 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
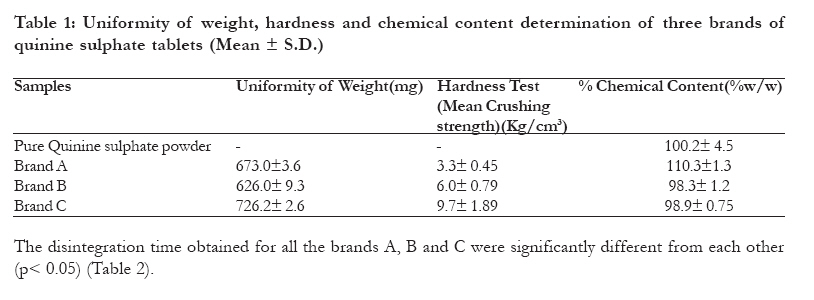
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 197 - 203 Evaluation of the physicochemical equivalence of three brands of commercially available quinine sulphate tablets from South Western part of Nigeria Adegbite AI, *Adegbolagun OM Department of Pharmaceutical Chemistry, Faculty of Pharmacy, University of Ibadan, Ibadan *Corresponding author Olayemi M. Adegbolagun Department of Pharmaceutical Chemistry Faculty of Pharmacy University of Ibadan, Ibadan Email: duplag03@ yahoo.com Code Number: hs11031 Abstract Background: The relatively little resistance to quinine globally has led to an increase in its use in P. falciparum malaria especially in multi-drug resistant strains.
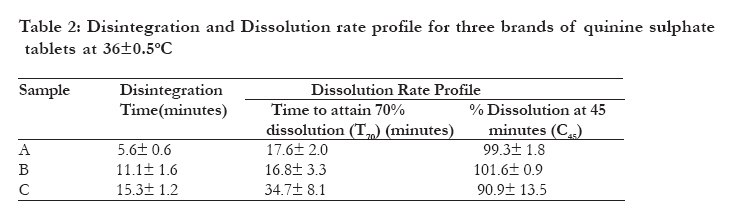
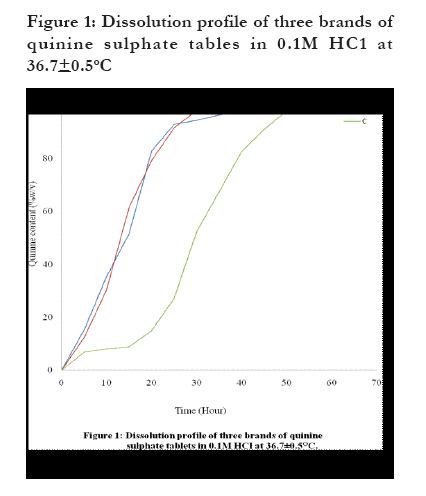
Keywords: Quinine sulphate tablets, non-aqueous titration, chemical equivalence, biopharmaceutical equivalence Introduction There have been many reports on the socio-economic burden of malaria in the developing world with the children being the most vulnerable with significant morbidities and mortality1. The failure of the various malaria control strategies in the recent past makes malaria a topical health and socio-economic issue in the developing world. The development of drug resistant malaria has necessitated a multi- sectoral approach to the management of malaria infection. This has resulted in the reintroduction of some older antimalarial drugs such as quinine and amodiaquine. Thus, interest is focusing the reintroduction of quinine as the 1st line of treatment for severe malaria especially cerebral malaria and also as a second line of treatment for uncomplicated malaria2. Quinine, a quinolone methanol, is the main alkaloid of Cinchona species. There is relatively little resistance to quinine worldwide3. It is a laevorotatory stereo isomer of quinidine and it is available in different salt forms which include hydrochloride, sulphate, dihydrochloride, bisulphate etc. Quinine has been used clinically in parenteral treatment of severe malaria andoral treatment of resistant falciparum malaria4. Although, decreasing sensitivity to quinine has been detected in areas of South East Asia, the strains of P. falciparum from Africa are generally sensitive to quinine5,6. In line with the WHO recommendation, the federal government of Nigeria adopted the use of Artemisinin-Combined Therapy (ACTs) drugs as first line antimalarial drugs. The ACTs comprises of the combination of artemisisnin derivatives with established antimalarial agents such as chloroquine and amodiaquine2. Earlier workers have reported in vitro and in vivo synergism between artemisinin and quinine7,8. The combination of artemisinin derivatives and quinine have been suggested for multidrug resistance areas where malaria transmission is intensive3. The choice, quality and time of commencement of anti-malarial drug use along with adequacy of dose of the drugs affect the overall efficacy of antimalarials, thus the quality of antimalarials is important in the roll back malaria programme. The sourcing of drug product from more than one source has been accompanied by reported cases of variability in clinical responses, which has been attributed to different formulation factors, methods of handling/production, packaging or storage factors as well as outright sub-standard product9. In line with the WHO guidelines, the National Agency for Food, Drug Administration and Control (NAFDAC), which is the drug regulatory authority responsible for the administration and control of drugs in Nigeria, has released standards of quality, efficacy and safety, which are aimed at getting the right quality of drug products to the consumers. Drug products that are chemically equivalent must be identical in strength, quality, purity while pharmaceutical equivalency is as assessed by similarity in content uniformity, disintegration and dissolution rates10. In Nigeria, chemical and biopharmaceutical inequivalencies have been reported for some brands of ampicillin and tetracycline capsules as well as ciprofloxacin hydrochloride and metronidazole tablets11,12,13,14. However, in a study on some brands of sulphadoxine-pyrimethamine tablets, chemical as well as biopharmaceutical equivalency was observed with three out of eight brands tested, while the remaining five brands were found not equivalent15. A report on the quality of some anti-malarials used in selected African countries revealed a significant problem of sub-standards with percentage failures of active ingredient content ranging from 20% to 67% for chloroquine tablets and 5% to 38% for sulphadoxine- pyrimethamine tablets. Dissolution