 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 190 - 196 Low tuberculosis case detection in Gokwe North and South, Zimbabwe in 2006 *Chadambuka A1, Mabaera B1, Tshimanga M1, Shambira G1, Gombe NT1, Chimusoro A2 1University of Zimbabwe, College of Health Sciences, Department of Community Medicine *Correspondence author
Addmore Chadambuka
Health Studies Office
P. O Box CY1122
Causeway, Harare
Email:
achadambuka1@yahoo.co.uk
Code Number: hs11030 Abstract Background: Case detection is an important component of tuberculosis control programmes. It helps identify sources
of infection, treat them, and thus break the chain of infection.
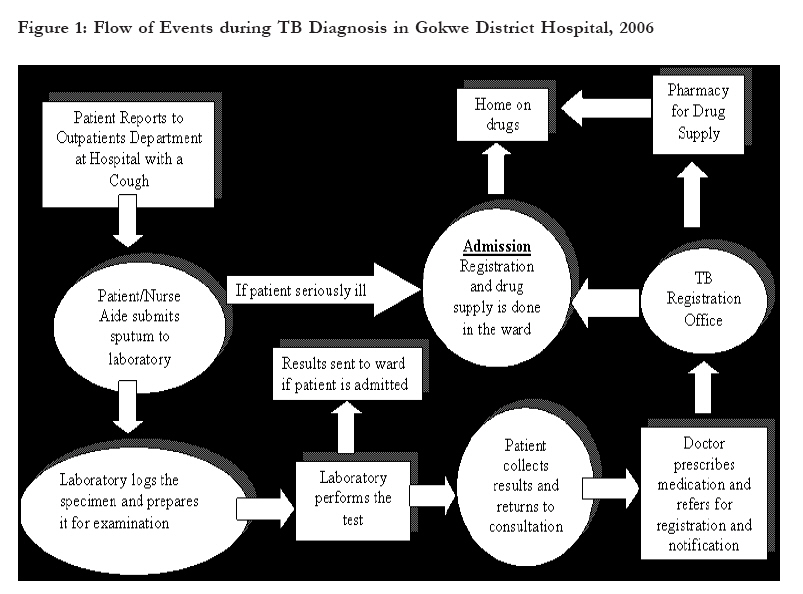
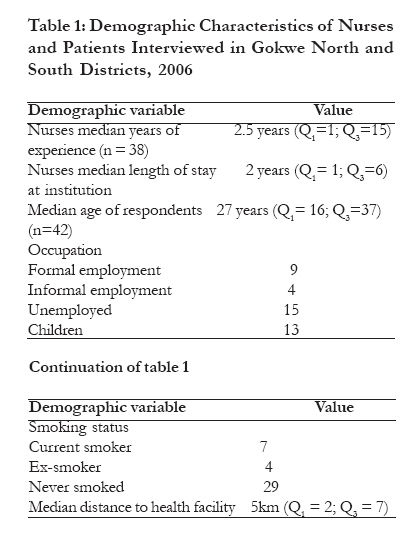
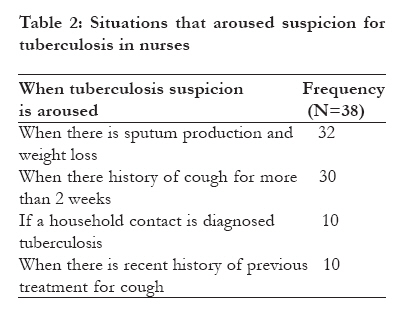
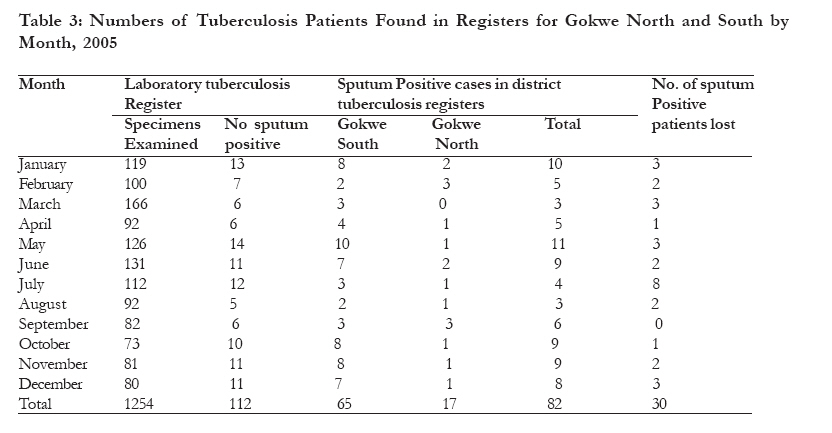
Key words: case detection, tuberculosis, Gokwe North and South, Zimbabwe Introduction Tuberculosis is caused by Mycobacterium tuberculosis and is spread through droplet nuclei from person to person. Pulmonary tuberculosis mainly presents with a cough of more than 2 weeks, chest pain, coughing up blood or sputum, weakness, weight loss, poor appetite, fever and night sweats1 Targets for tuberculosis control are detection of 70% of new smear positive cases and treatment success rate of 85% of detected cases made possible through systematic patient education, short course chemotherapy, decentralized clinic organisation and defaulter retrieving. This is complemented by public education, passive case finding with sputum smear microscopy and systematic investigation of household contacts.2-5. Case-finding is an essential component of the control of tuberculosis through identification of individuals discharging numerous tubercle bacilli. Treatment of these individuals rapidly renders them noninfectious, thereby cutting the chain of transmission. A secondary benefit is minimizing the delay in initiating treatment, thereby increasing probability of cure 4 Bacteriology remains the recommended method of tuberculosis case detection, first using sputum smear microscopy and then culture3. Missed cases are infectious until commenced on treatment. Each case has the potential of infecting 10-15 healthy individuals annually6. Globally every year about 100 million people are infected, 9 million develop active tuberculosis and 2 million die from it. Annual tuberculosis incidence is increasing by 1% per year globally7. In Africa the rate of increase is much higher due to higher HIV. WHO estimates that 1.6 million new infectious cases of tuberculosis and 600000 deaths occur annually making tuberculosis one of the commonest preventable causes of death in Africa8. The country recorded 87214 cases and 19516 deaths in 2004. The national incidence of sputum positive tuberculosis was 271 and 280 per 100000 for 2004 and 2005 respectively. National tuberculosis incidence per 100000 per year was reported as 674 and 681 per 100000 for 2004 and 2005 respectively. The notification rate was 434 per 100000 per year for the year 2004. Case detection rate for all cases was 64%. The notification rate for new sputum positive was 113 per 100000 per year. Case detection rate for the new sputum positive was reported as 42% and sputum smear positive tuberculosis incidence was 5 per 100000 in Gokwe North while in Gokwe South case detection rate was 25% and the sputum smear positive incidence was 18 per 100000. These figures were far below the national average incidence. 