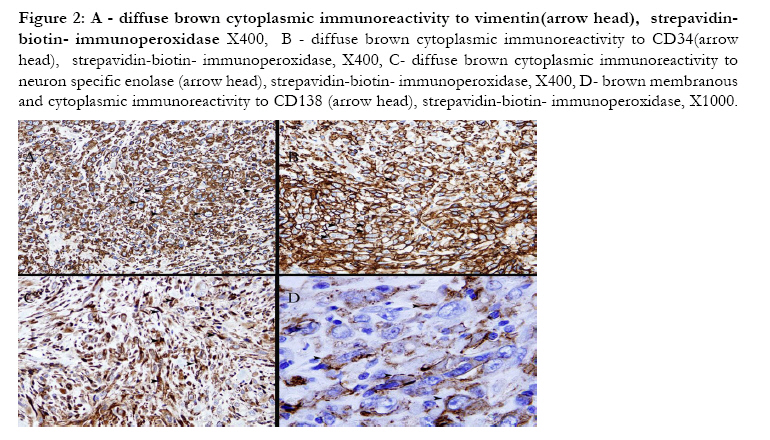
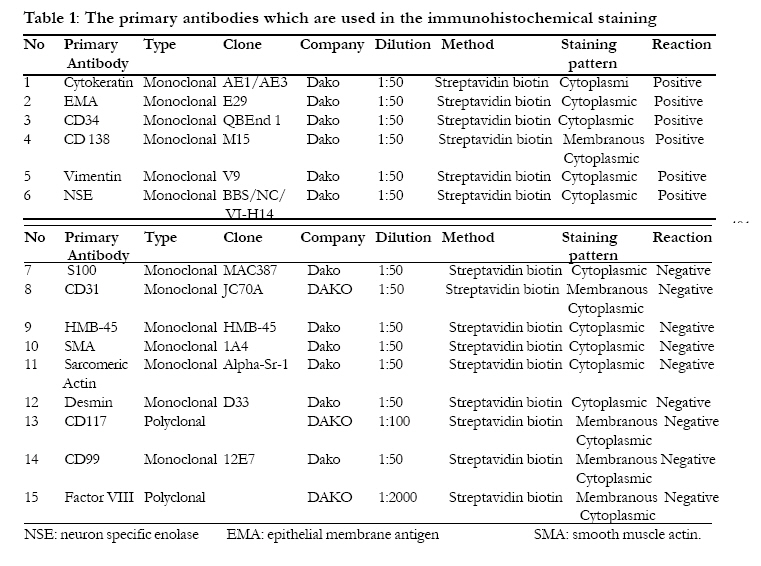
African Health Sciences, Vol. 10, No. 4, December, 2010, pp. 400-404 Epithelioid Sarcoma in a child presenting as a submandibular mass *Al-Salam S1, Al Ashari M2 1Pathology department, Faculty of Medicine and health Sciences,
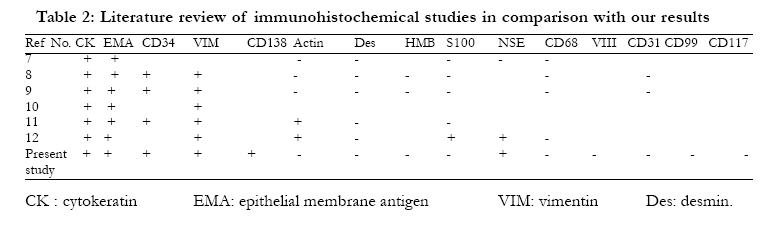
United Arab Emirates University Al Ain, UAE *Corresponding author: Dr. Suhail Al-Salam MD, Assistant Professor and Consultant Pathologist, Pathology department, Faculty of medicine and health Sciences, United Arab Emirates University, Al Ain, UAE, Tel: 0097137672000 Ext-464 Fax: 0097137671966 E-mail: suhaila@uaeu.ac.ae Code Number: hs10073 Key words: Soft tissue sarcoma; Epithelioid sarcoma; Paediatric; Submandibular Epithelioid sarcoma (ES) is a clinical curiosity with uncertain histogenesis1. Histologically, two variants have been described: the "classic or distal" variant, which usually affects distal extremities of adolescents and young adults between 15 and 35 years of age , particularly in the hand and foot, and consists of a subcutaneous or deeper nodular proliferation of rounded to plump cells with abundant eosinophilic cytoplasm palisading around areas of necrosis2, while the "proximal" variant , first described in 1997 by Guillou et al. 3, is found mostly in the pelvic, perineal, and genital tracts of young to middle-aged adults and characterized by a proliferation of epithelioid-like cells with rhabdoid features in the absence of a granuloma-like pattern. In this monograph we report a case of pediatric epithelioid sarcoma presented as a submandibular mass and to the best of our knowledge it has not been previously documented in this place. A nine year old female child presented with a firm fixed lobulated mass near the left angle of the mandible with a provisional diagnosis of enlarged submandibular lymph node. Fine needle aspiration cytology (FNAC) of the mass was performed and revealed a spindle cell lesion with myxoid back ground suggestive of nodular fasciitis. Excisional biopsy of the mass was done. A round, lobulated mass was received measuring 4x3x3cm, cut sections were homogenous with foci of necrosis. Histologically, the tumor cells have nodular proliferation (Fig. 1A) of large polygonal to spindle-shaped cells with epithelioid appearance and abundant eosinophilic cytoplasm palisading around areas of necrosis and simulating a granulomatous process (Fig. 1B). The tumor cells were uniformly immunoreactive to cytokeratin (CK) (Fig. 1C), epithelial membrane antigen (EMA) (Fig. 1D), vimentin (Fig. 2A), CD34 (Fig. 2B), neuron-specific enolase (NSE) (Fig. 2C), and CD 138 (Fig. 2D). The tumor cells showed no immunoreactivity to S-100 protein, HMB-45, smooth muscle actin (SMA), sarcomeric actin, desmin, CD31, factor VIII, CD99 and CD117 (Table 1). The patient had an uneventful postoperative recovery with no recurrence after one year of follow-up. No adjuvant chemotherapy or radiotherapy was given to the patient. Figure 1: A - showing the nodularity of epithelioid sarcoma (thick arrow) with areas of necrosis arrow head) H&E X 100 B - showing large polygonal cells with epithelioid appearance (thick arrows)and abundant eosinophilic cytoplasm palisading around areas of necrosis (arrow head)and simulating a granulomatous process, H&E, X400, C showing diffuse brown cytoplasmic immunoreactivity to cytokeratin (arrow head), strepavidin-biotin- immunoperoxidase, X400, D - showing brown membranous and cytoplasmic immunoreactivity to epithelial membrane antigen(arrow head), strepavidin-biotin- immunoperoxidase, X400. It was only after Enzinger's report of sixty two cases in 19704 that ES received widespread recognition as a distinctive tumor type. ES is notorious for being misdiagnosed5. Our patient was clinically misdiagnosed as enlarged submandibular lymphnode, since the mass had a round and smooth contour with firm consistency making it similar to an enlarged lymphnode. Furthermore, the FNAC was misleading too showing features of spindle cells with myxoid background; non-specific features leading to a wrong diagnosis. The use of FNAC as a diagnostic modality for the pathologic evaluation of soft tissue neoplasms is uncommon and controversial6. Paediatric ESs are rare neoplasms. More than seventy cases of paediatric ES have been documented1-12, however, no report of ES in the submandibular region. It is noteworthy to mention here that the tumor