failures ranged from 5 to 29% for chloroquine tablets and 75% to 100% for sulphadoxine - pyrimethamine tablets16. Similarly, substandard or fake artemisinin derivatives such as artesunate and dihydroartemisinin have been reported in some parts of South-East Asia with about 38 52% reported for artesunate17, 18. In view of the suggestion of the inclusion of the combination of quinine with artemisinin derivatives in the roll back malaria programme, there is the need to evaluate the quality of available quinine preparations in the healthcare delivery system so as not jeopardize the expected therapeutic outcome. The objective of this study was to evaluate the biopharmaceutical and chemical equivalency of the three brands of quinine sulphate tablets available within the South West part of Nigeria as at the time of this study. Methods Three different brands of quinine sulphate tablets from the same batch, with labeled contents of 300mg per tablet were obtained from different retail pharmacies in Ibadan which were representative of the brands available within the South Western part of Nigeria. All the tablets were in blister packs. Quinine sulphate reference pure drug was obtained from BDH Chemical Ltd, Poole England. Physical Examination of the tablets All the tablets were white sugar coated with similar shapes, thickness and diameter. Thin Layer Chromatographic identification 1%w/v pure quinine sulphate and its equivalent solution of tablets prepared in a solvent mixture of chloroform: ethanol (2:1), were identified using thin layer chromatography (TLC). The TLC condition involves the use of Methanol: strong Ammonia solution (100: 1.5) as mobile phase on Silica Gel G254 stationary phase with ultraviolet spectroscopy detection at 254 and 365nm19. Uniformity of weight determination Twenty tablets from each of the three brands were weighed individually using Mettler 1180 weighing balance. The average weights of the tablet were calculated as well as their percentage deviation from the average weight. The expected deviation from the mean for the average weight should not be more 5% 20. Hardness Test The crushing strength of five individual tablets per brand was determined using a Keetan tablet hardness tester. Tablet Disintegration Test This was determined at 37oC usingVeego disintegration testing apparatus until no particle remained on the basket of the system. The time taking for each of the six tablets tested in each of the brand was recorded. Dissolution rate determination (B.P. 2001)20 This was determined using the Veego dissolution rate testing apparatus using 0.1M HCl (900 ml) as the dissolution medium. The dissolution medium was maintained at 36.5 37.50C and the basket was rotated at 100 r.p.m. Samples (10ml) were withdrawn at timed intervals of 5minutes for 1hour. 10ml fresh dissolution medium was used to replace the withdrawn samples after each sampling. The samples were filtered and diluted appropriately before the absorbances were measured at 348nm using ultraviolet/visible spectrophotometer (Cecil Instruments Ltd, Cambridge, England). Six tablets were used from each brand. The content of quinine sulphate in each sample was determined based on the calibration curve obtained with serial dilutions of the pure drug at 5, 10, 20, 30, 40, 50 and 60µg/ml determined at 348nm using pure quinine sulphate powder. The regression equation for the calibration curve was y = 134.72x + 0.0035, r2 = 0.9948. The dissolution profiles of the different brands of quinine sulphate tablets were generated from the graph of the amount of quinine sulphate dissolved versus time. The average T70 (time for 70% of the active drug to be dissolved) and the amount dissolved at 45minutes were obtained for each brand. Chemical content determination Non- aqueous titrimetry using colour indicator end point was used for chemical content determination of the pure quinine sulphate powder as well as the quinine sulphate tablets (B.P.2001), crystal violet indicator was used as indicator20. 0.05g quinine sulphate powder or its equivalent in the tablet dosage form of the different brands were dissolved in a mixture of 1.8ml chloroform and 3.5ml acetic anhydride and titrated against 0.1M acetous perchloric acid using 0.5%w/v crystal violet solution as indicator until a bluish green end point. Blank titrations were carried and titre values were adjusted by deducting the blank determination from the assay. All the determinations were carried out in triplicate. Statistical analysis Student t-test and one-way ANOVA was used for the statistical analysis, p < 0.05 was taken as the significant level. Result The TLC analysis of the pure drug and the various brands gave Rf values of 0.50. All the tablets are sugar coated