 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Perceptions of risk and barriers to cervical cancer screening at Moi Teaching and Referral Hospital (MTRH), Eldoret, Kenya *Were E1, Nyaberi Z2, Buziba N3 1Department of Reproductive Health, Moi University Code Number: hs11009 Abstract Background: Affordable screening cervical cancer methods using visual inspection with acetic acid (VIA) and with
Lugol's iodine (VILI) are being developed. Scaling up of screening services requires an understanding of the user perceptions
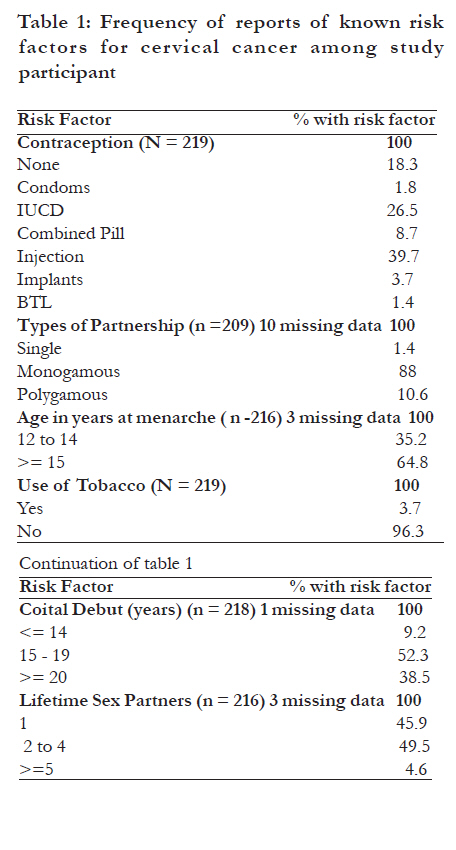
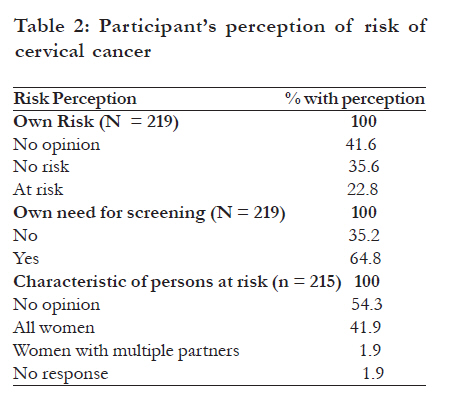
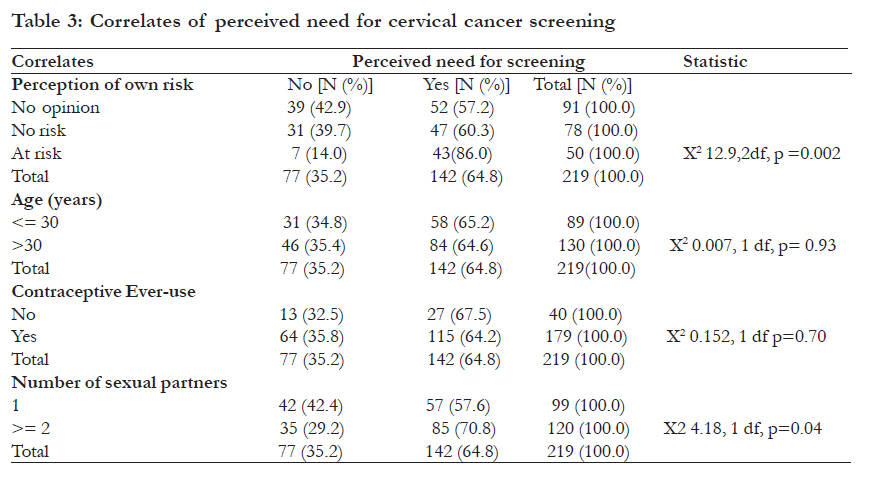
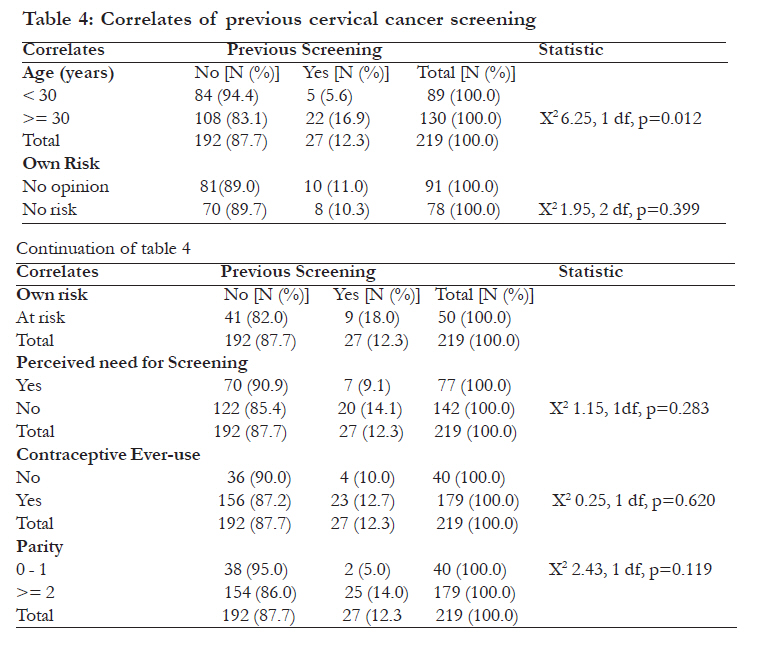
about screening. Key words: Barriers, cervical cancer screening, Kenya Introduction Cancer of the cervix is the commonest tumor affecting women in developing countries including Kenya1,2. Of the cases seen at the MTRH, 90% present with late stage disease and thus can only benefit from radiotherapy or palliative care. The mean duration of illness at presentation is 8.2 months and more than 50% will have visited the primary care facilities for early symptoms of the disease before coming to MTRH3. Majority of the cases do not access the sole radiotherapy facility at the Kenyatta National Hospital (KNH) due to distance, cost and the heavy booking of the facility. At MTRH, only radical surgery can be offered for early cancers, but these account for less than 5%.The options available for late presenting patients are therefore few. Pap smear a cytological screening method to identify pre-cancerous lesions has helped achieve massive reductions in the incidence of invasive disease in the developed countries4,5,6. Pap smear screening requires well trained providers, access to equipment and supplies, cytology laboratory, arrangements for communicating results to screened women and a facility for confirming diagnosis and treatment of the precursor lesions and referring advanced cases. Although its cost effectiveness can be enhanced through use of non-physician providers it is currently not widely available due to infrastructural constraints. Newer low cost techniques such as visual inspection with acetic acid (VIA) and visual inspection with Lugol's iodine (VILI) have been developed and are being evaluated. Emerging evidence suggests that these new approaches have comparable test characteristics to the cytological methods7,8. Compared to pap smears, VIA has a bigger problem of false positives which can lead to over-treatment7,8,9. However, VIA is cheap, easy to learn, does not require laboratory infrastructure and allows women to get the results in one visit except where VIA positive lesions require further evaluation. See and treat strategies have also been developed to increase access to treatment10. While a lot is thus being done to develop new screening technologies, there is need to assess the health seeking behavior of women meant to benefit from such new approaches. Determinants of uptake of cervical cancer screening services include age, education, contraception use and being married11,12. Reasons for not screening include perception of not being at risk and fear that abnormal test results mean existing cancer13,14,15. Women with low educational achievement, low awareness of the risk factors for cervical cancer, and who do not have support from their husbands may also have poor uptake of screening services14,16,17. Identification of characteristics of women, their perceptions of own risk and barriers to accessing existing screening services can provide important information for shaping screening services as developing countries prepare to adopt emerging and more affordable technologies such as visual inspection approaches. Our study objective was to document the cervical cancer risk characteristics, previous screening behavior, the perception of own risk and barriers to accessing screening in the past for non-pregnant women accepting to undergo cervical cancer screening by visual inspection while attending the MCH-FP clinic of MTRH. MethodsSetting and Target Population: This cross-sectional study was carried out between