 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Parity and maternal education are associated with low birth weight in Malawi Muula AS 1, *Siziya S 2,Rudatsikira E3,4 1Division of Community Health, Department of Public Health, College of Medicine, University of Malawi,
Blantyre, Malawi Code Number: hs11010 Abstract Background: The consequences of low birth weight (LBW) include death and long-term health sequelae. Limited
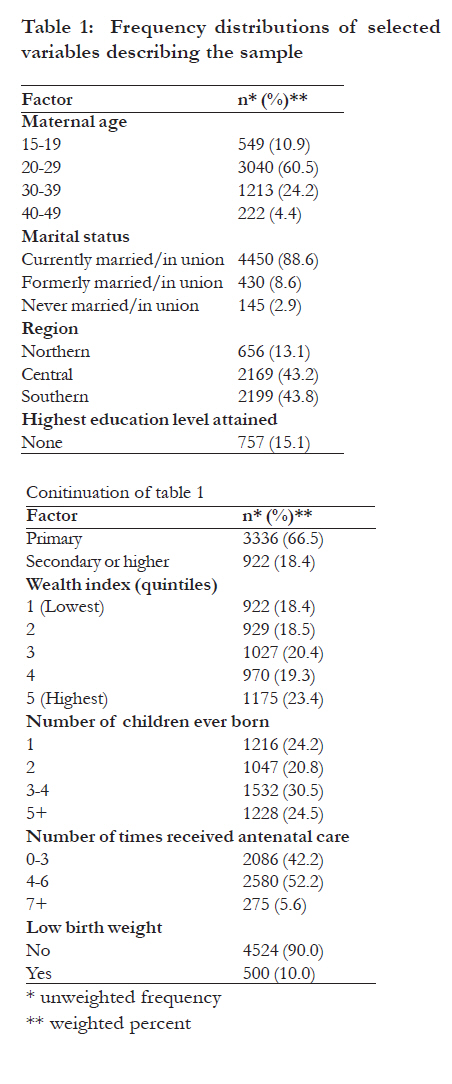
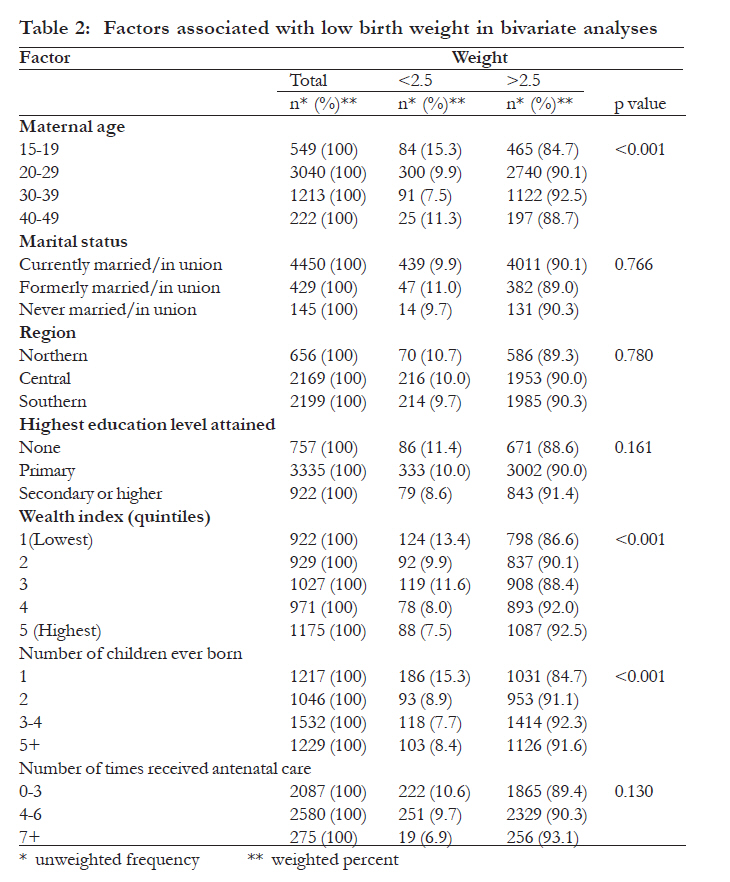
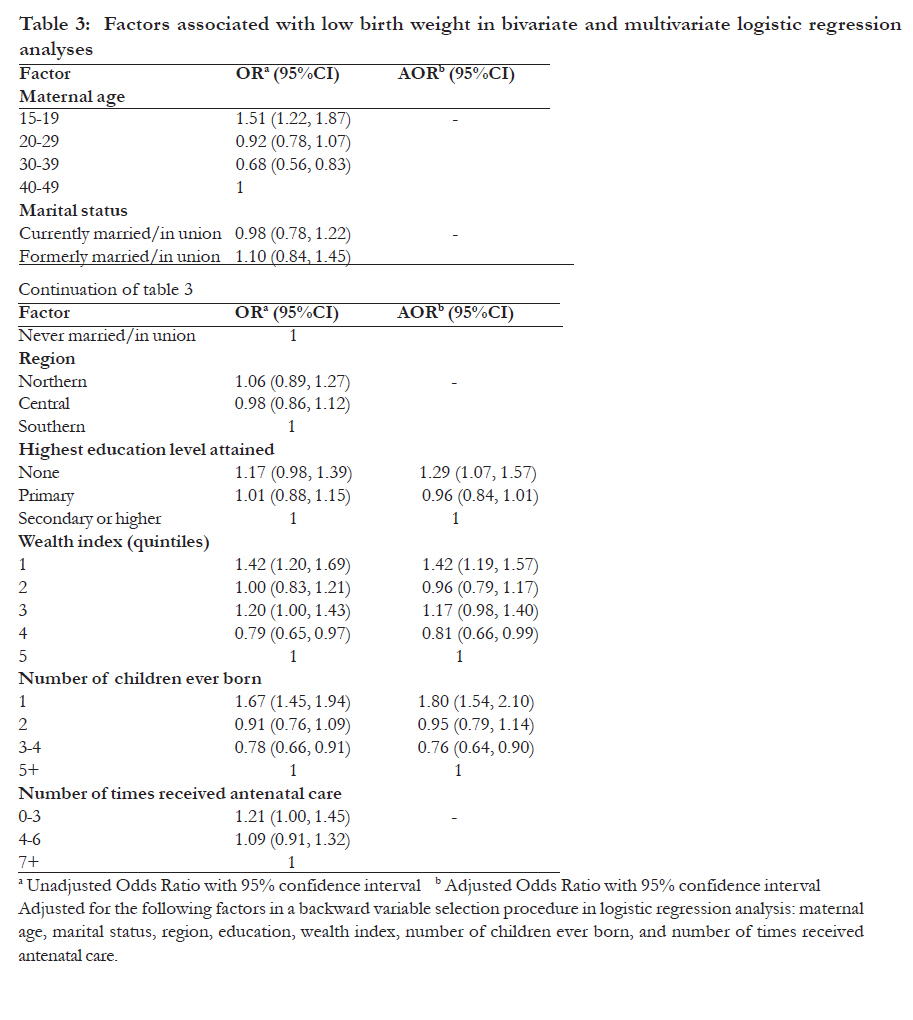
attention has been made towards the study of socio-demographic factors that may be associated with LBW in Malawi. Key words: Parity, maternal education, low birth weight Introduction Low birth weight (LBW) is an important birth outcome because it is associated with several adverse effects, including diseases which increase neonatal mortality and have long term consequences among the survivors1. For instance, foetal growth restriction and postnatal weight gain has been linked to adult coronary heart disease and the related disorders: stroke, hypertension and type 2 diabetes2,3. Babies are likely to be born with lower weight in a developing country like Malawi than in an industrialized country with rates averaging 14.3% in Africa and 6.4% in Europe4. Previous studies in Malawi have reported associations between LBW and selected variables such as maternal malaria and/or HIV infection5,6. While there has been interest in the biological correlates (HIV, malaria) for LBW in Malawi, there remains paucity of data on socio-demographic factors that may be associated with LBW in the country. As may be expected, a biomedical approach to LBW is likely to arouse interest in biomedical solutions such as antiretroviral prophylaxis against HIV infection, intermittent presumptive treatment (IPT) and insecticide treated bed nets against malaria. These are certainly important considerations and have understandably been scaled up in the country but are unlikely an end of themselves to substantially reduce LBW. This may be so, if other equally, if not more important determinants of LBW receive limited attention. We, therefore, set out to explore a list of social and demographic factors (age, wealth, education, parity, residence in a region of the country) that may be associated with having delivered a LBW baby at the most recent delivery among Malawians women. We used data from the Malawi Multiple Indicator Cluster Survey (MICS) conducted in 2006 to explore these associations. MethodsStudy design and the MICS Questionnaire A secondary analysis was conducted using the 2006 Malawi MICS data, which we obtained from ORC Macro, Calverton, Maryland, United States of America. The data were collected by the National Statistical Office. The MICS is a household survey initiative developed by UNICEF to assist countries in filling data gaps for monitoring the socio-economic situation of children and women 7,8. Its design enables the estimation of nationally representative estimates and allows cross-national comparisons of indicators due to its standard methodology. Sampling and data collection The 2006 Malawi MICS used a two-stage sampling methodology to select a total of 1,200 households per district. At the first stage of sampling, 40 census enumeration areas (clusters) were selected in each district with probability of being selected proportional to population size. A household list was drawn from each