 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
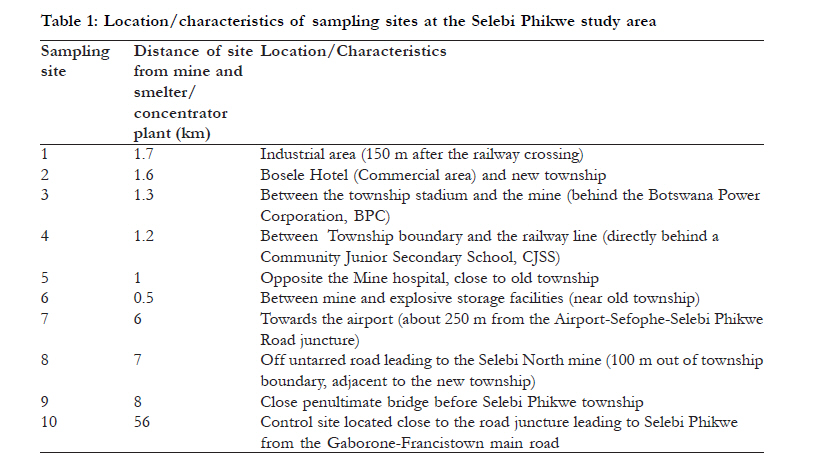
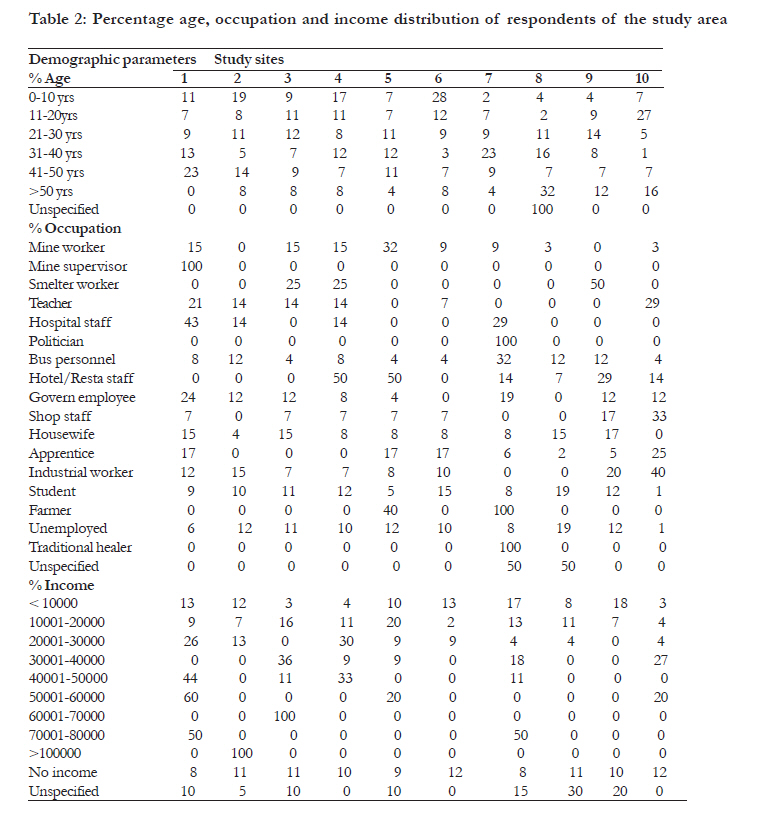
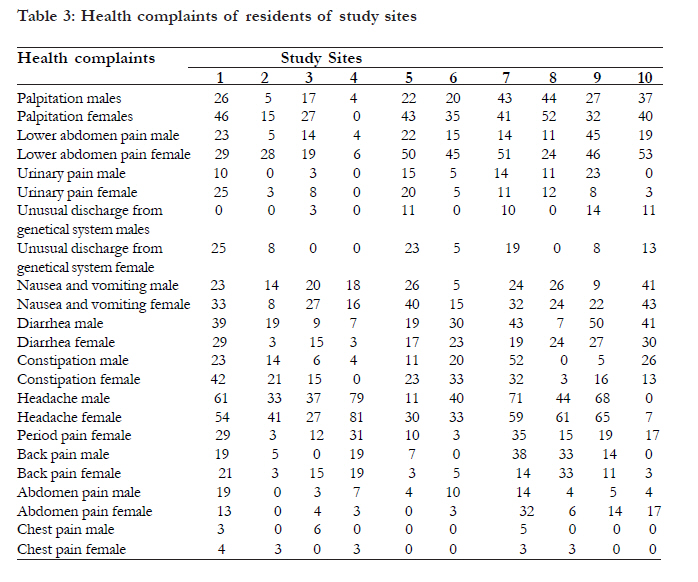
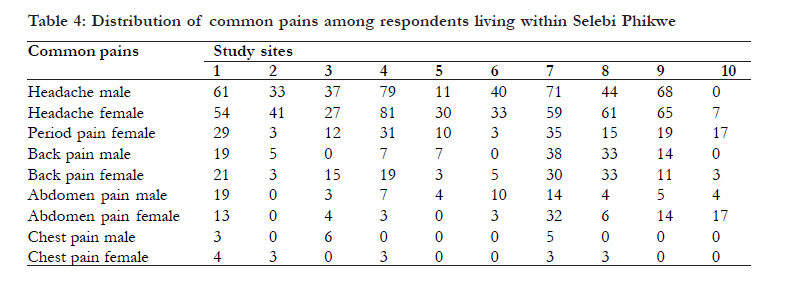
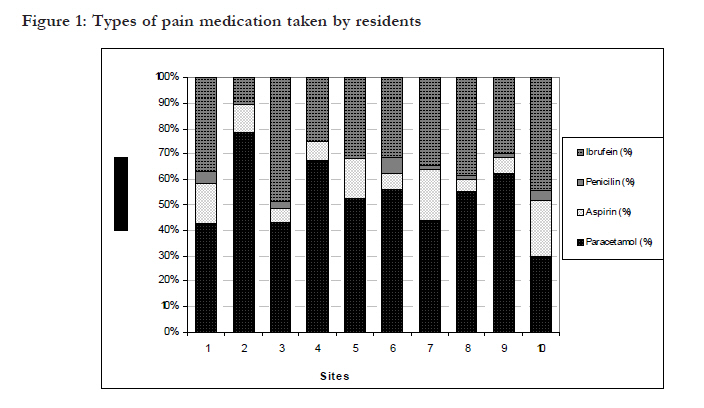
Health status within the precincts of a nickel-copper mining and smelting environment *Ekosse G-IE Directorate of Research Development, Walter Sisulu University, Eastern Cape, South Africa Code Number: hs11014 Abstract Background: Mining and smelting activities affect the biophysical environment and human health. Keywords: fumes of sulphur dioxide, health, pain, smelter/concentrator plant Introduction Exploitation of Ni-Cu ore bodies at Selebi Phikwe, Botswana has been active for more than thirty years. Underground mines provide Ni-Cu ore which is fed into the concentrator/smelter for its processing to Ni-Cu matte1,2. Due to financial and technical constraints, inhabitants displaced as a result of the Ni-Cu exploitation were not compensated. This resulted in the simultaneous growth of mining facilities as well as townships. The local population traded in livestock and dairy products, traditional alcoholic beverages, and Belina imbrassia (phane worms); and 5000 workers were engaged in mining activities. Consequently, squatter camps sprang up as well as urban settings3,4. Large scale and small scale industries, commercial businesses and agricultural farms developed in the area. Women and children continued to be gainfully engaged in harvesting and selling of Belina imbrassia caterpillar which is widely eaten in southern Africa. Through a separate study, it was demonstrated that mining and smelting activities at Selebi Phikwe were having a direct influence on the biophysical environment, contaminating the soils, Colophospermum mopane, Belina imbrassia and the atmosphere4,5. Atmospheric pollution due to release of particulate air matter (PAM)6 and sulphur-rich gases was eminent at Selebi Phikwe. It was hence suspected that the inhabitants of the area probably inhale polluted air. Its residents generally complain of frequent coughing, influenza/common colds, constant headaches, chest pains, cardio-pulmonary complications, tuberculosis, bronchitis, pneumonia, general body weaknesses and poor sex performances 1,7,8. Considering the afore-mentioned setting, it was evident that research be directed at human health concerns for residents within the precinct of the mining environment. This study thus focused on elucidating on the health status of residents within the precincts of the mine and the concentrator/smelting plant as Selebi Phikwe, Botswana. Methods Selebi Phikwe (27o 47'E - 27o 53'E, 22o 55'S - 22o 00'S), is located in the north-eastern part of Botswana. The study area is approximately 250 km2 with 50 000 inhabitants; and a population projection of 78 000 by 2021 based on current growth rate of 2.4% 9. Rapid population expansion from <5 000 in 1971 to its present population size characterised by 52.5 % male and 47.5 % female, has led to exertion of pressure on existing social and economic infrastructures10. Most of the males that comprise the labour force are engaged in mining of Ni-Cu. The study area was divided into ten sites based on a previous study by Ekosse et al. 5,6, as indicated in Table 1. Site ten was the control site located 56 km from the study area. Primary data concerning the general health status of inhabitants in the Selebi Phikwe area