May 2005 and January 2006, at Moi Teaching and Referral Hospital (MTRH). MTRH is Kenya's second national teaching and referral hospital and is located in the town of Eldoret, in the North Rift Area of Western Kenya. The MCH-FP clinic is a general outpatient reproductive health and well baby facility serving about 300 women monthly. Women accessing this clinic are from the Eldoret Municipality and immediate environs, an estimated population of about 400000 persons of which about 90000 are women in the reproductive age. During the study period, a total of 2803 women were seen at the clinic for either family planning or well baby services and formed the population from which our study sample was drawn. The Study Procedure A consecutive sample of women accessing family planning services or presenting their children at the well baby clinic were invited to screen for cancer of the cervix using visual inspection approaches. The main inclusion criteria were being 18 years and above, non-pregnant and consenting to be included in the survey. Women who were visiting the MCH-FP clinic for antenatal care were excluded. Women approached to undergo the screening procedure were first interviewed by a non-care provider research assistant using a pre-designed questionnaire to document their knowledge, attitudes and previous use of cervical cancer screening. The visual cervical cancer screening services were being offered free on a trial basis at the hospital. The participants were informed of the various available approaches including Pap smear, VIA and VILI and informed that the latter two techniques while cheaper than Pap smears were still being evaluated. The purpose of this survey was to explore the concerns of women about Pap smear cervical cancer screening, generally, but, more specifically, to document the correlates of reported need for cervical cancer screening and previous screening behavior. Among the factors explored was how the respondents rated their own risk of cervical cancer and, consequently, their need for screening. Socio-demographic data and information related to known risk factors for the development of cervical cancer were collected. The key outcome variables were previous screening behavior, perception of own risk, need for screening and barriers to screening. The study was approved by the Ethics Committee of MTRH and permission to carry out the study granted by the Director of MTRH. Data Analysis and Presentation Data was analyzed using Statistical Package for Social Sciences (SPSS) version 15 software. Descriptive statistics were derived for socio-demographic characteristics, known risk factors and perceptions of risk related to developing cervical cancer. For open ended questions, the responses were grouped into broad categories and then frequencies of the responses calculated. Correlates of perceived need for screening and previous screening were determined by cross-tabulating relevant determinant variables with these outcome variables. Chi-square statistic was calculated for the specified cross-tabulations, where appropriate, with significance declared at a p-value of <0.05. ResultsDemographic characteristics We invited 308 women of whom 219 accepted to participate in the questionnaire survey and to be screened using visual inspection methods of VIA and VILI. This represented a response rate of 71.1%.The participants were evenly distributed around age 30 years with a mean of 31.3 years and a standard deviation of 6.8years. Primigravidas and women with no past pregnancy accounted for 44.5% while the rest (55.5%) had had at least two past pregnancies. The mean parity was 3.1 with a standard deviation of 1.9. Occurrence of Known Risk Factors The frequencies of known risk factors for cervical cancer in the study sample were estimated based on participants' self report. The traditional risk factors for development of cervical cancer were observed in a substantial proportion of the study participants. Of note is the large proportion (over 54%) of study participants who on self report had multiple sex partners. Tobacco use was uncommon, reported by less than 4%. Sexual debut earlier than 20 