 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Knowledge of cervical cancer and screening practices of nurses at a regional hospital in Tanzania *Urasa M1,2, Darj E1 1Department of Women's and Children's Health, International Maternal and Child Health, Uppsala
University, Sweden. Code Number: hs11008 AbstractBackground: Cervical cancer, the most common cancer among women in Tanzania is strongly linked to Human
Papilloma Virus. Precancerous lesions can be detected by Papanicolau smear screening. Nurses, being the largest group of
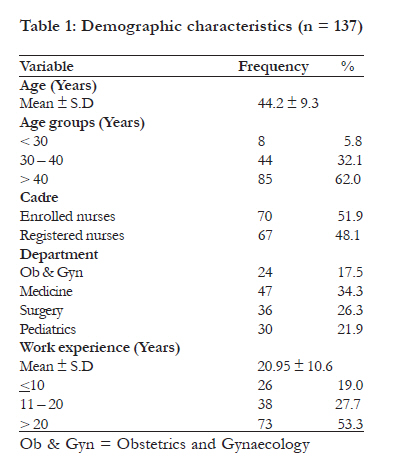
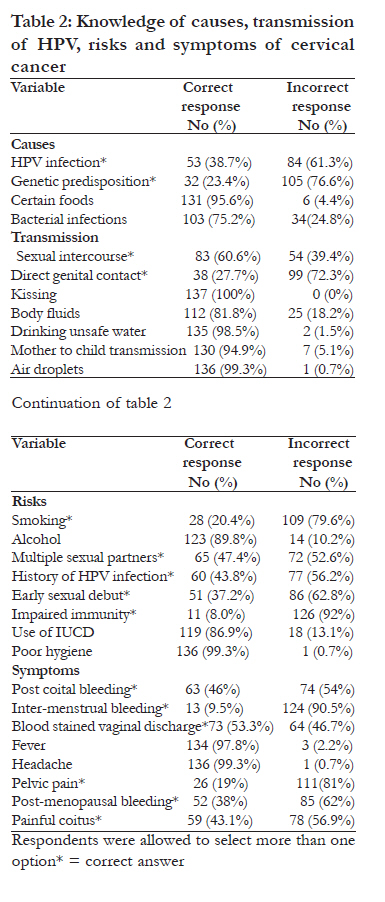
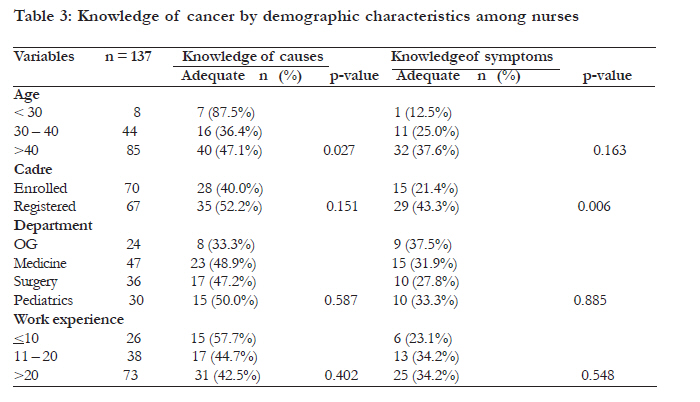
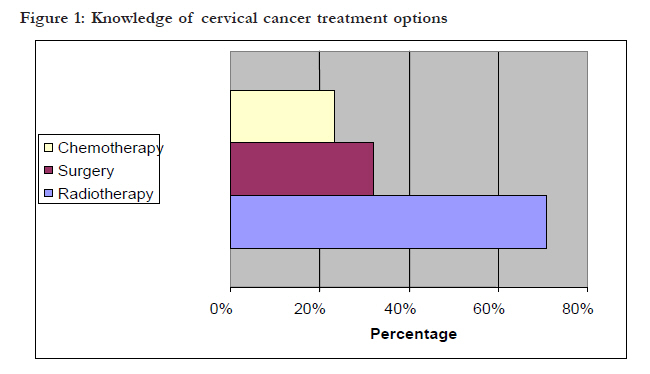
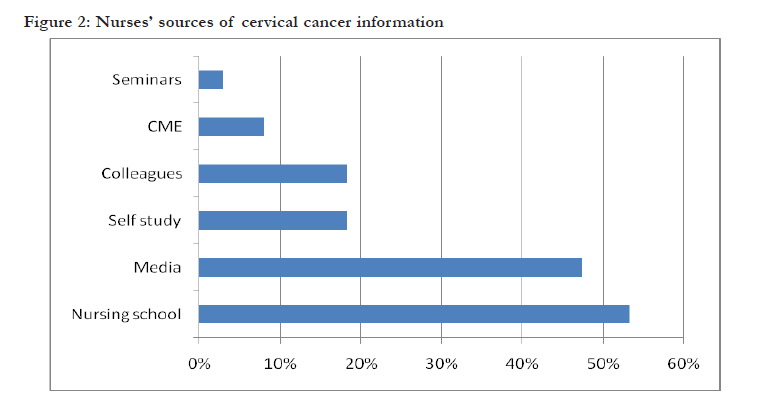
health workers, have an important role in promotion of cervical cancer screening. Key words: Cervical cancer, HPV, knowledge, nurses Introduction Cervical cancer is the second most common cancer in women worldwide (12%) following cancer of the breast; in developing countries however it is the most common cancer among women1. The majority of cervical cancer related deaths occur in developing countries. According to the WHO, 80% of the 288,000 deaths out of 471,000 new cases globally were from developing countries in 20002. In Tanzania where the population is approximately 40 million people, 11.4 million women within the reproductive age and beyond are at risk of developing carcinoma of the cervix. The WHO reports that cervical cancer's crude incidence rate in Tanzania is 40.6 per 100,000 women compared to 25.7 and 16 respective averages for the rest of East Africa and the world. Out of the 7515 cases reported in the country in 2002, a staggering 6009 (80%) died3. According to the Tanzania cancer registry, cervical cancer accounted for 29.8% of all cancers in females in Northern Tanzania between 1998 and 20004. The situation is complicated by the high prevalence of HIV which is estimated to be 8% in the general population, the proportion of women at risk is expected to be high as HIV infection is associated with a rapid progression of invasive cervical cancer5. There is strong epidemiologic evidence linking cervical cancer to the Human Papilloma Virus (HPV) sexually transmitted More than 35 types of the HPV are known to infect the genital tract out of which approximately 20 are associated with cervical cancer, with the most common types 16 and 18, and types 6 and 11 are more commonly associated with genital warts6,7. Early sexual debut, multiple sexual partners, HPV infection, smoking, genetic predisposition and compromised immunity are associated with development of cervical cancer1,6,8,9. Recent studies have shown a link between HIV-1 and invasive cervical cancer4,5. Morbidity and mortality related to cervical cancer can effectively be reduced by screening and eradicating pre-invasive disease as shown by studies done in developed countries. Studies have shown sensitivity and specificity of Pap smear screening to be 50-75% and 98-99% respectively2,6. Despite the availability of screening methods such as pap smears and HPV-DNA testing many women in low income countries do not have access to these services2,10. In these countries, visual inspection with acetic acid (VIA) which is a low cost method that does not require specialized know how is being advocated11. Studies have shown the sensitivity of VIA to be the same as that of Pap smear while its specificity is lower than 85%2. WHO has recommended its member countries to develop and integrate cervical cancer screening into their health systems depending on the local social, cultural and economic contexts. This will ensure a defined referral system for diagnosis, treatment and follow up11. The national health policy in Tanzania however does not have a screening policy for cervical cancer; priority is given to infectious diseases such as malaria, tuberculosis, leprosy, diarrheal diseases, acute respiratory infections and sexually transmitted infections all of which have individual control programs12. Treatment of cervical cancer is dependent on the stage of the disease, age and medical state of the patient, tumor characteristics,patients' preferences and resources within the health sector of each country. Options can be monotherapy or combined; they range from conisation of the cervix, simple hysterectomy with or without lymphadenectomy, radical hysterectomy with pelvic lymphadenectomy, pelvic exenteration, chemotherapy, radiotherapy, to palliative