9-14 We evaluated causes of low tuberculosis case detection in Gokwe North and South Districts. Methods We conducted a cross sectional descriptive study of nurses, patients and TB records. One district hospital serves the two districts for diagnosis and treatment of TB. Nurses on duty during the study period were interviewed to assess knowledge and practices. We included all nurses that work in outpatients department at the hospital as they are the first point of contact where TB suspicion is critical. We also included all nurses at rural health centres. A total of 38 nurses worked in the rural health centres and the hospital OPD. The researchers stood at the hospital entrance used by all patients and asked the screening question. All patients leaving the hospital were asked whether they had a cough. Out of 457 patients screened, 42 patients reporting a cough of more than two weeks were included in the study. Twelve refused to answer the screening question. For patients who were children, the caregiver or parent who brought the child for treatment were interviewed. We checked for missed symptomatic cases during patient exit interviews. The TB coordinator, laboratory scientist and 3 members of the district health executive were key informants who were asked about patient flow and possible points of loss of patients. We described the activities that happen from the time the nurse suspects TB in a patient (Figure 1). District Tuberculosis and Laboratory registers and stock cards were reviewed from January to December 2005. If a patient was sputum positive in the laboratory of April 30, they were documented in May in the district TB register as sputum positive in April even though registration was in May. The patient appeared in the district TB register as an April patient, which date they were found positive. Following the spot, morning procedure for collecting sputum, patients submit 2 sputum specimens at one time and they are given one serial number. If the two specimens are both positive they are counted as one. We calculated the proportion of health workers with correct knowledge of the signs and symptoms of tuberculosis, proportion of nurses doing the correct thing when they met suspects and the proportion of suspect tuberculosis patients that were missed. Verbal consent was obtained from individual who participated in the study and confidentiality was assured. Patients who had cough for 2-3 weeks who were not screened were referred for reassessment. Permission was obtained from the Provincial Medical Director, the District Medical Officer for Gokwe and the Health Studies Office. Results Findings from Health Workers Demographic Information We interviewed all 38 nurses. The median length of service in the Ministry was 2.5 [Q1=1; Q3=15]. Only two nurses (5.3%) had received refresher training in tuberculosis management. The demographic characteristics of nurses are shown in Table 1. Knowledge A correct definition of tuberculosis was given by 35 (92%) nurses. Persons mentioned as being at risk of getting tuberculosis were those with compromised immunity, children under five years and those living in overcrowded places. Knowledge was high if respondents could give 3 or more symptoms of tuberculosis. Eighty seven percent gave 3 or more signs and symptoms of tuberculosis. Main symptoms mentioned were weight loss, cough lasting more than 2 weeks, haemoptysis and night sweats The mode of transmission was well known with 36/38 (95%) mentioning that tuberculosis was airborne. About a third of the nurses mentioned correct prevention measures. The correct duration of treatment was mentioned by 35/38 (92%) nurses and tuberculosis treatment drugs were well known. Nurses observed patients that had paid for chest X-ray (22/38) (58%) and sputum examination (11/38) contrary to national TB policy which states that these services should be free. Tuberculosis Diagnosis Nurses are expected to identify suspects, advise patients to cough up sputa after providing a specimen jar, complete the laboratory request form, direct the patient where to submit sputa (laboratory), collect results and document them on patient's card and then refer patient to the physician. Nurses knew the different methods ofdiagnosing