 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 176 - 181 Nasal carriage of multi-drug resistant Staphylococcus aureus in healthy inhabitants of Amassoma in Niger delta region of Nigeria *Onanuga A, Temedie TC Department of Pharmaceutical Microbiology & Biotechnology, Faculty of Pharmacy, Niger Delta University, Wilberforce Island, Bayelsa state, Nigeria *Correspondence author Adebola Onanuga Department of Pharmaceutical Microbiology & Biotechnology Faculty of Pharmacy, Niger Delta University Wilberforce Island Bayelsa state, Nigeria Tel: +2348034524996; +2348050344034 E-mail: adebolaonanuga@yahoo.co.uk Code Number: hs11028 Abstract Background: Nasal Staphylococcus
aureus is a major source of community and hospital associated staphylococcal
infections. This study determined the prevalence of nasal S. aureus isolates and investigated their antimicrobial resistance profile
in healthy volunteers.
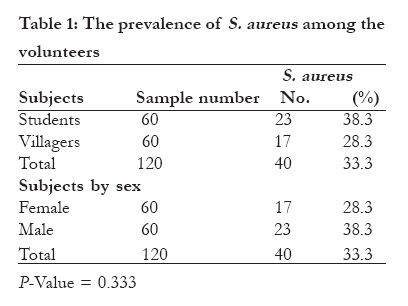
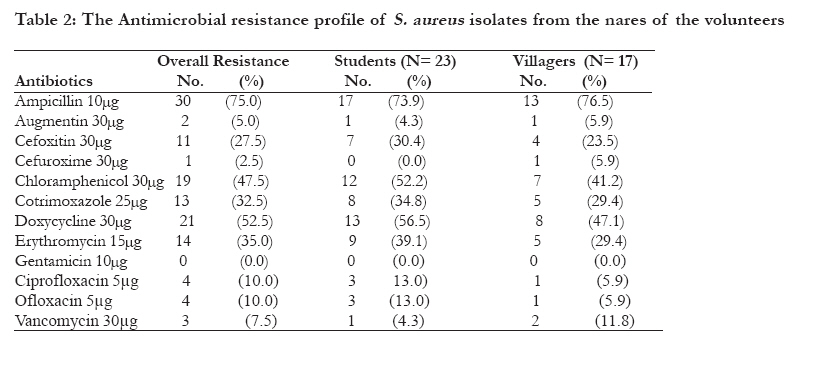
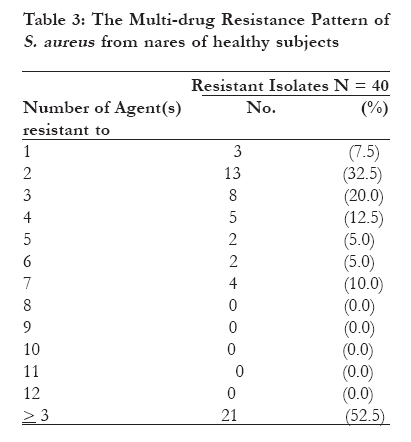
Keywords: Staphylococcus aureus, Nasal, Multi-drug, Resistance, Antimicrobial, Healthy Introduction Staphylococcus aureus is a leading cause of community-acquired infections particularly in colonized in humans1. It causes superficial skin lesions such as boils and furunculosis; more serious infections such as pneumonia and urinary tract infections; and deep-seated infections such as osteomyelitis and endocarditis2, 3. Colonized patients are the chief source of S. aureus in hospitals4, 5. S. aureus colonizes various parts of healthy humans such as the nares, skin, vagina and gastrointestinal tract1. Its prevalence have been severally reported in healthy populations; 36% and 40% were reported in women's urine in two centres in Nigeria, 17.3% in nasal cavity of Turkish children, 36% in nares of Japanese adults and 32.4% in nasal cavity of adults in USA 6-9. Colonizing strains may serve as endogenous reservoirs for overt clinical infections or may spread to other patients. S. aureus have become resistant to various antimicrobial agents including the commonly used penicillin-related antibiotics. Multi-drug resistant strains of S. aureus have been reported with increasing frequency worldwide. Strains that are resistant to methicillin were found to exhibit varying resistance to lincosamides, macrolides, aminoglycosides, fluoroquinolones, or combinations of these antibiotics2, 10. Vancomycin a glycopeptide which was initially very effective in the treatment of Methicillin resistant S. aureus (MRSA) infections is recently being witnessed with intermediate resistance from MRSA strains11. S. aureus from the anterior nares have been reported to be linked to most community and hospital associated infections; and recent study has also showed that nasal carriage is a source of S. aureus bacteremia12. Elimination of nasal carriage has been reported to cause reduction in the incidence of S. aureus infections13. Thus, the antimicrobial resistance profile of nasal S. aureus is of great public health concern especially in developing countries where health facilities are inadequate. Therefore, we report the nasal carriage of multi-drug resistant S. aureus in healthy inhabitants of Amassoma in Niger Delta region of Nigeria. Methods Study Population Nasal specimens were collected from one hundred and twenty (120) asymptomatic inhabitants of Amassoma community comprising of 60 students of Niger Delta University and 60 villagers. Amassoma is a very small village in Bayelsa state in South-South Nigeria where the new state university was established. The occupations of the villagers were trading, crops farming and fishing. Willingness of the subjects to participate in the study was a strong criterion. They volunteers gave informed consent by providing demographic data and were not on any antibiotic for at least two weeks at the time of sampling nor had been admitted into any hospitals in the last one year before the survey. They were of ages 15 to 35years comprising of 60 