 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 228 - 239 Predictors of psychopathology among Nigerian adolescents: the role of psychosocial, demographics, personality and medical condition reports domains *Taiwo AO Department of Psychology, University of Ibadan, Ibadan, Nigeria *Correspondence author Dr. Abigail O Taiwo Department of Psychology University of Ibadan Ibadan, Nigeria E-mail: bolataiwo31@yahoo.com Code Number: hs11035 Abstract Background: Psychopathology among adolescents has become a global concern in the last decade.
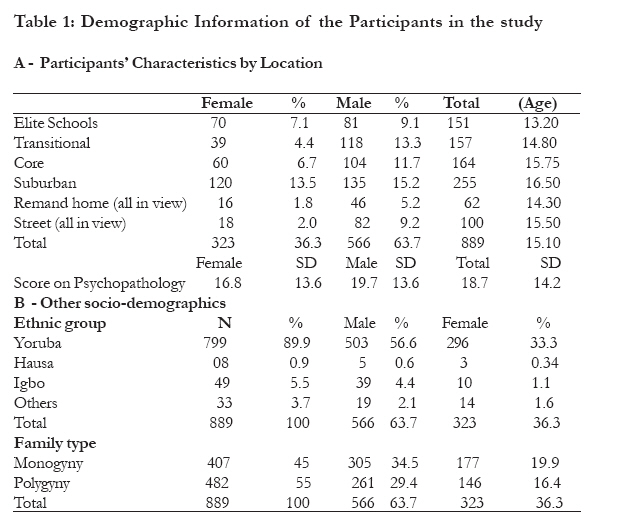
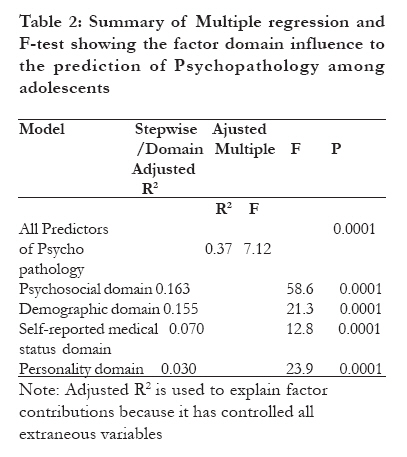
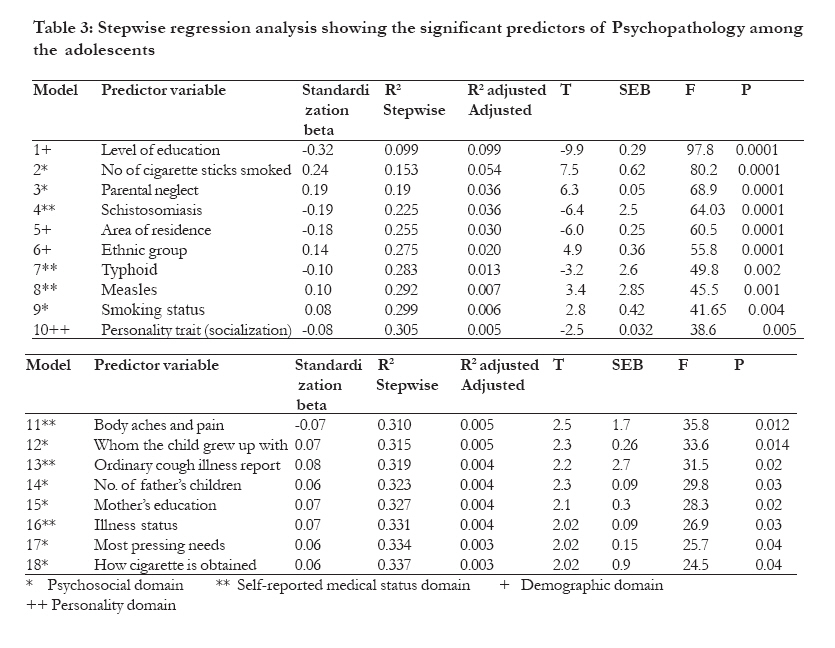
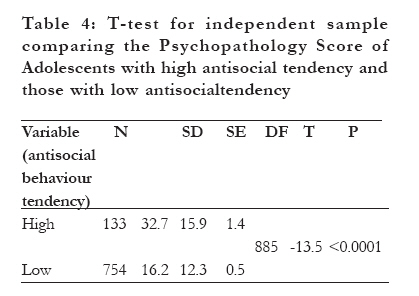
Keywords: Psychopathology, psychosocial, domain, antisocial behaviour, personality Introduction Adolescence corresponds to the period between the ages of 10 and 19 years and is a critical phase in the lifespan of development1, 2, 3. It is a bridge between childhood and adulthood, hence an important stage in the configuration process of the definite personality4. Although the need to pay great attention to adolescence is well recognised3, adolescent psychopathology is an area that is in need of research. However, it is known that the stage is characterized by instability and susceptibility to the development of psychopathology symptoms4. Psychopathology has been reported among adolescents worldwide5, but prevalence rates have varied across countries6. However, the most consistent prevalence rate was 18 % reported in studies from the United States of America and the United Kingdom 6,7. Logistic problems have made obtaining prevalence statistics impracticable in most developing countries. However, high prevalence of psychopathology among Nigerian high school adolescents has been observed8, 9. Early treatment is required for psychopathology with onset in adolescence because such adolescents are at risk of developing adult psychopathology10, 11, 12. For example, depressive symptoms are found to increase during adolescence and peak in early adulthood11, 13. Literature however indicated that there is dearth of treatments for adolescent psychopathology 4, 14, 15, 16.There is a need to determine the predictors of psychopathology during adolescence to aid the development of preventive and palliative programmes that could be applied to prevent early adulthood psychopathology. In order to meet this need, the current study adopted a multi-theoretical approach to present a model of explanation for reported psychopathology among Nigerian adolescents. Many theories have guided past research efforts to explain particular aspects of childhood and adolescent psychopathology. For example, human ecological system and attachment theories have long provided the most widespread explanation for adolescent psychopathology. The human ecological system theory17 postulates that environmental conditions including economic, family and political structures are part of life courses from childhood which determine the psychological well being of an individual. The attachment theory18 focuses on close, intimate, emotionally meaningful relationships which describe the biological system or powerful survival impulses that evolves to ensure the survival of a child during early developmental stages. The combination of the ecological system and attachment theories lay the background for some studies which examined the role of some psychosocial and socio-demographic factors in adolescent psychopathology. For instance, a significant positive relationship exists between social disadvantage, large family size, overcrowding and overactive and inattentive signs of attention deficit hyperactivity disorder among adolescents19, 20, 21,. Studies have also shown a significant association of familial factors (such as parenting, family type, family structure as well as family dysfunctions) with high psychopathology among adolescents22,23,24, 25, 26. Ethnic differences, low socioeconomic status and low levels of education are some demographic factors that have been implicated in the emotional and behavioural problems as well as unclassified psychopathology of