in our patient shows both histological and behavioral features of distal type of ES despite its occurrence in a proximal area. The immunohistochemical profile of ES is quite interesting and shows immunoreactivity to CK, EMA, CD34, Vimentin, NSE, and CD138. Many immunohistochemical studies7-12 have shown similar staining patterns (Table 2), however, none have reported CD138 expression in ES, which is to best of our knowledge, the first time being documented in ES. CD138 (Syndecan-1) is a cell-surface heparan sulfate proteoglycan, that links the cytoskeleton to the interstitial matrix and plays a role in cellular adhesion and proliferation processes. Via its heparan sulphate chains, CD138 binds to a variety of growth and angiogenic factors and acts as a classical co-receptor for growth factor receptors, thus promoting cell proliferation and tumor formation13. ES is usually confused histologically with a variety of lesions including; granulamatous lesions, rheumatoid nodules, fibromatosis, an ulcerating squamous cell carcinoma and soft tissue sarcomas with epithelioid features such as angiosarcoma, malignant peripheral nerve sheath tumor (MPNST), rhabdomyosarcoma, leiomyosarcoma and synovial sarcoma (SS) 11. Both morphological and immunohistochemical staining patterns are helpful in solving the differential diagnosis. The negative immunoreactivity to CD68 differentiates epithelioid sarcoma from granulomatous processes, rheumatoid nodule and other histiocytic lesions. The immunoreactivity to CK, EMA, CD34 and vimentin differentiates epithelioid sarcoma from squamous cell carcinoma and other epithelial tumors11, while the combination of negative immunoreactivity to CD31, factor VIII, S100, SMA and desmin with positive immunoreactivity to CK, EMA, CD34 and vimentin rules out angiosarcoma, MPNST, rhabdomyosarcoma and leiomyosarcoma. The differentiation from SS is very difficult since they almost have similar immunohistochemical prolfile. However, absence of the biphasic pattern, nodularity with central necrosis, well circumscription and absence of immunoreactivity to CD99 can differentiate ES from SS. In addition, SS is characterized by the presence of SYT-SSX fusion oncogene. Demonstration of the t(X;18) by cytogenetics or fluorescence in situ hybridization will enable us to differentiate between synovial sarcoma and ES. Moreover, TLE expression is a consistent feature of SS14. The origin of ES remains controversial1-12. A recent analysis of the immunohistochemical pattern of both epithelial and mesenchymal markers led to the conclusion that ES is a mesenchymal tumor capable of partial epithelial transformation15. ES is known to recur and metastasize even after wide excision and the reported metastatic rate is between 30% and 45%1,2,4,5. The tumor metastasizes through lymphatic and blood vessels to regional lymph nodes, skin, lungs, heart, pleura, liver, pericardium, bone and soft tissue of the other parts of the body. Lungs are the most common site of distant metastasis1,5. Unlike most soft tissue sarcomas, the involvement of lymph nodes are frequently described1,5. Baratti et al. reported lymphnode metastasis in 30% of ES5. Surgery is the gold standard method of treatment. Adequate treatment requires radical en bloc excision as early as possible along with extensive lymph node dissection. The role of radiotherapy and chemotherapy is controversial1-12. Baratti et al. found no significant survival difference between patients who received and who did not receive adjuvant chemotherapy or radiotherapy5. In our patient, the mass was excised completely and no adjuvant therapy was given postoperatively. There was no evidence of local recurrence, lymph node involvement or distant metastasis for more than one year of clinical and radiological follow-up of our patient. Older age, male sex, proximal or axial location, depth, tumor size, mitotic figures, necrosis, vascular invasion, tumor haemorrhage , local recurrence, nodal metastases, and the extent of surgery, were identified as adverse prognostic factors5. Conclusion ES can occur in the submandibular region and can show both histological and behavioral features of the distal type despite its occurrence in a proximal site. References
Copyright 2010 - African Health Sciences The following images related to this document are available:Photo images[hs10073t2.jpg] [hs10073f1.jpg] [hs10073t1.jpg] [hs10073f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}