tuberculosis. The gold standard for tuberculosis diagnosis was said to be sputum microscopy by 20/38 (53%) nurses. All the nurses knew that three sputum specimens were required for tuberculosis diagnosis but the correct frequency of sputum collection was known by 4/38 nurses. Table 2 shows when nurses said they would begin to suspect tuberculosis in a patient. Questions nurses asked to confirm tuberculosis suspicions were mainly history of household contacts with tuberculosis and history of night sweats. They would proceed to take weight (29/38), temperature (27/38), pulse (8/38), respiration (2/38). They would order sputum examination (37/38) and a chest X-ray (28/38). For tuberculosis diagnosis in children 14/38 nurses would check for growth faltering, another 14/38 respiratory symptoms lasting more than 3 weeks after antibiotic treatment and 9/38 would ask for history of household contact with smear positive tuberculosis. All nurses at clinic level (13/38) reported they would refer suspects to the next level on suspicion of tuberculosis. Main reasons for patient referral were suspicion of tuberculosis, failure to respond to antibiotic therapy and history of recent treatment for tuberculosis. Most nurses (32/38) said they had no tuberculosis suspect registers in their institution. Registers were not available for inspection where nurses reported having them. Most nurses (23/32) reported no means of suspect follow up while 9/32 said they referred issues of follow up to the tuberculosis office. Actions on diagnosis of sputum positive tuberculosis The nurses stated that they would give health education on tuberculosis (13/38), initiate contact tracing (7/38), examine contacts (3/38) and refer patients for voluntary counseling and HIV testing (1/38) following diagnosis of sputum positive tuberculosis Findings from patient exit interviews Exit interviews were done with 42 patients, (24 men and 18 females), whose median age was 27 years (Q1= 16; Q3= 37). Those formally employed were 9/42 while 4/42 were informally employed, 15/42 were unemployed, 7/42 were school children and 6/42 was below school and employment age. Interviews showed that 26/42 had never smoked, 7/42 were current smokers and 4/42 were ex-smokers. Table 1 shows the demographic characteristics of the patients. All the 42 patients interviewed had a cough history of 2weeks or more. More than half of the respondents (26/42) had a cough of 2-3 weeks while 10/42 had cough that was between 3 weeks and 3months and 6/42 had a cough of longer than 3 months. A history of previous treatment for cough was reported in 15/42 patients of which 6/15 said the cough was productive and 1/15 reported the sputum being blood stained. Only 1/21 patients remembered being asked about household contacts for the previous cough episode while 13/42 had been asked about household contacts with a cough for the current cough episode. We reviewed patients' cards. Twenty two patients had two cough episodes. On the first cough episode, 7/22 patients sought treatment for both cough and chest pain, 13/22 for cough only and 2/22 for chest pain only. Out of these, 4/22 were asked to submit sputa for examination and all were negative. On the current episode (coinciding with period of study) one of the patients who were initially sputum negative on the previous cough episode had converted to sputum positive. Most of the patients, 21/22 had sought help from a health facility. Patients reported having last sought medical help 1-3months previously were 11/22, more than 4 months were 7/22 and less than month were only 4/22. Patient knowledge on tuberculosis Most of the patients or their caregiver (38/42) had heard about tuberculosis before and 34/38 could give a lay definition of tuberculosis. Knowledge on how it was transmitted was correctly stated by 29/38 patients while 31/38 