adolescents, 7, 2127, 28.While the factors mentioned above fit perfectly into an `ecological system model', establishedcorrelates of psychopathology such as overt dysfunctions or divorce, neglect/abuse, unpleasant parent-child relationship, psychological factors such as dissociation, future time and value orientation27, 28, 29, 30 could fit into either `attachment model' or both. Associations of personality factors and somatic illnesses with psychopathology have also been established in the literature. A meta-analysis of 33 studies guided by theoretical personality framework revealed a significant relationship between neuroticism, conscientiousness, agreeableness and extraversion with psychopathology 31, thereby emphasizing the importance of personality in the understanding of psychopathology. According to the generalized interpersonal personality theory, personality is recognizable soon after birth and evolves through phases of socialization32, 33. Personality factors implicated for early manifestation and relationship to psychopathological symptoms among adolescents are role taking (also known as perspective taking) 34, 35, 36, 37, role perception and self concept38, 39 40, 41, 42. These factors are jointly referred to as "socialization", a psychological term which referred to the tendency to conform or not to conform to the values and norms of the society34. Studies focusing only on clinic samples also found adolescents suffering some medical illnesses (acute and chronic) reporting significantly high level of psychopathology43, 44, 45 but the understanding of this relationship remains unclear45, 46. There is evidence from literature that a high prevalence of psychopathology exists among clinically diagnosed or legally identified adolescents with high antisocial behaviour tendencies 16,47,48,49. A high correlation between conduct (CD) and attention deficit disorder (ADD) among these adolescents has been reported50. A similar result was obtained among the sample of delinquent juveniles in Russia51. These observed relationships between psychopathology and antisocial behaviour among adolescents made the American Psychiatric Association47 to conclude that adolescents with antisocial problems are part of a population within which there is higher incidence of psychopathology. These non-indigenous studies have however either focused only on clinic or legally identified adolescents. The current study aimed to expand its scope to include non-diagnosed adolescents in a Nigerian community. The current study investigated the role of gender factors, personality (So) and somatic illnesses on adolescent psychopathology, as well as bridged the gap of research among the non-clinic adolescent samples within Nigerian community. Specifically, a multi-theoretical model was used in this study to explain psychopathology amongNigerian adolescents. The following questions guided the focus of this study: (a) What factors are significant predictors of psychopathology among the Nigerian adolescents? (b) If the factors are grouped into domains following combination of related theories, what percentage of the variance observed in the adolescents' psychopathology will each explain? (c) Will the adolescents with higher reported antisocial behaviour also report higher level of psychopathology? An exploratory study was therefore designed to answer these questions. Method Study Setting The data collection took place within the convenient environment of each participating group. School participants were usually assembled in the school hall to fill their questionnaires while the street children were seen in their identified cluster areas (Mapo, Oje, Bodija, Agbaje, Gate and Sasa). Participants from the remand homes were assembled in the office space provided within their institutions at Polytechnic Eleyele Road, Ibadan and Oregun Road, Lagos. Participants The sample comprised 889 adolescents (566 males and 323 females). They were randomly sampled from nine secondary schools (school adolescents) (N = 727), street children (N=100) and remand homes (N= 62). Participating secondary schools were selected from the four stratified areas (elite, core, transitional