chemotherapy. Treatment at an early stage has the best prognosis with the highest cure rates13,14. HPV Vaccine The recent introduction of the HPV vaccine provides the opportunity to substantially reduce transmission of both high risk types 16, 18 and low risk types 6, 11 by doing so it will reduce not only morbidity and mortality related to cervical cancer, but also the financial burden brought about by diagnosis and treatment interventions12. It prevents infections when given to those with no previous exposure. Consequently it needs to be administered to adolescents before their sexual debut. Due to its high cost the vaccine is not available to the public in low income countries15-17. The aim of this study was to determine awareness of cervical cancer and screening practice among the nurses at a regional hospital in Tanzania. Specifically to determine levels of knowledge of transmission of HPV, causes of risks, treatment and prevention of cervical cancer. Furthermore, the association between knowledge and demographic characteristics and to determine the proportion of nurses who had been screened for cervical cancer, as well as the nurses' suggestions for improvement of cervical cancer knowledge.Methods Data collection was done in September 2009 at a hospital in northern Tanzania. It is a public institution fully owned and financed by the government with a 450 bed capacity serving a population of about 1.6 million people catering for 18 district hospitals from within and outside the region. Pap smear screening services are not available at any of the government hospitals in the region. Screening services are available at a religious affiliated private hospital and in a referral hospital in a nearby region approximately 80 km away.The hospital has 92 registered nurses (2 nurse officers with university degrees, 10 with advanced diplomas and 80 with diplomas of nursing), 116 enrolled nurses (with certificate in midwifery), 127 nurse auxiliaries and 5 Maternal and child health aides (MCHA). Although the nurse auxiliaries make up the largest group of "nurses", they were excluded, because their training, for one year, aims for ward attendance only. Participants in this study were 67 registered and 70 enrolled female nurses from the departments of Obstetrics & Gynecology, Internal medicine, Surgery and Pediatrics. This was a descriptive cross sectional study. The sample size was 137 respondents determined by the Kish and Leslie formula. Respondents were selected by systematic random sampling technique weighted according to the representation of the nursing cadre among all nurses at the hospital. Two lists of registered and enrolled nurses were made in alphabetic order, the first names on both lists were included followed by every other name on the list. A self administered questionnaire in Swahili language was distributed to the nurses and collected by the principal investigator during shift changes and tea breaks. Dependant variables were categorized into adequate and inadequate using a scoring system. This study measured nurses' knowledge of HPV transmission, causes, risk factors, symptoms, treatment and prevention of cervical cancer. Nurses' own screening practices was also measured. Continuous variables such as age and work experience (duration of employment) were categorized according to the results of the study. To ensure clarity the questionnaire was pre-tested on nurses at a health centre the nurses who took part in the pre test were not included in the study. Ethical clearance for the study was obtained from the National Institute of Medical Research in Tanzania. Permission to carry out the study was sought from the Regional Medical Officer and the hospital's Medical Officer in charge. Oral consent was obtained from respondents after the objectives of the study were explained and confidentiality ensured. Data were entered and analyzed by the researcher using the Statistical Package for Social Sciences (SPSS) version 16. The results are presented as frequency tables and means. Chi square tests were made to find associations between the dependent and independent variables with significance set at <0.05. Results A total of 137 respondents were included in this study. The mean age of the participating nurses was 44.2 years (S.D ± 9.3). Nurses aged more than 40 years constituted the majority (62%). Enrolled and registered nurses made up 51.9% and 48.1% respectively of the study sample. The department of Medicine had the largest