cluster and a systematic sample of 30 households in each cluster was eventually identified. All children under the age of 5 years in selected households were enumerated. The child's mother or any other caretaker of the child (in the absence of the mother) was interviewed. Data was not available on the proportions of the respondents who were mothers or other caretakers. A total of 31,200 households (26 districts multiplied by 1,200 households) were selected in 1,040 clusters (26 districts multiplied by 40 clusters) under MICS. All the selected 1,040 clusters were covered during the fieldwork period. MICS is thus one of the largest household sample surveys undertaken in Malawi. Response rates of the Malawi Cluster Indicator Survey All 31,200 households selected for the sample were occupied. This is because the house listing operation and the canvassing of households took place at the same time. Of these households, 30,553 were successfully interviewed resulting in a household response rate of 97.9%. In the selected households, mothers or other caretakers of 22,994 of 23,238 eligible children were interviewed, yielding a response rate of 98.9%. Variables of interest Associations between LBW, defined as birth weight of <2500 grams, and the following factors were assessed: age of woman, marital status, region of the country, highest level of education level attained, wealth index quintile, children ever born to woman, and number of times the mother received attended antenatal clinic. Wealth variable Wealth was defined based on household assets (such as radio, bicycle, car, television, type of roofing, and floor) reported by the survey participant. Each asset was assigned a weighting value, using principal component analysis as described by the World Bank and ORC Macro. A household was assigned a standardized score for each owned asset. For each household, these scores were summed and households ranked into five wealth quintiles 9. Regional descriptions of the country Malawi is divided into three administrative regions: northern, central and southern. These regions differ in many regards such as, majority ethnic group, wealth and education status. In the North, the majority ethnic group is Tumbuka that has a patrilineal inheritance system and virilocal residence (a married woman leaves her parental home to live with the husband's family). The Malawi Demographic and Health Survey 2004 estimated 16.3% adult women and 10.1% adult men had no formal education, while 12.2% women and 18.8% men had secondary education or higher 10. The central region is largely dominated by the Chewa tribe, while the south is largely occupied by the Yao, Lomwe and Nyanja. Both the central and the southern regions are uxirolocal (a married man leaves his family to live with the wife's family), and inheritance is matrilineal. There are certainly exceptions to these general rules where in some cases, patrilineal and virolocal patterns are followed. Education attainment in the central and southern regions is similar and lower than that in the northern region. Statistical analysis Data were analyzed using SPSS version 14.0 (SPSS, Chicago, Illinois, United States of America). Frequencies were calculated for the LBW variable and explanatory variables. A weighted logistic regression analysis was conducted to estimate the magnitudes of associations between selected explanatory variables and the main outcome. All the variables considered in bivariate logistic