females and 60 males with each group contributing equal number. The nasal specimens were collected with labeled sterile swabs sticks and were taken to the laboratory within 2hrs of collection for inoculation on selective media. The study was carried out from February to July 2009. Isolation and Characterization of S. aureus Each of all the swab samples was inoculated onto sterilized Mannitol salt agar (Oxoids, U.K) plates and incubated at 37°C for 24 to 48h. The characteristic isolates were aseptically isolated and characterized using standard established microbiological methods, which include colonial morphology, Gram's stain reaction and biochemical characteristics14. Isolates that were Gram-positive cocci (grape-like clusters), positive to catalase test, slide coagulase test with human plasma and DNase test14 were considered as S. aureus in this study. Antibiotic susceptibility testing-Agar diffusion method (zone of inhibition measurement) Each of the isolates of S. aureus was standardized using colony suspension method and strain's suspension was matched with 0.5 McFarland standard to give a resultant concentration of 1.5 x 108 cfu/ml. The antibiotic susceptibility testing was determined using the modified Kirby-Bauer diffusion technique14 by swabbing the MuellerHinton agar (MHA) (Oxoids U.K) plates with the resultant saline suspension of each strain and the following six (6) antibiotic discs from Oxoids U.K, were placed on the plate after 20 minutes: cefoxitin 30µg (for detection of MRSA), gentamicin 10µg, ofloxacin 5µg, ciprofloxacin 5µg, doxycycline 30µg and trimethoprim/sulfamethoxazole (cotrimoxazole) 1.25/23.75µg. The plates containing the discs were allowed to stand for at least 30mins before incubated at 30°C for 24 h so as to favour the growth of methicillin resistant strains15. The diameter of the zone of inhibition produced by each antibiotic disc was measured and interpreted using the CLSI zone diameter interpretative standards16. Agar dilution method (MIC test) Standardized solutions of six (6) antibiotics; vancomycin (Novaplus, USA), ampicillin (Merck, Germany), erythromycin (Merck, Germany), chloramphenicol (Merck, Germany), amoxicillin-clavulanic acid (augmentin) (Glaxowellcome, UK) and cefuroxime (Glaxowellcome, UK) were aseptically prepared. These solutions were used to prepare MuellerHinton agar plates of varying CLSI minimum inhibitory concentrations (MICs) breakpoints16; vancomycin 2-12µg/ml, cefuroxime 8µg/ml, ampicillin 0.25µg/ml, erythromycin 0.5µg/ml, chloramphenicol 8µg/ml and amoxicillin-clavulanic acid (augmentin) 4/2µg/ml. The plates were spot inoculated with each strain's standardized suspension and incubated at 30oC for 24h15. Strains that showed growth on each of the antibiotic-agar plate were regarded as resistant to that antibiotic using CLSI breakpoints standard16. The isolates of S. aureus that were resistant to three or more of the tested twelve antimicrobial drugs were defined as multi-resistant in this study. Statistical Analysis Frequencies were obtained and percentages were calculated for study variables. Demographic characteristics were compared with the use of Chi square and Fisher's exact test (two tailed) with the SPSS statistical program (version 15). All reported P values are two-sided and A p-value of less than or equal to 0.05 is considered to be statistically significant (>0.05) Results A total of forty (33.3%) out of 120 nasal samples of healthy subjects screened gave S. aureus isolates. The University students appeared to have more yields than the villagers in the community but the difference is not statistically significant (P = 0.333). Also, the male volunteers appeared to be more colonized than their female counterpart as shown in table 1 but the difference is not significant (P = 0.333). The isolates showed high resistance to ampicillin 75%, doxycycline 52.5%, and chloramphenicol 47.5%; with 27.5% of the isolates being methicillin resistant (resistance to cefoxitin). The isolates were totally susceptible