representation of nurses (34.3%) while the department of Obstetrics and Gynecology had the smallest (17.5%). The mean duration of working experience was 21 years (S.D ±10.6). Nurses with more than 20 years of working experience made up the largest proportion (53.3%) (table 1). Knowledge of cervical cancer Table 2 shows knowledge of transmission of HPV, causes, risk factors and symptoms of cervical cancer. HPV infection and genetic predisposition were correctly identified by 38.7% and 23.4% respectively of the nurses as causes of cervical cancer while 95.6% and 75.2% respectively knew correctly that certain foods and bacterial infections were not causes of cervical cancer. Most nurses (60.6%) correctly identified sexual intercourse as a mode of transmission of HPV, while the majority (more than 80.0%) identified kissing body fluids, drinking unsafe water, mother to child transmission and air droplets as non modes of transmission. Multiple sexual partners and history of HPV infection was identified by 47.4% and 43.1% respectively as risks for developing cervical cancer by the respondents. The most common symptom of cervical cancer identified was blood stained vaginal discharge (53.3%), followed by post-coital bleeding (46%), painful coitus (43.1%) and post-menopausal bleeding (38%). Only 19% and 9.5% identified pelvic pain and inter-menstrual bleeding as symptoms. The participating nurses know correctly causes and transmission in 46%, symptoms in 32.1% and adequate risks in only 7.3 %. More than 80% of nurses aged less than 30 years had adequate knowledge on causes of cervical cancer and transmission of HPV compared to only 36.4% and 47.1% for the 30 - 40 and above 40 age groups respectively (p = 0.027). However, the association with cadre, department and work experience was not significant. There was a significant association between the nurses' cadre and knowledge level of symptoms of cervical cancer; 43.3% of the registered nurses had adequate knowledge of symptoms of cervical cancer compared to only 21.4% of enrolled nurses as indicated in table 3. As shown in figure 1, radiotherapy was the most common (70.8%) form of treatment identified by the respondents, followed by surgery (32.1%) and chemotherapy (23.4%) (figure 1). Only 31 (22.6%) of the respondents were aware of the HPV vaccine. Of these, 7 (22.6%) knew that vaccination should be done before sexual debut. Other methods of prevention of HPV infection such as condom use and being faithful to one partner were identified by 48.2% and 46.7% respectively of the nurses. Antibiotics were incorrectly identified by 11.7% of the nurses. Post menopausal screening was the most widely identified time for screening (40.9%) followed by "after sexual debut" (32.1%) while 7.3% incorrectly identified before sexual debut as the timing for screening. Regarding screening interval 55.5% identified either once between the ages of 35 and 45 or once every 3 to 5 years. Nurses were asked for their most recent source of cervical cancer information. Figure 2 show that nursing school was the most common (53.3%) source of cervical cancer information followed by the media (47.4%). Colleagues and self study were sources of information for 18.2% of the respondents each. Only 2.9% and 8% had attended seminars and continuing medical education sessions on cervical cancer. They responded whether they were satisfied with their knowledge regarding cervical cancer or not. The majority, (83.9%) of the respondents were dissatisfied with their knowledge of cervical cancer, only 16.1% were satisfied. Nearly half of the respondents (48.2%) were aware of cervical cancer's importance as compared to other cancers affecting women, 17.5% said it was moderately important, 8.8% mildly important and 25.5% did not know. Most (48.9%) of the respondents were aware of the high risk of developing cervical cancer in case of being HPV infected while 51.1% said there is no risk. Nurses' own cervical cancer screening practices Most (116/137) of the respondents had never had a Pap smear the most common reason (54.7%) was not knowing where to go for the test, followed by seeing no reason for the test (13.1%), being afraid of the procedure (9.5%) and being afraid of bad results (7.3%). Of the 21 respondents who had a Pap smear test 13 (61.9%) had decided to do so on their own while 8 (38.1%) had been advised by a medical personnel Nurses' suggestions for improvements All respondents suggested more education regarding cervical cancer