 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Rheumatic manifestations among HIV positive adults attending the Infectious disease clinic at Mulago hospital *Kaddu-Mukasa M1, Ssekasanvu E 1, Ddumba E1, Thomas D2, Katabira ET1 1Department of Medicine, College of Health Sciences, Makerere University Code Number: hs11004 AbstractBackground: Rheumatic manifestations in HIV are common and sometimes the initial presentation of
the disease. HIV is now a common infection at the Infectious Disease Clinic, Mulago. The spectrum of
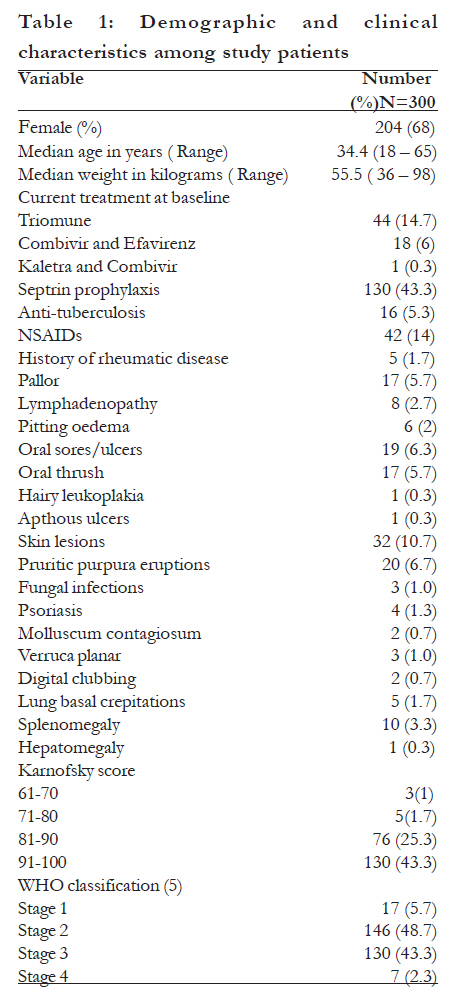
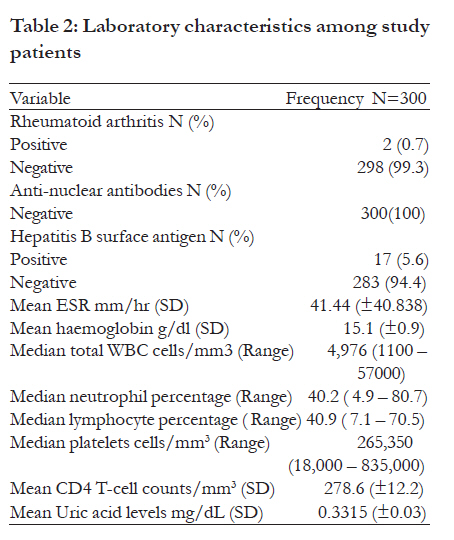
joint diseases seen depend on a number of factors such as, the CD4 count, HLA status and current therapy. Key words: rheumatic manifestations, hiv and arthritis Introduction The national HIV prevalence is estimated to be 6.2% of the total Ugandan population1. HIV infected individuals have an increased risk of developing musculoskeletal disease2. Wide spectrums of clinical manifestations involving different systems have been reported during HIV infection. Rheumatic manifestations are among the most common features associated with HIV, often the primary presentation within this group. Rheumatic conditions such as reactive arthritis, psoriatic arthritis, ankylosing spondylitis, undifferentiated spondyloarthropathy, polymyositis, vasculitides, septic arthritis and pyomyositis have been described in association with HIV3,4. Estimates of the exact prevalence of rheumatic manifestations of HIV infection vary widely. This is the first study reporting the prevalence and clinical rheumatic manifestations among Ugandan patients with HIV infection.Methods This cross-sectional study was conducted at the Infectious Disease Clinic, Department of Medicine, Makerere Medical School (IDI-MU) from October 2005 to February 2006. Four hundred eighty seven patients attending the IDI-MU were screened for eligibility to participate in the study. The eligibility criteria were: (1) documented HIV-1 infection; (2) age 18 years and above; (3) willingness to provide informed consent; (4) No history of recent trauma to the joints within the previous two weeks. Three hundred HIV positive patients were recruited into the study using systematic consecutive sampling. Patients were evaluated for rheumatic diseases, their clinical and laboratory findings documented. We compared the clinical and laboratory simultaneously among the subjects with rheumatic diseases and those without.According to drug access policy in the Infectious Disease Clinic, HAART was essentially initiated for patients with CD4 counts <200 cells/uL and for those with any clinical condition classified as AIDS (WHO clinical stage 3 or 4). All the subjects recruited into the study received Trimethoprim-sulfamethoxazole prophylaxis in accordance with the IDI guidelines. Routinely, all patients are followed by their physicians on a monthly interval basis (clinical observation for all plus HAART renewal for treated patients). They are also allowed to return to see the physicians without prior appointment for any problem occurring between two scheduled visits. Quantitative adherence to HAART was estimated by the number of doses taken during the 30 days prior to the follow-up visit, divided by the number that should have been taken, and expressed as a percentage. Adherence levels of e"95% are considered as acceptable. Patients were also asked if they were taking the drugs at the right time. Antiretroviral therapy is monitored by clinical and immunologic responses. CD4+ cell count measured every six months and viral load is not routinely performed. A weekly switch meeting is held to discuss patients who appear to be failing on the first line therapies. Written informed consent was obtained before recruitment into the study. The subject's demographics, clinical