 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 158 - 162 Seroprevalence and determinants of human herpes virus 8 infection in adult Nigerians with and without HIV-1 infection *Ogoina D1, Onyemelukwe G1, Musa BO1, Babadoko A2 1Immunology unit, Department of Medicine, Ahmadu Bello University Teaching Hospital (ABUTH), Zaria *Corresponding author: Ogoina Dimie Immunology Unit, Department of Medicine ABUTH, Zaria P.O. Box 06 Shika, Zaria, Kaduna state Nigeria Telephon: +2348034510717 E mail: dimostic@yahoo.co.uk. Code Number: hs11025 Abstract Background: There is a dearth of studies on HHV8-HIV co-infections from Nigeria, even as both infections have
been shown to be endemic in Africa. This study examined the seroprevalence and determinants of HHV8 infections in
adult Nigerians with and without HIV-infection.
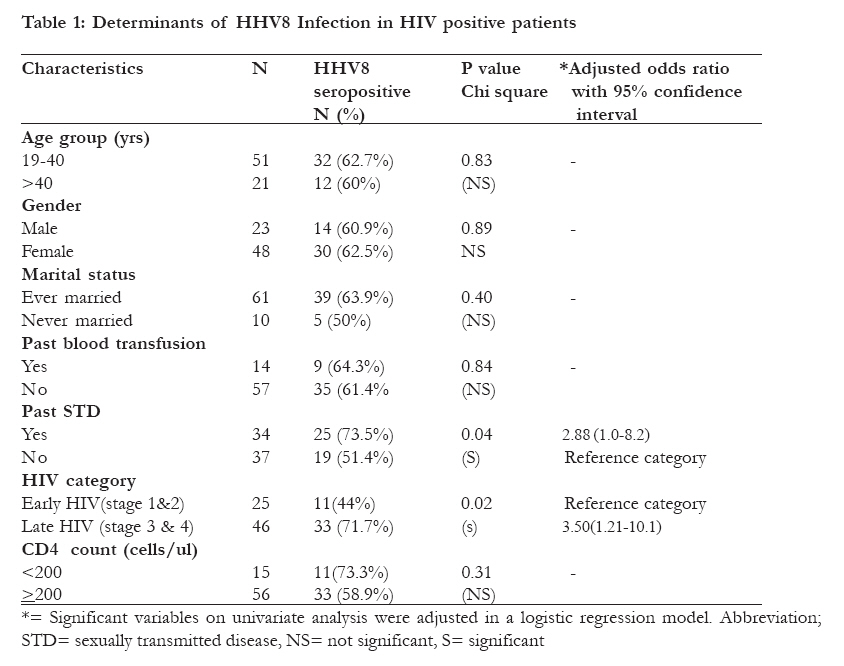
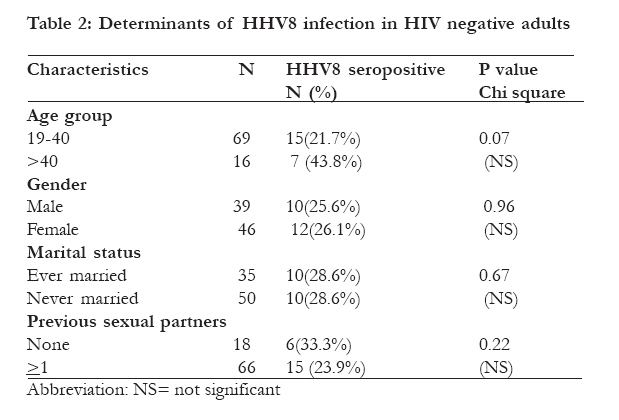
Key words: HHV8, KS, HIV-1, STD, Seroprevalence, Nigeria Introduction Human herpes virus 8(HHV8), also known as Kaposi's sarcoma associated herpes virus (KSHV ), is a member of the gamma herpes virus family established as the major aetiological factor in all forms of Kaposi's sarcoma (KS)1-3. The seroprevalence of HHV8 infection often mirrors the prevalence of Kaposi's sarcoma. Consequently, in many parts of Africa where KS is endemic, the HHV8 seroprevalence in the general population is often above 20% while lower rates ranging from 0-20% have been reported from countries in Europe and North America where KS occurs rarely1,2,4. The transmission of HHV8 has been shown to occur via body fluids such as blood and blood products, saliva, semen and vaginal secretions and rarely via organ transplantation2. Homosexuality, multiple sexual partners, sexually transmitted infections (STI) and transfusion of HHV8 infected blood are, therefore, some established risk factors for HHV8 infection in adult populations 2,5-7. In Africa, HHV8 infection is also endemic in children4 and intra-familial contact with infected saliva from infected adults has been implicated as a means by which children get infected with HHV8 in one study8. The current HIV pandemic has resulted in the emergence and re-emergence of AIDS-associated KS (AIDS-KS) in many parts of the world9. As an STI, HIV may not only facilitate HHV8 acquisition but may promote faster progression asymptomatic HHV8 infection to AIDS-KS via the tumour promotive effects of HIV-1 induced cytokines and HIV-related immunodeficiency10,11. Conversely, HHV8 infection may also facilitate faster progression of HIV to AIDS 12 by promoting trans-endothelial spread of HIV, by promoting infection of new HIV target cells as well as by inducing HIV-1 replication10,11. Human herpes virus 8 and HIV-1 infections therefore display synergistic interactions with adverse clinical consequences. While both HHV8 and HIV-1 infections are known to be endemic in many parts of Africa, there is still a paucity of studies on HHV8-HIV co-infections from Nigeria. Although, a study from the Lagos, south of Nigeria, suggested a predominant sexual route of HHV8 transmission in adults5, the seroprevalence and possible routes of HHV8 transmission among adults in northern Nigeria remain unknown as there are no studies from this part of the country. This study was carried out to provide preliminary information on the seroprevalence and determinants of HHV8 infection in apparently healthy adults of the general population and among HIV-1 infected patients without KS in Zaria, Northern Nigeria. We also sought to ascertain the clinical associations between HHV8 and HIV/AIDs by comparing HHV8 seroprevalence rates in relation to severity of HIV disease as determined by CD4 cell counts and HIV clinical stages. Methods Study population In a cross sectional study carried out in Ahmadu Bello university teaching hospital (ABUTH), Zaria, northern Nigeria, a total of 170 adults (80 HIV-1 positive and 90 HIV negative) without Kaposi's sarcoma were enrolled over a 6 months period in 2007. The HIV positive adults were enrolled consecutively as they presented to the ABUTH HIV/AIDS clinic. The HIV negative participants were apparently healthy