gave the correct signs and symptoms of tuberculosis. Findings from records Patient Management by Nurses Weight was measured in 39/42 patients, there was no history of weight loss in 38/42 and chest pain or breathlessness in 34/42. No history of smoking was documented by nurses. Records of treatment for previous cough episode were available for 21 patients. On that episode of cough 4/21 were asked to submit sputa for laboratory examination and the results of all four were negative. Two of the nineteen were asked to go for chest X-ray which they all did. On the current episode of cough that they had 9/42 had been asked to submit sputa for examination which they all did. Results were positive for 4/9 samples submitted. All four patients found sputum smear positive were notified and started on treatment. Two patients were asked to go for chest X-ray and one had the x-ray taken but the other did not as there were no more films. No patient had history of household contact(s) documented for both previous and current cough episodes. Tuberculosis Registers Review 2005 Results We reviewed the district tuberculosis and laboratory registers. One laboratory served the two districts but separate district TB registers were maintained. Sputum positive patients in the laboratory register missing in the district tuberculosis register were 30/112 (27%) as shown in Table 3. Laboratory Services and Equipment Checklist No stock outs of laboratory materials recorded in 2005. No breakdown of laboratory equipment was experienced. Spares were available. The X-ray machine had one major breakdown for about two weeks. Other Findings We reviewed with 5 key informants' tuberculosis patient flow within the hospital to identify possible points of loss of patients. Five key informants reported patients disappeared from outpatients department after submission of sputum specimens. Four reported patients were discharged from the wards before sputum results are out. Three reported patients were discharged from the wards before registration and decide not to report to the tuberculosis office. Another three key informants reported that those patients from the laboratory and wards that have inadequate identifying information recorded to allow for follow up were lost. Figure 1 shows the activities that occur from the moment a suspect presents at the outpatients department or rural health centre. Discussion Knowledge of tuberculosis among the clinicians was high. This high level of awareness is strength for the tuberculosis programme as it is likely to be associated with good case detection if it is accompanied by a high level of suspicion. Despite the good knowledge nurses had, they were not putting it into practice. The nurses' reported index of suspicion for tuberculosis was aroused by cardinal signs of disease but a few nurses remembered to consider previous history of treatment for cough and presence of a household contact with tuberculosis. This resulted in some suspects repeatedly treated for cough or living with a contact not being screened for tuberculosis contributing to low case detection. This was confirmed by findings of exit interviews where very few patients reported being asked about household contact with tuberculosis. The knowledge that nurses had did not translate into practice. A study in Harare found that among children who were contacts of sputum positive index cases, forty nine percent of the children evaluated had probable tuberculosis, 28% had suspected tuberculosis and 23% had no tuberculosis16. Children below five years who are contacts to sputum positive patients are at higher risk of getting tuberculosis17 and not asking about household contacts and investigating for tuberculosis in them resulted in missed cases. A study in Malawi showed that far less patients were requested to submit sputum than should have