and at the control site was obtained by administering questionnaires and structured interviews conducted with randomly selected individuals. The questionnaire consisted of six subsections covering demographical and biographical data, family history, general complaints about personal health, past medical history, past and present treatment/medication, general profile, social and personal history. Individuals selected to take part in the study were those who lived in Selebi Phikwe. An approach whereby individuals were chosen based on where they lived making sure that there was equal distribution of questionnaires to all the ten sites was used. Equal distribution of questionnaires per site for individuals was opted for because the subpopulation per site was almost the same; an approach suggested by Czaja and Blair11. Field data obtained through the administration of questionnaires were coded, processed and analysed both qualitatively and quantitatively. The Statistical Package for Social Sciences (SPSS) Version 11.012, and Microsoft Excel (MS Excel)13, were utilised to analyse data on the health status of individuals at Selebi-Phikwe Cu-Ni mine area in Botswana. Obtained data was coded and the data codes were entered directly in the Data Editor using the software packages. Frequency and cross tabulation procedures in SPSS were used in analysing the coded data. The Frequencies procedure offered descriptive statistics and graphical displays that were useful for describing variables. The cross tabulation tables generated were used to display the relationships among location site and gender (type) as the control variables with all other variables. To get a graphic representation of the output, these cross tabulation tables were imported into Microsoft Excel for the production of percentage distribution charts. Results The age, occupation, and income status of respondents are presented in Table 2. It could be deducted from the table that > 25 % of the respondents from site 10 were > 50 years old, whereas there was none from site one > 50 years old. Furthermore, 28 % of the respondents from site seven were 31 - 40 years old, and 60 % from site eight were not sure of their real ages albeit they were adults. Mine workers lived in all the sites except sites two and nine. Furthermore, 34 % of the respondents from site one and 18 % from site five were mine supervisors. Fourteen percent of respondents from site four, 20 % from site three and 24 % from site nine were smelter workers. In site one, 40 % of the respondents were industrial class workers. In sites four and five, 20 % of the respondents from each of the sites were hotel/restaurant workers, and 42% from site eight were not specific as to the type of employment engaged in. In site 10, 24 % of respondents were farmers, 20 % apprentices, 18 % teachers and 5 % housewives. Annual earnings of most of the workers were < BWP10 000.00. All sites had workers of low income earnings (< BWP10 000.00) with the highest percentage being 33 % from site six. Fifty percent of the workers from site eight did not specify income. Whereas 55 % of the workers of site three earned BWP60 000.00 - BWP70 000.00 annually, 65 % of those from site two had an annual income of > BWP100 000.00. Currency conversion at the time of fieldwork was BWP6.12 to US$1.00. Table 3 gives details of respondents' complaints consisting of palpitations, pain in the lower abdomen, shortness of breath, chest pains, unusual