to gentamicin while very low resistance was observed against cefuroxime, augmentin, ciprofloxacin, ofloxacin and vancomycin (MICs > 16µg/ml)16 as shown in table 2. The observed differences in the isolates' resistance pattern among the volunteers' groups are not statistically significant (P > 0.05). Multi-drug resistance in this study was taken as resistance to three or more of the twelve antimicrobial drugs tested. Twenty one (52.5%) of all the isolates were multi-drug resistant, ten of them (47.6%) were methicillin resistant Staphylococcus aureus (MRSA) and only 3 (7.5%) was fully susceptible to all the antimicrobial drugs (Table 3). There was no difference in the level of multi-drug resistance in the two groups of volunteers (P = 1.0). Discussion S. aureus is a well-known pathogen with an alarmingly increasing level of developing resistance to most available antimicrobial agents2. Nasal S. aureus have been implicated in community associated infections like soft tissue infections17 and hospital infections like bacteremia12. Our study showed an overall prevalence of 33.3% of S. aureus in the nostrils of the volunteers which is in support with previous findings of Kuehnert et al. in U.S.A and Uemura et al. in Japan who reported a nasal colonization in healthy adults of 32.4% and 36.0% respectively1, 9. In contrary, Pant and Rai's findings revealed higher S. aureus nasal colonization rate (43.8%) in staffs of teaching hospital in Nepal 18. Also, in Abia state of Nigeria, Chigbu and Ezeronye19 reported 50% nasal colonization in both hospital and non-hospital subjects. Whilst, Adesida et al.20 reported a much lower (14.0%) nasal colonization in medical students in Lagos, Nigeria. These variations may be attributed to the characteristics of the population under study. A population that is on antibiotics as at the time of sampling may yield a much lower prevalence of S. aureus while a population from hospital settings may yield a much higher prevalence because of the high prevalence of infectious patients in that environment. Other factors that can cause variations may be sampling and culture techniques20. The occupations of the subjects in this study do not predispose them to high prevalence of nasal colonization of S. aureus. This study's high prevalence of nasal carriage of S. aureus further supports the fact that anterior nares remains a principal reservoir of this organism and there is need to eliminate its virulent strains because of their involvement in most severe community and hospital associated S. aureus infections in colonized individuals4, 11. The differences observed in the colonization rates between the groups of volunteers (university students and villagers) and the sexes are not statistically significant (P = 0.333). This means that neither sex nor educational status is a risk factor for nasal colonization of S. aureus and there is no activity of any of the groups that predisposes them to S. aureus colonization or infection. The susceptibility test results showed ampicillin to be the least effective agent with 75% bacterial resistance, this of course have been widely reported for S. aureus from various sites of healthy subjects6,7 and nosocomial infections21,22. This is basically due to the effect of beta-lactamases produced by S. aureus. The uncontrolled availability of the agent in every drug vendors, which leads to its frequent use and misuse exert greater selection pressure for the resistant strains23 thereby makes this agent almost useless in the treatment of staphylococcal infections. The observed moderately high resistance to doxycycline, chloramphenicol, erythromycin and co-trimoxazole may also be as a result of their uncontrolled usage in the environment which favours the increasing number of resistant strains due to selection pressure23. The observed resistance to cefoxitin (MRSA) 27.5% is higher than the reports of Gorwitz et al 241.5% in U.S.A, Chen and Huang25 13.6% in Taiwan and Olonitola et al.2614.85% in Zaria, Nigeria from anterior nares