and suburban) of Ibadan region. Characteristics of these areas are described in previous reports56, 57. Sampling from these areas was to ensure that participants were representative of adolescents from Ibadan region. Balloting; a simple randomization technique was used to select volunteers to participate as school adolescents in the study (adolescents who picked even numbers from a pool were selected). These school adolescents were drawn from junior secondary school class one (JSS 1) to senior secondary school class two (SSS 2). A snowballing sampling technique was used to recruit street adolescents. The volunteered street adolescents were drawnfrom established cluster areas within Ibadan, namely, Bodija, Beere/Mapo, Agbaje, Ojoo, Sasa and Gate. The remand home sample was drawn from two state Juvenile correction facilities located at Ijokodo, Ibadan and Oregun, Lagos. The participating schools and the number of adolescents are presented in Tables 1(a) and (b). Study design This study was a cross-sectional survey and adopted an ex-post facto design. Predictor variables (42 in all) were grouped into four domains of psychosocial, demographics, self reported medical conditions and personality, following the domain pattern of previous studies52, 53. The psychosocial domain included parental support, thought of danger if an adolescent sleeps outside the home without parents' knowledge (dissociation), value orientation, family type, family size, family status and social class status. Others were virginity (ever had sex), age at first sexual intercourse, smoking status, onset age of cigarette smoking, number of cigarette sticks smoked per day, future time perspective, death of parent(s), custodian of the adolescent and number of father's children. The demographic domain included sex, age, area of residence, birth-order, ethnic group, parent's level of education as well as educational attainment of the child. The self-reported medical status domain consisted of 19 medical conditions and described later under the instruments section. Each medical condition stood as a factor of its own. The score of the adolescents on Gough socialization scale (So) is the personality factor which represented the last domain in this study. The dependent variable in this study is a score of an adolescent on the self-reported psychopathology schedule. Previous explorative studies provide strong support for the enlistment of numerous factors 54, 55. Instruments Instrument used was a questionnaire which was in two versions, English and Yoruba. The questionnaire was divided into seven sections. Section one measured social and demographic factors such as age, sex, state of origin, ethnic group, birth order, family type, level of education, parental status, family size, parent's socio-economic status, etc. Section two measured future time perspective tapped from questions relating to the adolescents' future ambitions and things regarded as most valued. Section three was a 9-item parental support scale (PSS) 58. The scale measured perceived needs of the adolescents and examined their priority needs. It is a measure of parental support (tangible and emotional) for the adolescents. The author reported an alpha reliability coefficient of 0.80; N = 400 for the scale. Higher scores indicate low parental support (neglect). Section four was a 31-item self reported antisocial behaviour scale58. The scale measured the antisocial behaviour tendency of an individual adolescent. Sample items included; "I tell lies", "It is extremely difficult for me to keep a promise I made to someone", "I love to brag a lot", "I can not control my anger", "I enjoy disturbing others who are serious minded", "I have been personally involved in vandalizing properties", "I do not attend my school regularly because of my teacher's cane", "I gamble a lot", "I run away from home", and "I have been personally involved in setting fire on a property". Response options ranged from Never =1, Once = 2, 2-4 times = 3, 5-7 times = 4 to very often =5. Higher scores is indicated a greater tendency for antisocial behaviour. The author reported an alpha reliability coefficient