examination as well as a detailed rheumatologic examination performed by the investigators were recorded in a structured questionnaire. Blood samples were drawn for rheumatologic studies which included the Rheumatoid factor by latex agglutination test titers more than 1: 80 was considered positive. Anti nuclear antibodies (ANA) studies were by indirect immunofloresence using Hep-2 cells, titers above 1:160 were taken as ANA-positive. Hepatitis B surface antigen reactivity was measured using diagnostic kits from Cypress diagnostics, Langdorp, Belgium. The full hemogram was done with a Beckmann Coulter ACT 5 diff analyzer, California, USA while the erythrocyte sedimentation rate (ESR) in the first hour was measured with Westergren method. CD8+ and CD4+ lymphocyte measurements were done using a FacsCalibur instrument (Becton Dickinson San Jose, California, USA). The uric acid levels were measured using Bio Medica Diagnostics 3300, Nova Scotia, Canada. Subjects who had joint involvement had radiographs taken to assess the extent of joint involvement as well as erosions, osteoporosis and subchondral cysts. Statistical analysis: The data was coded, entered and verified with double entry using Epi-info 6.04. Statistical analysis was performed using the Statistical Package for the Social Sciences, version 10.0 (SPSS, Chicago, IL, USA) and STATA 8.0 (StataCorp LP, Texas, USA). Continuous data was summarized using means and standard deviations (SD) and compared using t tests. Categorical variables were compared using chi-square test. A p value of <0.05 was considered significant. Funding source and ethical approval The study was funded by the Infectious Disease Institute The study was approved by the Scientific Review Committee of the Infectious Disease Institute and Makerere University Faculty of Medicine Research and Ethics Committee. ResultsSocio-demographic and clinical characteristics of study patients A total of four hundred eighty seven subjects were screened, however 300 subjects were enrolled into the study. One hundred twenty seven (67.9%) were participating in other ongoing studies while 34(18.2%) refusal to consent and 26(13.9%) failure to comprehend study information. Out of the three hundred subjects, two hundred and four (68%) were females. The age ranged between 18 65 years (median 34.4 ± 8.3 years). The median weight was 55.50 kilograms (Range, 36 98). Five patients (1.7%) of the patients enrolled into the study had a prior diagnosis of rheumatic diseases; one of the subjects carried a diagnosis of rheumatoid arthritis, while another had a diagnosis of gouty arthritis. The other three (3) were unsure of prior diagnoses made, but they attended regular specialised care in rheumatology clinic of the National referral hospital. None of the patients in the study had a history of rheumatic heart disease. One hundred thirty (130) of three hundred (43.3%) were on Septrin prophylaxis while 21% were on antiretroviral therapy. Forty four (14.7%) were on Triomune (Stavudine, Lamuvidine and Nevirapine), six percent (6%) on Combivir (AZT, 3TC) and Efavirenz, while one patient (0.3%) was on Kaletra and Combivir. Sixteen patients (5.3%) were receiving anti-tuberculous therapy regimen containing Pyrazinamide and Isoniazid. Forty patients were taking non-steroidal anti-inflammatory drugs. Eighty one (81) patients had symptoms related to rheumatologic diseases with a mean duration of the symptoms as 14 ± 57 days. The commonest joints involved were the knees (28.8%) and ankles (26.9%), Of the 81 patients, 57.1% had tenderness, swelling 28.6%, crepitus and deformity both 4.1%. Forty eight point seven percent were stage 2 while 43.3% were stage 3 according to the Interim proposal for World Health Organisation Staging System for HIV infection and Disease (5) as shown in table 