at the work place. The majority (85.4%) of the respondents suggested that more education at their place of work 5.8% suggested more emphasis should be put on the topic in nursing school and as well as education at the place of work and 8.8% suggested the use of mass media in addition to more education at their place of work. Discussion The majority of the nurses in this study had inadequate knowledge of transmission of HPV, causes, risks, symptoms, treatment and prevention of cervical cancer, as has been seen in other studies in Uganda, Turkey and Nigeria18,19,20. Regarding causes, less than 40% correctly identified either HPV infection or genetic predisposition. Only two thirds of the nurses identified sexual intercourse as a mode of transmission of HPV. This result is not surprising in a setting where the most commonly known sexually transmitted infections are HIV-AIDS, chlamydia, gonorrhea and syphilis. As a result less than half of the nurses knew that condom use and being faithful to one partner can prevent HPV infection. A large proportion of the nurses had inadequate knowledge of risks similar to nurses in Uganda18. This is in contrast to findings by Tessaro et al in the United States in a study on nurse practitioners who knew most of the risk factors such as multiple sexual partners, history of HPV infection and sexual intercourse at an early age21. In both studies however only a small proportion of the nurses identified smoking as a risk factor. This can be explained by the fact that smoking is most commonly associated with lung cancer and not with other types of cancers in anti smoking awareness campaigns in the community. This finding can also be explained by the fact that smoking is not a common practice among Tanzanian women. Impaired immunity was identified by 8% of the nurses. This is a poor result given that there is evidence linking cervical cancer to HIV infection more importantly so in a country where HIV prevalence is estimated to be 8%5. The most widely identified symptom was blood stained vaginal discharge by approximately half of the nurses. Post-coital bleeding, painful coitus and post-menopausal bleeding were identified by less than half of the nurses. The inability of these nurses to identify most of the symptoms can be due to shortage of health workers, the nurse patient ratio in Tanzania is approximated to be 1:23,000. As a result, work overload prevents the nurses from spending enough time with individual patients and knowing their symptoms. The majority of nurses knew that cervical cancer could be treated by radiotherapy while only a few were aware of surgery and chemotherapy as treatment options. These results are not surprising since most patients suspected of having cancer are referred to tertiary referral hospitals and the Ocean Road Cancer Institute in the commercial capital city for confirmation of diagnosis and treatment. The nurses therefore do not get to see the management of cervical cancer. Most of the nurses were not aware of the recommended pap smear screening interval, similarly in Uganda in a study done among hospital workers found that less than half of them had adequate knowledge regarding screening interval as found by Mutyaba et al18. Comparatively a larger proportion of Thai nurses could correctly identify the timing as found by Nganwai et al22. These results are a reflection of the fact there is no screening policy set by the ministry of health or locally at the hospital. In most hospitals in the country where Pap smear screening services are available, the test is carried out by doctors. Only a few of the few nurses who were aware of the existence of a vaccine for HPV knew when the vaccine is supposed to be given. In comparison, more than 90% of nurses in a study done among Canadian nurses knew that the vaccine should be given before girls become sexually active23. This could be explained by the fact that the HPV vaccine is still a new concept in most developing countries and is not yet included in the Tanzanian Extended Program on Immunization (EPI). These results could be explained by the level of education of these nurses, most of whom have diplomas and certificates in nursing as compared to those in a study in Thailand by Nganwai et al the majority of whom had bachelor's degrees whereby higher proportions of nurses correctly identified causes, transmission, symptoms, treatment and prevention22. Nursing school was a major source of information for many nurses in this group