with similar shape and colour although with different inscriptions. All of the brands complied with the uniformity of weight determinations by not deviating by up to 5% from the mean value (Table 1). The mean crushing strength which is an indication of the hardness of the tablets showed that brands B and C gave similar crushing strengths, while the values obtained for brand A was the lowest (Table 1). The obtained values are statistically different between all the brands (p<0.05). The obtained dissolution rate profile revealed that all the brands attained more than 70%w/v dissolution by the 45minutes specified in the British Pharmacopoeia, the values were found not to be different statistically with p>0.05 (Table 2, Figure 1). However, the time to attain 70%w/v dissolution obtained was similar for brands A and B, while it is statistically different from that of brand C p<0.05 (Table 2, Figure 1). The result of the non-aqueous titration of the pure quinine sulphate powder and the three tablet brands is presented in Table 1. The pure quinine sulphate powder and brands B and C had values within the range specified in the B.P. of 99 101%w/v for pure compound and 95 - 105%w/v for the tablet dosage form (Table 1). However, the chemical content obtained for brand A was found to be higher than the official specification (Table 1). The % chemical content obtained for B and C were found to be similar with p > 0.05, while brand A was found to be statistically different from those of B and C (p<0.05) (Table 1). Discussion All the brands used were within their shelf life at the time of the study. The three different brands of quinine sulphate tablets obtained from different retail pharmacy outlets within Ibadan metropolis were found to be the same as those obtainable within the Southwestern part of Nigeria. The tablets were subjected to a number of tests in order to assess their biopharmaceutical and chemical equivalence. The assessments involved the use of both qualitative and quantitative methods of evaluation. The qualitative methods of evaluation includes tablet description i.e. colour size and shape, which were carried out by visual observation as well as active ingredient identification using thin layer chromatography (TLC). Quantitative evaluations on the other hand involves the used are uniformity of weight, disintegration and dissolution tests as well as chemical content determination. All the brands are similar in colour, shape and sizes as they are sugar coated white tablet with various identification inscriptions on them. The initial identification procedure using TLC revealed that all the brands contained quinine sulphate as they all gave similar Rf values of 0.50, which compares well with that of the reference pure quinine sulphate. All the brands complied with the uniformity of weight specification of 5% although brand A gave a deviation of 5.4% which is slightly higher than the 5% official specification but none of the tablet deviated by twice this value (Table 1). This indicates that the weights of the tablets in each batch within each brandare within the expected official specifications. The mean crushing strength determination is a measure of the degree of hardness of the tablets, brands B and C gave values above the recommended value of 4.0 Kg/cm3, while brand A was lower10 (Table 1). The obtained values were statistically different from each other (p<0.05). Although, the crushing strength is not an official method of assessing tablet quality, it is still useful in assessing the integrity of tablet dosage forms. However this may not be a problem with this drug as it is usually packed in blister pack. All the brands passed the disintegration test of less than 60minutes for coated tablets as specified in the B.P.20 (Table 2). Brand A had the lowest disintegration time. The obtained result seems to be in agreement with the crushing strength obtained for all the brands. The dissolution rate is a measure of the amount of drug released into the system with time. The dissolution profile of the three brands showed that all the brands met the official specification of 70%w/v dissolution at 45 minutes, (Table 2), however, the rate of dissolution was slower for brand C when compared with the other brands (Figure 1). The slower dissolution rate with brand C may be related to its hardness test and the disintegration time results in which it had the highest values when compared to the other brands. The dissolution rate of a drug is an important parameter in evaluating the absorption profile of drugs. A drug with poor dissolution profile is regarded as having poor biopharmaceutical characteristics, which may be a direct result of its formulation or method of manufacture. For a