adult volunteers (including students n=20; civil servants n=54 and traders n=16) of the general population in Zaria selected by convenience sampling. Data collection and Clinical examination A structured pre-tested interviewer-administered questionnaire was used to collate all study individuals demographic data, clinical details, social history, sexual history and other determinants of HHV8 infection such as past history of blood transfusion and past history of sexually transmitted disease(s). Patients were clinically staged into early HIV/AIDS (stage 1 and 2 WHO stages13) and late HIV/AIDS (stage 3 and 4 WHO stages13) diseases. Sexually transmitted disease was defined as self reported or clinically confirmed past or recent history of any one of the following - gonorrhea, syphilis, herpes genital ulcers and genital warts. Laboratory methodology All healthy adults were found to be HIV negative by 2 parallel rapid HIV screening assays while all patients were confirmed to be HIV-1 positive by western blot (Immunetics Inc, Qualicode HIV1/2 kit). All study subjects CD4 T cell counts were determined by flow cytometry (Partec, GmbH Munster Germany). Serum samples collected from all subjects were stored at -200 C until collectively analysed for IgG HHV8 anti-lytic antigen antibodies (BIOTRIN, UK) according to manufacturer's brochure. This test kit has a sensitivity of 90.4% and specificity of 93%. HHV8 results were interpreted as positive when samples were reactive and negative when samples were non-reactive. Equivocal samples were excluded from the final analysis. Ethical approval and informed consent for the study were obtained from the ABUTH research ethical committee and study participants respectively. Statistical analysis Data was analyzed using SPSS 15. Differences in variables were sought by student t test, chi square and fisher's exact test as appropriate. Significant determinants of HHV8 infection were adjusted in a logistic regression model expressed in odds ratio (OR) with 95% confidence interval (CI). P<0.05 was considered significant. Results Study population A total of 71 HIV positive subjects and 85 healthy participants were studied after excluding 9(11.2%) patients and 5(5.6%) healthy participants with equivocal HHV8 results. The mean ages plus standard deviation of healthy controls (33yrs± 9.13) and patients (36yrs ± 9.06) were similar (P>0.05, t test). All 71 HIV infected patients and 67 (78.2%) of the 85 healthy participants were heterosexuals with one or more previous sexual partners while 18(21.2%) of healthy participants were sexually naïve (no previous sexual intercourse). A history of STD was reported in 34 (47.9 %) patients and in 2(2.4%) healthy participants. None of the study participants were intravenous drug users. Clinical features and HIV/AIDS staging Five patients had clinical evidence of STD at time of study including 2 herpetic genital ulcers and 3 genital warts. The major diseases complicating HIV infection were tuberculosis (n=6) and HIV-associated diarrhoea (n=6). Forty eight (67.6%) of the 71 patients were asymptomatic at recruitment. Of the 71 patients, 25(35.2%) had early disease while 46(64.8%) had late disease. Seroprevelence and determinants of HHV8 infection Forty four (62%) of the 71 patients and 22 (25.9%) of the 85 healthy participants were HHV8 seropositive. This difference was statistically significant (p<0.001, X2= 20.64, df=1). The HHV8 seroprevalence in relation to the clinical characteristics of patients are shown in table 1. As shown in table 1, a past STD (OR= 2.88, 95% CI= 1.0-2.88) and late HIV/AIDS disease (OR=3.5, 95% CI= 1.21-10.1) were the only significant determinants of HHV8 in patients. The HHV8 seroprevalence was higher in patients with CD4 cell count <200cells/ul compared to those with CD4 >200cells/ul, albeit statistically insignificant. The HHV8 seroprevalence rate was not related to any of the evaluated variables in healthy participants (Table 2). However, 6 (33.3%) of the 18 healthy participants who had no previous sexual contact or previous blood transfusion were also HHV8 seropositive. These 6 healthy participants were young adult's aged 24-29 