1.Laboratory characteristics and diagnosis made The mean ESR was raised at 41.4 ± 40.8mm/hr, mean haemoglobin was normal 15.1±0.99g/dl. Mean CD4 T-cell count was 278.6 ± 12.23/mm3 and uric acid 0.33 ± 0.03mg/dl. Rheumatoid factor was positive in two (2) patients and the anti-nuclear antibodies were negative in all study patients. Hepatitis B surface antigen was positive in 17 out of 300 (5.6%) patients. Synovial fluid aspirates were performed for 10 subjects and three (3) patients had septic arthritis with Staphylococcal organisms cultured. Four (4) had non-inflammatory arthritis with a negative gram stain, polymorhs < 25% and WBC counts ranging between 200 2000 /mm3. Three (3) had inflammatory arthritis with synovial fluid leukocytes > 2500 cells/mm3. Radiographs taken of the affected joints did not reveal any erosions or reduction in joint space, subchondral cysts or osteoporotic bones. The rheumatic manifestations using the American College of Rheumatology Criteria found among the study patients are as follows. The most common was arthralgias at 19.3%, followed by HIV associated arthritis (4.3%), 1% septic arthritis, 1 % Psoriatic arthritis, 0.7% rheumatoid arthritis and 0.3% Osteoarthritis. (Table 2)Clinical and laboratory comparisons between groups with and those without rheumatic manifestations in HIV infected patients. The mean age was not statistically different 36.46years in those with rheumatic manifestations and 33.69 in those without. There were no differences between the two groups regarding sex distribution. Patients with a prior diagnosis of rheumatologic disease were more likely to have a rheumatic manifestation in the setting of HIV, (p-value 0.001, OR 1.0, 95% CI 1.0 1.13). Patients taking anti-tuberculosis therapy (Rifampicin, Isoniazid, ethambutol and Pyrazinamide) were more likely to have a rheumatic manifestation (p-value 0.016, OR 3.78, 95% CI 1.4 9.9). Only 21% of with rheumatic manifestations were on highly active anti-retroviral therapy and this was not significant (p-value 0.41, OR 0.52, 95% CI 0.14 1.82). Clinically pallor, lympadenopathy, oral ulcers, skin lesions, digital clubbing, lung crepitations and splenomegaly were not statistically different in occurrence between the two groups of patients. 13.8% of patients had bilateral pitting oedema compared to 3.1% without rheumatic manifestations. Those with pedal oedema were more likely to have rheumatic manifestations p-value 0.0027, OR 5.41, 95% CI 1.01 28.96). No association was found between rheumatoid factor and rheumatic manifestations (p-value 0.4639, OR 2.73, 95% CI 0.17 44.08). All patients had a negative anti-nuclear antibody assay. Neutrophil counts were associated with rheumatic manifestations with a p-value of 0.0175. Patients with rheumatic manifestations had negative correlation with neutrophils counts and uric acid levels of -0.14 and -0.1 respectively. Other laboratory results were not associated with rheumatic manifestations. CD4 cell counts were not associated with rheumatic manifestations (p-value 0.5311) Discussion The diagnosis of rheumatic manifestations or diseases in the setting of HIV can be challenging especially in a resource limited setting. Results from this study show a high prevalence of 27% of musculoskeletal involvement this is comparable to other studies. The most common rheumatic manifestation was arthralgias and this was common in patients receiving anti-tuberculosis therapy. This may have been due to Pyrazinamide inhibiting renal tubular secretion of uric acid through its main metabolite pyrazinoic acid. This leads to hyperuricemia producing non-gouty poly-arthralgias poorly responsive to Allopurinol6-8. Though uric acid was not associated with rheumatic manifestations and was negatively correlated in this study. The possibilities of co-current renal disturbances and