spitting, coughing regularly, and frequent headaches. They indicated that they experienced unusual loss of body weight, often had constipation, diarrhoea, and nausea and vomiting, and also suffered from pain when urinating as well as having unusual discharge. Data obtained from respondents indicated that residents suffered from frequent headaches, often had influenza/common colds, were regularly coughing, and experienced chest pains frequently than other complaints (Table 3). A high percentage of both males and females suffered from headaches frequently, of which higher percentages occurred in sites three, four and eight. However, there were slightly more females who suffered from headaches than males. High percentages of respondents who complained of having frequent influenza/common colds were for females in sites three, four and eight, and males in site eight. In site four, there were more males and females who complained of experiencing regular chest pains than in any of the other nine sites. Headaches, chest pains and influenza/common colds stand distinctly in all the studies as the most frequent health complaints. Responses of Selebi Phikwe inhabitants who suffered from headache, period pain, back pain, abdomen pain and chest pain are summarised in Table 4. Percentage values for the cited aches and pains in the control site were lower than those obtained from the other nine sites. Above 50 % of the respondents for both males and females from sites one, four, seven, eight and nine frequently suffered from constant headaches (Table 4) Percentage values of both male and female respondents who suffered from other pains were < 40 % for each type of pain. Most of the individuals suffering from aches and pains took medicines except those experiencing chest pains. In terms of medication for headache, period pain, back pain, and abdomen pain; paracetamol, aspirin (acetylsalicylic acid), penicillin and ibuprofen were the most commonly administered drugs (Figure 1). The respondents indicated that they could buy penicillin without prescription and took it for pains. From Figure 1, 88 % of respondents in site four suffering from pains took paracetamol; 66 % each from sites seven and nine; 60 % from site eight and 50 % from site one all took paracetamol. Fifty five percent of the respondents from site seven took ibuprofen. Imposing parameters such as fumes from the mine and the smelter/concentrator plant, dust generated by mining activities, vibrations due to rock blasts, and noise resulting from blasts and constant movement of heavy equipment were considered by the residents to be disturbing environmental factors affecting their health and well being. Quite distinctly clear is the fact that respondents have cited fumes of SO2 to be the main aspect of mining and smelting activities, which disturb them the most. The lowest percentage value for disturbances by fumes reported by respondents was in site five (60 %), and the highest was in site two (91 %). Disturbances by vibrations from the rock blasts were highest in site 1 and lowest in site nine. The noise emanating from blasts and the movement of heavy equipment was highest in site one. Respondents from site nine indicated that more dust was generated during mining activities. This was not the case in the control site where percentage values for fumes, dust, vibrations and noise were very low. Health complaints of residents could therefore be linked to aspects