and this deficiency contributed to low case detection18. Requests for sputum examination were low in this study. With the high laboratory pick up rate seen from the sputa patients in this cohort submitted, more tuberculosis cases could be picked if sputa were submitted for more patients. No mechanism was available for tracking suspects. Infectious suspects who never turn up for investigation at hospital level continue to spread infection as missed cases. Suspect registers enable follow up of suspects and would improve case detection. The study reported very few nurses initiating contact tracing after the diagnosis of a sputum positive case. These cases are likely to infect close contacts at home or at work. A study in Peru showed that contact tracing was a powerful means of improving case detection rates for active tuberculosis disease19. Not initiating contact tracing and examination of contacts is a weakness and contributes to low case detection. The behaviour of seeking help first from health facilities is strength for improving case detection because most patients come to the health system first for help where diagnosis should be done correctly and promptly. Patient and caregiver knowledge on tuberculosis was high. Tuberculosis has become more and more common with the presence of HIV in the population. Most individuals, households or families have come in contact with tuberculosis either in the homes or at work. Record keeping and reconciliation is critical for improving case detection. Cases missing in the district register are probably due to delays in reconciling the two registers. Missing patients are as good as undetected patients because they continue to spread the infection. Also contributing to loss of cases is the patient flow around the hospital. The tuberculosis office is not conveniently located for patient access and thus patients may decide to move out of the institution without getting there. Study limitations We relied on what the laboratory reported. We did not have another laboratory scientist to perform test on negative(s) for confirmation as true negative. We may have missed cases this way. We did not conduct exit interviews at rural health centres and this might have increased or decreased case detection depending on the performance of nurses at these clinics Conclusion Low tuberculosis case detection was because nurses were not routinely requesting for sputum for examination in patients presenting with signs and symptoms of tuberculosis. The district was missing sputum positive tuberculosis cases due to delays in reconciling laboratory and district tuberculosis registers and inadequate identification details and addresses for follow up purposes resulting in early defaulters between diagnosis and registration. Recommendations We recommended that nurses should routinely ask about household/work contacts and request for sputum examination among patients presenting with a cough or a recent history of treatment for cough. The Tuberculosis Officer should conduct weekly reconciliation of laboratory and district tuberculosis registers to reduce on missed cases The district health executive should introduce a tuberculosis suspect register to all its health facilities to ensure that all tuberculosis suspects are captured and followed up. Contribution of the Research to Case Finding The study has shown that it is important to device mechanisms for tracking TB suspects. Conducting exit interviews with a focus on TB case detection helps to detect TB cases that might have been missed during consultation. Good record keeping and regular reconciliation of Laboratory and District TB Registers is critical for improving case detection. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11030t3.jpg] [hs11030t1.jpg] [hs11030t2.jpg] [hs11030f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}