of nurses whose mean duration of work experience is about 20 years. This reflects the inadequacy of the information given in nursing school and raises concern about the fact that only a small percentage had been to seminars or continuing education sessions. The media has played a big role in increasing cancer awareness in the country in the past few years. The medical women association of Tanzania (MEWATA) has been running breast cancer screening campaigns, which have been in the media but the target audience has been the general public hence the inadequacy in knowledge seen in these nurses many of whom cited the media as their source of information. Given the shortage of health workers at the hospital, it is not surprising that only a few cited self study as their source of information. Despite the presence of a small library at the hospital their duties during working hours do not allow spare time to be utilized in the library reading. The type of literature available at the library might also be a factor as most of the books are old medical text books meant for doctors which might not be easy for the nurses to read. Only a small proportion of the nurses had attended continuing medical education sessions at the hospital or seminars out of the hospital. In comparison, 86% of the nurses in the study by Tessaro et al in the United States had attended a cancer education program in the last 5 years prior to the study (21). This depicts that cervical cancer hasn't been given priority when it comes to arranging the CME sessions or that the nurses have not been able to attend the sessions which are run in the morning when they are preparing the wards and patients for rounds, a lack of interest could be a reason as well. The importance or updating one's knowledge after nursing school is reflected by the significance of the association found between age and knowledge of causes and transmission whereby the younger nurses (< 30 years) were more knowledgeable compared to those aged above 30. Similarly Nganwai et al found a significant association between age and knowledge in Thailand22. This importance is also reflected in a survey by Tessaro et al in which public health nurses' knowledge was assessed in 1993 and again in 1996 where a significant increase in knowledge of risks of developing cervical cancer after receiving education from the breast and cervical cancer control program between the surveys24. These results could be explained by the fact that the nurses below the age of 30 have recently come out of nursing school compared to the older ones, but on the other hand unexpected as the older nurses would have been expected to have more knowledge given the fact that they are more experienced. There was also a significant association between nursing cadre and knowledge of symptoms, registered nurses were more knowledgeable than enrolled nurses This might be due to the differences in the content of nursing curricula between the two cadres, but also surprising due to the fact that they are exposed to the same patients and responsibilities in the wards. The importance of level of education is again supported by findings by Nganwai et al in a group of more qualified nurses22. The lack of a significant association between knowledge levels and department can be explained by the fact that nurses at the hospital rotate between departments at least once every one to two years. In Nigeria however, different health workers, medical doctors and medical literature were the most commonly mentioned sources of information about Pap tests, only a few cited the media in a study by Gharoro et al25. The need for further education regarding cervical education is echoed by the nurses' dissatisfaction with their knowledge. The majority cited education at the place of work in the form of seminars and continuing medical education sessions when asked for suggestions for improvement of their cervical cancer knowledge. They also recommended that emphasis be made in their nursing schools' curricula and the use of print and electronic media as another way of reaching many nurses with information. Most nurses in the study by Nganwai et al also expressed a need for further information about cervical cancer, with the majority calling for printed materials. When asked about their previous screening practices less than one fifth of the nurses had had the test. A similar trend of screening practices was observed by Mutyaba et al among female respondents in a study done