of environmental pollution due to mining activities. These observations have been reported in other mining environments such as in Zambia14 and Australia15 where Ni and Cu are mined. Meteorological conditions such as temperature, wind speed and wind direction aid in the transportation and deposition of PAM. Daily average temperatures at Selebi Phikwe between January and July decreased from a maximum of 28 oC in February to 14 oC in July. Wind speed increased from 2 m/s in January to 6 m/s in July. At the time of study, the wind direction was from north westerly to east south easterly or south easterly direction. By implication, the health of respondents in sites lying within the wind direction was more affected. Clearly, the weather parameters played a contributory role in the spreading and high prevalence of frequent coughing, rampant chest pains, constant headaches and regular influenza/common cold suffered by the inhabitants of Selebi Phikwe. A study conducted by Urashima et al.16 and Kunst et al.17 confirmed that increase in wind speed and decrease in temperature could result in increase in the number of influenza infections; a meteorological condition that could be applicable to the Selebi Phikwe scenario. Prevailing winds blowing through the Ni-Cu concentration/smelter plant in the north-easterly direction means SO2 pollution directly affected certain areas of the town including the industrial site. With such level of emission, there was the potential to increase the incidence of respiratory problems which included breathing, respiratory illness, alterations in pulmonary defences, and aggravation of existing cardiovascular disease. Conclusion This study focussed on elucidating on the health status of residents of the study area based on the influence of mining activities. It was conducted through the administration of questionnaires and structured interviews, from which the results were analysed using SPSS and MS Excel. The analysed data presented included demographic information, complaints of personal health, and environmental concerns which were considered to be directly related to mining activities within the study area. Findings of the study revealed that health hazards increased with closeness to the mine and the concentrator/smelter plant. In order to reduce the health hazards due to mining activities at Selebi Phikwe, the residents should avoid staying outdoors as much as possible where the risk of exposure to contaminated air is quite high; and for those who are frail in health, they should consider relocation to other township areas away from the sulphur-rich gases and fumes. Residents should have regular check-ups of their health status. Government and related agencies, and the Mine Authorities should work as a team in monitoring pollution activities at Selebi Phikwe. In collaboration with Health Service Providers, active Health Education Programs which focus on sanitation, and health and wellness of the inhabitants of the study area should be regularly conducted. Such radical move will aid in abating the frequency of occurrences of the sicknesses and diseases in the study area. Expansion of Selebi Phikwe should be regulated in such a way that the growing population is least exposed to the sulphur-rich gases and fumes. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11014t3.jpg] [hs11014t2.jpg] [hs11014t1.jpg] [hs11014f1.jpg] [hs11014t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}