of 0.91; N = 400 for the scale among adolescents. Section five was a 19-item self reported illness chart58. Response option was in a yes or no format. The scale was derived from frequently or recently suffered physical illness symptoms freely reported by adolescents. These reported/described symptoms were given to medical doctors who inserted the diagnoses in front of each symptom described. These formed the basis for the validation of the instrument. Sample items included, "When I urinate, I pass blood with it" (Schistosomiasis), "I frequently suffer aches and pains in my body" (body aches and pains), "I once had a swollen leg and a worm was extracted after some days of pain" (Guinea worm), "I am frequently wounded; I always nurse wounds" (wound), "I have a cough that won't subside even with the use of cough mixture, and when I cough, my sputum is usually stained with blood; I have also lost weight" (tuberculosis), and "I currently have a mild cough". Other illnesses assessed included gonorrhea, typhoid, measles, body aches and pain, stomach-ache, epilepsy, sickle cell, etc. A reliability coefficient alpha of 0.97 was established for the scale among adolescents in Ibadan (N = 400) 58. Section six was a 46-item Socialization Scale (So) 34, 35. The scale was adapted and validated among adolescents in Ibadan with a reliability coefficient alpha of 0.88; N =40058. So was used in this study because it is assumed that at adolescent's stage, personality traits are not yet completely formed. So measures the degree of socialization that an individual has attained and also identifies individuals' role perception and self concept. So was derived from the role taking theory30 and represents a theoretically important personality variable in socialization30. Studies which find So predicting those who are likely to develop behavioural and emotional problems among adolescents at later years have been reported in some parts of the world32,33. The response option was in True or False format. A high score implies inadequate socialization and dysfunctional role taking. Section seven was a 35-item psychopathology symptom schedule originally designed as the Pediatric symptom checklist (PSC) 59. The scale was adapted and validated for use as a self reported measure among adolescents (N = 400) in Ibadan metropolis58. A cut off point of 32, which is one standard deviation above the mean ( = 18; SD= 14), was established for the scale but the original authors59 established a cut off of 28 for their American population using ROC curve. A test-re-test reliability range of r = 0.84 - 0.91 was reported for the PSC 51. Studies have also indicated strong internal consistency (Cronbach alpha range of 0.91-0.93) of the scale when inter-item analysis was carried out on the items58, 60, 61. Sample items included "I complain of aches or pains", "I spend more time alone", "I have problem concentrating", "I feel I am bad", "I fidget a lot (unable to sit still)", "I feel sad, unhappy", "I have problem sleeping", "I feel irritable, easily angered", "I blame others for my troubles", and "I take unnecessary risks". The response format ranges from Never = 0; Sometimes = 1 and often = 2. The scale was reported to be sensitive to the presence of psychopathology symptoms for children and adolescents. It was chosen in this study because it is a quick screening tool for psychopathology among children and adolescents. Translation of the original questionnaire to Yoruba was carried out by a professor in Yoruba Language. The translated version was later given to 10 Yoruba speaking individuals to judge whether each item was the same with the original English questionnaire (expert judgment). A consensus agreement was reached that the Yoruba version measured the same concepts as the English version through at least 90% support of the experts on each item. This questionnaire was later administered to twenty adolescents who could read and understand both English and Yoruba. They were first administered an English version and were later administered the Yoruba version after two weeks. Their responses were subjected to a test-retest reliability exercise which generated