HIV associated nephropathy might have involved in this. We were unable to confirm this as serum creatinine and urine biochemical analyses were not performed.No association was observed with the use of highly active anti-retroviral therapy (HAART) in this study possibly because of small number of subjects with exposure. Only 62 patients were on HAART; however other studies have reported a shift in the clinical spectrum with patients presenting with osteonecrosis and non-HIV associated malignancies with a relatively high prevalence3,9. The use of prophylactic measures of using Septrin for the prevention of opportunistic infections such as genitourinary and enteric infections may have an effect on the rheumatic manifestations as previously described manifestations such as Reiter's syndrome were uncommon in this study. All subjects recruited in this study were receiving Septrin prophylaxis. Earlier studies elsewhere found prevalence rates of 0.4 11%4,10-12 The involvement of knees and ankles compared to other joints has been described earlier4,10,13. Fifty seven percent of these joints involved were tender on palpation and 28.6% were swollen. The pathogenesis of the tenderness remains to be elucidated, but theories have been suggested that cytokines, formation and deposition of immune complexes within the joint and transient bone ischemia might be responsible12. Septic arthritis was observed in 1% of the study patients and staphylococcal infection was found. This is lower than previous studies which have reported higher incidences of septic arthritis in this group, probably due to the different study settings. None of the patients with rheumatic manifestations fitted into the classical description or incomplete Reiter's syndrome14. Prophylactic use of Septrin might have an important role to play in controlling the probable enteric and venereal infections implicated to play a role in the pathogenesis. We did not attempt to isolate or perform Polymerase Chain reaction (PCR) to detect the presence of possible enteric or genitourinary tract infections as well as follow up participants to determine the response to NSAIDs or antibiotics. This might explain why Reiter's syndrome was uncommon in this study. Rheumatoid factor was negative in 99.3% of the study subjects, which is similar to earlier studies15,16 Patients with a prior diagnosis of rheumatologic disease before becoming HIV positive were more likely to have a rheumatic manifestation in the setting of HIV especially if the CD4 cell counts are still above 200 cells. Previously damaged joint tissues due to the earlier chronic inflammation increase the risk for septic arthritis as well as recurrent arthralgias17,18. One of the two patients with Rheumatoid arthritis reported a reduction in the severity of the disease. This is in keeping with the pathogenesis of rheumatoid arthritis as the CD4 T-cells counts drop17,19. Anti-nuclear antibodies were negative in all patients, this is similar to findings to work by11,16. Conclusion HIV positive patients commonly present with rheumatic manifestations. Usually the larger joints are affected more than smaller joints. Clinicians offering health care to HIV positive patients need to be aware of the various clinical presentations and they need to keep a high level of suspicion. Acknowledgement We acknowledge the Infectious Disease Institute-Makerere University for funding this study, Makerere University-John Hopkins University laboratory staff and John Kyabbagu for the laboratory work. The study patients and staff of IDI-MU clinic for supporting this work.Potential conflict of interest: None directly related to this study for all authors. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11004t3.jpg] [hs11004t1.jpg] [hs11004t2.jpg] [hs11004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}