number of drugs such as frusemide, mefenamic acid, oxazepam and aspirin tablets, in vitro dissolution rate has been found to correlate with in vivo results assessed by bioavailability studies21,22. However, a lack of correlation between in vitro dissolution rate and in vivo bioavailability of one brand of paracetamol has been reported in a study on three brands of paracetamol tablets23. Thus caution must be exercised in the use of dissolution rate for the assessment of bioequivalence of different drug formulation. The result obtained in this study revealed a faster rate of dissolution with brands A and B, which may indicate a faster onset of action. The time for 70%w/v dissolution (T70) for the two brands were not significantly different from each other (p>0.05), however, the values are significantly different from that of brand C (p<0.05). Furthermore, the percentage dissolved at 45minutes were similar for brands A and B, while the values are higher than that of brand C, the difference in values were however found not to be statistically significant (p>0.05) (Table 2). All the values obtained are higher than the 70%w/v dissolution specification20, which may indicate that the overall bioavailability may not be affected by the difference in dissolution profile between the three brands. Dissolution rate has been reported to have a direct bearing on the bioavailability profile of tablet dosage forms as it can be used to predict the drug release pattern in vivo22. Although comparative bioavailability studies would be required to draw clinical conclusions, the differences obtained in the dissolution profiles may indicates formulation differences that could result in differences in bioavailability. The chemical content of the different brands were determined using a non- aqueous titration with colour indicator end point determination using 5%w/v crystal violet indicator (B.P. 2001). The pure Quinine sulphate powder as well as brands B and C gave a chemical content which were within the official specification, the values were found to be statistically similar (p> 0.05). However, the value obtained for brand A was higher than the official specification and it was statistically different from the other two brands (Table 1). The chemical content obtained for brand A in this study is above the official specification of 95-105%w/w (B.P. 2001). This shows that brand A failed the chemical content specification and could not be regarded as chemical equivalent of the other two brands. Previous studies by Onwujekwe et al (2009)24 reported that 46% of quinine tablets available in the South-East of Nigeria did not meet the USP requirement, while 23.8% and 74% substandard level was reported in Tanzania and Cameroon respectively by other workers25,26. The obtained result in this study however showed that the non-compliance with official specification of one of the brands is not a problem of being substandard but rather exceeding the specification. A similar study on the physicochemical equivalence of seven brands of chloroquine phosphate tablets found in the South West of Nigeria reported that two of the seven brands studied contained a level of chloroquine phosphate that exceeded the official specification27. While another report on eight brands of sulphadoxine-pyrimethamine combination reported that one of the brands contained more than the official specification for pyrimethamine15. Quinine exhibit dose-related toxicity28, thus the high chemical content of brand A, coupled with the low crushing strength, fast disintegration rate and rapid dissolution profile may have a definite impact on the bioavailability profile of this brand relative to the other two brands. This indicates that brand A may not be bioequivalent with the other two brands considering the overall expected bioavailability of all the brands. Conclusion Of the three brands evaluated in this study, Brands B and C may be regarded as chemical equivalents although they cannot be regarded as biopharmaceutical equivalents because of the significant differences in their disintegration rates and dissolution profiles. It was quite interesting to note that none of the brands is manufactured within the country, while only brand C is registered by the country's drug regulating agency (NAFDAC). The possibility of the interchangeability of the three brands of quinine sulphate tablets can only be verified by evaluating their bioequivalence. Acknowledgement The authors acknowledge Bond Chemical Industries, Ltd. Awe, Oyo State, Nigeria for giving access to their facilities for use during this study. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11031t1.jpg] [hs11031t2.jpg] [hs11031f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}