years was rampant mentioned by nearly 62% of participants. The high rate of contraceptive use was not surprising since this was a selected population derived from the MCH-FP clinic (Table 1). Perceptions of Risk and need for Screening About 35% of participants felt that they were at no risk of developing cervical cancer and felt no need for screening for the condition. Even though only approximately 23% of all respondents felt that they were at risk of the condition, about 65% of all participants, none the less, felt they needed to be screened for the disease. A substantial 42% of the participants had no opinion on their own risk, and this was further reflected in the 54% of all participants who did not have any opinion on who is at risk of cervical cancer (Table 2). Correlates of Perceived Need for Screening Of women perceiving themselves to be at risk of cancer of the cervix, 86% (43 out of 50) expressed the need for cervical cancer screening compared to about 60% (47 out of 86) of those perceiving themselves to be at no risk and 57% (52 out of 91) of those who had no opinion on own risk. These differences were statistically significant (p=0.002). Approximately 71% (85 out of 120) of women reporting more than one lifetime partners compared to 58% (57 out of 99) of those reporting one lifetime partners expressed a need for screening. The association between number of life time sex partners and perceived need for screening was also statistically significant (p=0.041). When controlled for the number of lifetime sex partners, the relationship between the perception of being at risk for developing cervical cancer and the need for cervical cancer screening disappeared for those reporting one lifetime sex partner (X2 4.807, 2 df, p=0.090) but persisted for those reporting two or more lifetime sex partners(X2 10.771 2df,p=0.005). There was no significant relationship between age or reported contraceptive ever-use and a perception of need for cervical cancer screening (p=0.933) and (p=0.697), respectively as shown in table 3. Previous Cervical Cancer Screening and Barriers to Previous screening Only 12.3% of participants had ever had cervical cancer screening at the time of the survey. While 39% reported that there were no barriers to cervical cancer screening, fear of abnormal screening results and lack of finances appear to be the most commonly reported barriers to screening mentioned by 22.1% and 11.4% of respondents respectively. Lack of awareness about the service was reported by 4.1% of the participants while 5.5% of the respondents mentioned fear of genital exam as a barrier to screening. A substantial 16.1% of participants expressed no opinion about the barriers to cervical screening. Correlates of Previous Screening Among participants of above 30 years, 16.9% (22 out of 130) had had previous screening compared to 5.6% (5 out of 59) among participants of age 30 years or below. This difference was statistically significant (p=0.012). There was no statistically significant relationship between reported previous screening and perceived need for screening (p=0.283), between previous screening and perceived own risk (p=0.399), previous screening and contraceptive ever-use (p=0.620) and between previous screening and parity (p=0.119) as indicated in table 4. Discussion We found a low level of self-reported previous cervical cancer screening even among this very highly selected population, consisting women already seeking reproductive health services. Only 12.3% of the participants reported having screened at least once before this contact. Previous testing was significantly more common among women of over 30 years, probably reflecting a cohort effect of exposure to health services. Previous exposure to reproductive health services has been reported to be associated with higher awareness of screening for cervical cancer in an Indian population18. It is, however, likely that the level of cervical cancer screening in the general population, from which our study sample was drawn, will be much lower than that found in this selected group of participants. In Thailand, an opportunistic cervical cancer screening