in Uganda at a University teaching hospital where only 19% of the female respondents had had a Pap smear test despite the fact that the test was available and free at the hospital18. Similarly, Gharoro et al, reported that a minority of Nigerian female health workers had had a Pap test25. In contrast, a study done in a University teaching hospital by Nganwai et al in Thailand found that 56.4% of the nurses had had a Pap smear test regularly and 86.5% intended to check regularly in the future22. Despite the small proportion of nurses who had had a Pap smear test, almost half of them considered cervical cancer to be of high public health importance. In a study conducted in Nigeria where 93% of respondents including doctors, nurses and hospital maids had never had the test20. This again highlights the absence of a screening policy as well as a lack of awareness of the public health importance of cervical cancer among nurses. In Uganda, Mutyaba et al found that the respondents' reasons for not being screened were not feeling at risk, lack of symptoms, carelessness, fear of vaginal examination, lack of interest, test being unpleasant and not yet being of risky age21. Gharoro et al, show that the majority (89.2%) of those who had never had a Pap test did not feel at risk of developing cervical cancer22. Results from this study as well as those done in Tanzania, Uganda and Nigeria indicate that the utilization of screening services is dependent on an individual's awareness of the importance of cervical cancer screening as well as the ability of the health sector to make these services available and accessible18,25,26. From a health belief model and conceptual framework one can deduce the hypothesis that the nurses' screening practices are influenced by their perception of their own susceptibility to the disease, their regard of the public health importance of the disease, benefit of screening and barriers to screening which are in turn influenced by their knowledge about the disease. As a result and in support of the health belief model, only a small proportion of the nurses had had a Pap smear. The significant association found between knowledge levels and socio-demographic factors (age and nursing cadres were significantly associated with knowledge) shows that not only do demographic characteristics and knowledge influence perceptions and utilization of screening services, they also influence each other. This hypothesis is supported by findings by Smith et al in a study where results showed that female nursing students who had higher mean knowledge scores were more likely to have had a Pap smear test a year prior to the study compared to those who had not27. Nurses in high income countries play a role in cancer prevention and participate in cervical cancer screening by carrying out Pap smear tests21,28,29 due to the lack of logistics and scarcity of gynecologists and pathologists in Tanzania nurses could be used effectively in the prevention of cervical cancer, by being enabled to perform Pap smear tests and using the visual inspection by acetic acid technique which is less costly and does not require high expertise. The data from this study is from one hospital therefore the results cannot be generalized to nurses in other health facilities in the country. These results call for creation of health promotion and disease prevention policies as well as awareness campaigns and screening programs at all levels of the health sector. Integration of screening services into already existing programs, such as family planning and reproductive health services, would be an effective strategy in an already financially and human resource challenged health sector. Conclusion In Tanzania like in most developing countries nurses are the majority of health personnel. It is important that they are well educated regarding cervical cancer, due its public health importance in Tanzania and the world, as they have a large role to play in informing the general public and promoting preventive practices given their influence in society. Acknowledgements We thank the nurses who participated in this study, Mr Kapanda of the School of Physiotherapy of the Kilimanjaro Christian Medical College in Tanzania for his assistance with the Statistical Package for Social Sciences (SPSS).References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11008f1.jpg] [hs11008t3.jpg] [hs11008t2.jpg] [hs11008f2.jpg] [hs11008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}