of healthy population, adults and school pupils respectively. However, Rijal et al.27 reported a much higher 56.1% nasal colonization in healthy school children in Nepal. This study's estimation of MRSA is based on the resistance to cefoxitin and not on the detection of mecA gene that codes for the production of the altered penicillin-binding protein (PBP2a) responsible for classical methicillin resistance. Olayinka et al.28reported absence of mecA gene in MRSA isolates in Zaria, Nigeria. Thus, further study on the potentials of these MRSA isolates is strongly recommended since some strains of MRSA without mecA gene are also being implicated in the cause of some severe infections in communities and hospitals28. The difference observed in the prevalence of MRSA between the groups is not significant (P = 0.730). The isolates also exhibited a lower resistance (7.5%) to vancomycin at 4 to 12µg/ml which is higher than the report of Olonitola et al.26 2.97%, this may be due to the classes of subjects involved. Vancomycin, a drug reserved for the treatment of MRSA infections, which in the past S. aureus exhibited 100% susceptibility to but in this study, S. aureus isolates in healthy individuals were seen to have 7.5% resistance (MICs > 16µg/ml)16 to vancomycin. The students and villagers had one (4.3%) and two (11.8%) isolates resistant to vancomycin respectively. The observed difference is not significant (P = 0.379) which implies that no special characteristics of the participants predisposes them to vancomycin resistance. This shows the alarming rate at which S. aureus develops cross resistance to antibiotics and thus, making newer agents becoming inefficient. The very low resistance observed to cefuroxime, augmentin, the fluoroquinolones and the fact that all the isolates were totally susceptible to gentamicin support previous finding6, 7, 29. The profound activities of these agents to the organism may be largely due to their mode of action which is principally bactericidal. The bacterium's very low resistance to augmentin may be due to the presence of clavulanic acid (a competitive inhibitor of beta-lactamases) that restores the antimicrobial activity of the beta-lactam antibiotic (amoxicillin) against S. aureus, a known beta-lactamase secreting bacterium. Cefuroxime is a second generation cephalosporin agent that is resistant to beta-lactamases and it is very effective in the treatment of S. aureus infections. These agents' activities on this organism in this environment may also be due to the fact that they are not so easily abuse because of their expensiveness and they are equally available in injectable forms which involve expert's assistance for their administrations. Thus, these agents can equally be used for the treatment of S. aureus infections. Our study report a high (52.5%) multi-drug resistant S. aureus isolates from anterior nares of healthy individuals in which 47.6% of them were MRSA. Findings from other researchers gave high multi-drug resistant S. aureus in hospital and community associated infections30, 31 but there appeared not to be any such report from nares of healthy populations. This findings call for great concern because it has been shown by previous studies that carriage of S. aureus in the nose appears to play a key role in the pathogenesis of infection4, 12, 17. This calls for strategies for elimination of nasal carriage of S. aureus so as to reduce the incidence of S. aureus infections. Conclusion The results emphasize the need to discourage antibiotics' abuse (a strong contributing factor of antimicrobial drug resistance in bacteria) in order to prevent the return of the consequences of a pre-antibiotic era. It also supports the need to implement strategies for elimination of nasal carriage of S. aureus, so as to prevent severe multi-drug resistant S. aureus infections in our environments. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11028t2.jpg] [hs11028t3.jpg] [hs11028t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}