strategy based on Pap smear, similar to what is currently available in Kenya, recorded an estimated population coverage of only 5%19. In Kenyatta National Hospital, Nairobi, 22% of respondents, in a survey similar to ours, reported past Pap smear screening20. This was a more urban population compared to our participants. The rate of past screening in this urban population was, nevertheless, still quite low. Even where screening facilities exist, there are individual characteristics that determine whether a woman actually does access the services. Women who accept to screen tend to be younger (aged 30-39), married, had mostly been pregnant, better educated and had ever used contraception18,20,21,22.Our study participants had similar characteristics but we did not collect data on educational achievement nor did we assess their socioeconomic status. Knowledge of risk factors for cervical cancer development has also been observed to be associated with better uptake of screening services23,24. We found no significant relationship between previous screening and parity or contraceptive ever-use. However, as noted earlier women of age greater than 30 years were significantly more likely to have had cervical screening before the survey. Women's perceptions of the screening services, awareness of the risk factors for the disease, having financial resources and support from the spouse are other significant factors in determining use of available facilities15. Our participants reported key barriers to access as including fear of positive screening (or abnormal Pap smear) results, lack of awareness about the screening services and lack of finances to buy the services. Lack of awareness and low priority accorded women's health have been cited as some of the factors contributing to the observed reluctance of women to access screening services25. The correct perception of individual or own risk of development of cervical cancer is an important potential cue to action on the road to cervical cancer screening. Perception of not being at risk is documented to be associated with low uptake of screening13. We found a highly significant relationship between a perception of own risk of developing cervical cancer and an expressed need for cervical cancer screening. Lastly, it is critical that health education programs explain clearly to women the difference between precancerous lesions and invasive cervical cancer and the treatment options available for each of these clinical entities26. This would reduce the frequency of the erroneous fear of abnormal cervical screening findings which was mentioned as a significant barrier to cervical cancer screening in our study. The interpretation of these study findings is limited in several ways. Firstly, the findings are only referable to women who accepted to be interviewed and eventually to undergo screening using the visual inspection approaches. It is likely that women refusing to participate in the screening were significantly different from those interviewed hence curtailing the generalizability of the study. Secondly, the study population was also selected for the women who were already accessing the MCH-FP services and therefore not representative of women in the reproductive age group from the catchment of MTRH. And, thirdly, the key parameters of attitude, knowledge and reports of previous screening were based on self report, specifically, to interviewer administered question. Self report and interviewer administered questionnaire for health seeking behavior are known to be susceptible to social desirability bias27. Nevertheless, the study still provides some insights into the barriers to cervical cancer screening at MTRH. Acknowledgement This work received support from African Institute of Capacity Development (AICAD) under Contract Number: AICAD/04/A/011. We are grateful to the Director of MTRH for permitting this project to be carried out in the hospital and to the participants for their role in the project. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11009t1.jpg] [hs11009t2.jpg] [hs11009t3.jpg] [hs11009t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}