yrs. The healthy participants who had a past history of STD and previous blood transfusion (2 each) were all HHV8 seronegative. Discussion This study has revealed a HHV8 seroprevalence rate of 62% in HIV positive adults without Kaposi's sarcoma and 25.9% in apparently healthy HIV negative adults in Zaria, northern Nigeria. These high seroprevalence rates suggest that HHV8 infection is endemic in northern Nigeria but more prevalent in HIV infected adults, possibly because HHV8 and HIV-1 infections share common routes and risk factors for transmission. Similarly, Adjei et al14 in Ghana also reported a significantly higher HHV8 seroprevalence rate of 65.6% in HIV positive blood donors as compared to a 23.7% seroprevalence in HIV negative blood donors. Hladik et al6 in Ugandan also showed a similar trend with HHV8 seroprevalence rates of 39% and 63% in HIV negative and positive blood donors respectively. The finding of a significantly higher HHV8 seroprevalence rate in patients with a history of previous STD is supportive of a predominant heterosexual route of HHV8 transmission in HIV infected adults in Northern Nigeria. Heterosexual transmission of HHV8 infection has also been suggested from a study from Lagos,south-west of Nigeria where significantly higher HHV8 seroprevalence rates of 31% each were reported in commercial sex workers and individuals with sexually transmitted infections when compared to a 19% seroprevalence in apparently healthy adults of the general population5. The low rates of previous STD and past blood transfusion in the healthy HIV negative group as well as the finding of HHV8 seropositivity in sexually naïve healthy young adults, suggest a concomitant non-sexual and a non-blood transfusion-related route of transmission of HHV8 in young adult Nigerians. In a study of 56 children aged 2 to 14yrs from Calabar, south eastern Nigeria, a high HHV8 seroprevalence of 76.9%15 was reported, indicating active transmission of HHV8 among children by non-sexual routes. Although contact with HHV8 infected saliva has been proposed as a means by which children and young adults get infected with HHV8 in Africa8, the exact socio-cultural behaviours leading to exposure to infected saliva are yet to be fully defined in different Africa populations. In this regard, future studies are merited. Our study data is indicative of an adverse clinical association between HIV/AIDS disease and HHV8 infection as the HHV8 seroprevalence rates were found to be about four times higher in patients with late (stage 3 and 4 ) HIV/AIDS disease compared to those with early (stage 1 and 2) disease. Similarly, the HHV8 seroprevalence rate was found to be higher in those with low CD4 cell count<200cells as compared to those with CD4 cell counts >200 cells/u, albeit statistically insignificant. However, the suggestion of HHV8 inducing progression of HIV to AIDS in Nigerians can only be confirmed prospectively. A prospective study by Suchankova et al12 from Czech Republic revealed that patients with HHV8-HIV co-infection were more likely to progress from HIV clinical stage A to stage B. The absence of any clinical evidence of Kaposi's sarcoma in all our HHV8 seropositive patients with low CD4 count (below 200cels/ul) is supportive of the known role of factors other than immunosuppression in the pathogenesis of AIDS-KS 16. However, it is possible that some of our HIV-HHV8 co-infected patients may develop AIDS-KS in future, especially with the current emerging challenges of ART drug resistance and failure in the developing world 17. Conclusion HHV8 infection is endemic among adults in Northern Nigeria and particularly associated with advanced HIV/AIDS. The association with STD is supportive of a predominant sexual route of HHV8 transmission, although non-sexual routes of transmission may also be operative, especially in young sexually naïve adults. Acknowledgement We are grateful to staff of immunology unit, Department of medicine, staff of Haematology Department and staff of the ABUTH HIV clinic for facilitating this study. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11025t2.jpg] [hs11025t1.jpg] |
| |||||||||

{kind=link}
{kind=link}