regression analyses were entered into a multivariate model. A Backward variable selection procedure in logistic regression was used. We report unadjusted odds ratios (OR) and adjusted odds ratios (AOR) together with their 95% confidence intervals (CI). ResultsSocio-demographic characteristics of the survey participants A total of 26,259 females in the age group 15-49 years participated in the survey, and of these, 5024 (90.9%) had children who were weighed at birth out of 5527 women who were eligible to enter our study. Table 1 shows the distributions of selected variables describing the sample. Most (60.5%) of the participants were in the 20-29 years age group. Meanwhile, 15.1% of the participants were in the 15-19 years age group. Participants who were currently married/in union represented 88.6% of the sample. About two thirds (66.5%) of the participants had attained some primary level of education, and 15.1% had no formal education. Overall, 30.5% of the mothers had ever given birth to 3 or 4 children. While 5.6% of the mothers had received antenatal care (ANC) more than 6 times, 42.2% had received ANC less than 4 times. The prevalence of LBW was 10.0% (95%CI 9.2, 10.8). Variables associated with low birth weight Table 2 shows results from bivariate analyses. Only maternal age, wealth index, and number of children ever born were significantly associated with LBW. However, in multivariate analysis (results shown in table 3), the significant factors were: education, wealth index, and number of children ever born. Compared to mothers who had attained at least secondary level of education, mothers who had no formal education were 29% (Adjusted odds ratio (AOR) = 1.29 [95% confidence interval (CI) 1.07, 1.57]) more likely to bear children who had LBW. Compared to mothers who were in the 5th wealth quintile (the non-poor), mothers who were in the 1st and 4th quintiles were 42% (AOR=1.42 [95%CI 1.19, 1.71]) more likely, and 19% (AOR=0.81 [95%CI 0.66, 0.99)] less likely, respectively, to bear children who had LBW. Mothers who had ever given birth to 1 child were 80% (AOR=1.80 [95%CI 1.54, 2.10]) more likely to bear children who had LBW compared to mothers who had ever given birth to 5 or more children. Meanwhile, mothers who had 3-4 children were 24% (AOR=0.76 [95%CI 0.64, 0.90]) less likely to bear children who had LBW compared to those who had ever given birth to 5 or more children. Discussion In a nationally representative sample of Malawian women of age 15-49 years who had delivered a child in the past five years prior to the survey, we found in multivariate analysis that women with no formal education were more likely to have delivered a LBW baby compared to those with at least primary education. This difference persisted even after controlling for maternal age, marital status, region, education, wealth index, number of children ever born, and number of times received antenatal care. Both lower parity and lower wealth index were independently associated with a higher likelihood of having delivered a LBW baby. That having no formal education was associated with increased likelihood of having delivered a LBW baby was not perhaps surprising as different measures of socioeconomic disadvantage are associated with adverse delivery outcomes such as LBW 11-13. The mechanisms associated with LBW among the less educated may include poor diet as a result of low income and low dietary literacy. Olsen et al 14 have reported that milk consumption which may be a feature of high socio-economic position during pregnancy was associated with increased neonatal size. Limited education may also result in limited access to prenatal care, especially in settings where clients or their health insurance are expected to pay for service. This is not expected to be an issue as prenatal care attendance was controlled for in our analysis. We however hypothesized that educated women are more likely to adhere to health messages either because of their social circumstances or the cognitive priming that education affords 15-17. Non-poor women were less likely to deliver LBW babies than poor women, although this was not statistically significant. Wealth has been consistently reported to be associated with better pregnancy outcomes in diverse settings 18-20. While it is generally understood that improved wealth and/or education are desirable, we can not say the same to the number of children that the woman has ever had. Why were women who had previously given birth less likely to deliver LBW babies when age, wealth, education and other variables are controlled for? A possible explanation is that higher parity mothers have experiences to draw on to improve their pregnancy outcome. This however needs to be verified in a longitudinal study. Limitations of the study This study had several limitations. Firstly, data were not collected on a host of other factors that may be associated with LBW deliveries. These include twin delivery, congenital malformations, malaria, HIV and other infections, gestational weight gain, smoking, pre-pregnancy weight and prematurity 21-23. Furthermore data on the explanatory variables (e.g. education, parity) were self-reported. To the extent that survey participants misreported, our results may be biased. We have no specific information to suggest that survey participants may have mis-reported or not on any of the variables. There were some missing data, and these were declared missing in the analysis. We however conducted complete case analysis and did not attempt imputations of missing data. However less than 1% of the data for a given factor that was considered in the analysis was missing, and may not have significantly biased our findings. The ultimate goal of health research is to improve public health. We therefore need to examine the mechanisms that could explain the increased odds of LBW among women with no education, lower weight and fewer children ever given birth to. Due to the cross sectional nature of the data collection exercise of the MICS, no temporal linkages can be made between LBW and any of the explanatory variables. Conclusion The higher odds of delivering a LBW baby among women with no education, and lower wealth status may suggest that there is need to tailor pre-natal care based interventions on social status. This may involve creating education level-specific health messages. Acknowledgements We thank UNICEF, New York, for making these data available for our analysis. Grateful thanks to the women who participated in the survey. The UNICEF however, did not influence the analysis and had no role in the decision to submit manuscript for publication. Dr Adamson Muula is supported by the University of Malawi, College of Medicine funding for staff development of junior faculty. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11010t2.jpg] [hs11010t1.jpg] [hs11010t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}