a reliability coefficient of r = 0.93, suggesting that the two versions measured same construct. Procedure For the school adolescents, initial contact was made with the Principal of each school who assisted in obtaining consents from parents two weeks before the study commenced. Day for the data collection was fixed for each setting. Participants were then assembled in each of their settings and were again briefed on the purpose of the study and how to fill the questionnaire. Each participant from the street and remand home was individually assisted to fill their questionnaires because a majority of them could not read or write. Assistants who had been previously trained and were familiar with the questionnaire helped in filling the questionnaires which took about 40-50 minutes to complete. The general response rate among the participants was 89%. A total number of 1,010 questionnaires were administered; 1,000 were returned out of which 889 were completed. Snacks and soft drinks were provided for participants to compensate for the time spent in filling the questionnaire. Data analysis F Test, Multiple and stepwise linear regression as well as t-test were conducted to determine the domain as well as the variables that predict psychopathology among the sampled adolescents. For all the analyses, the computer programme SPSS 10.0 was used. Ethical consideration Permission for this study was obtained from the Research Committee of the Faculty of the Social Sciences, University of Ibadan, Nigeria. School participants and their parents were duly informed about the purpose of the study. Consent was obtained from the parents of school participants two weeks before the administration of the questionnaire but parents of remand home and street participants were not available for consultation. Permission for data collection was obtained from the Oyo State Ministry of Women Affairs and Youth Development and the Chairman of the National Union of Road Transport Workers (NURTW) for the remand home and the street adolescents respectively. Consent to participate was also obtained directly from all participants before each questionnaire was filled. A medical doctor from the University College Hospital was available to provide referral for those who needed medical attention. Results Descriptive characteristics The age range of the participants was between 10 and 18 (=15.2, SD = 2.4). One hundred and thirty-six (136) of the participants scored one standard deviation above the mean on psychopathology symptom schedule implying that there was a prevalence rate of 0.152 (i.e. 15%) for this sample (female score = 16.8; male score = 19.7; Total score = 18.7; SD = 14.2 ). The number of participants from each location and some important descriptive information are presented in Table 1 below. Two schools each were from elite, core and transitional areas but three were from suburban areas. The mean ages of adolescents from the core and suburban areas were relatively higher compared to those from elite and transitional areas (Table 1). The table also shows that there were more participants from Yoruba ethnic than other ethnic groups. This should be expected because the data was collected in a Yoruba ethnic dominated area. Predictors of Psychopathology This study sought to answer the three questions posed earlier. The first and second questions sought to identify significant predictors, as well as examine the influence of the theoretically and literature guided domains on psychopathology among Nigerian adolescents. To answer these questions, the 42 factors earlier listed were fed into a multiple regression model. These factors were essentially subjected to a correlational analysis. There was an assumption of equal chance for all the factors to enter in the equation irrespective of whether they directly affect the adolescents' psychopathology or mostly operate indirectly through other factors. These factors were also grouped into domains as previously mentioned and F-test was conducted to examine the contribution of each domain. The result of this exercise is presented in Table 2 below. Results from Table 2 above indicate that all the 42 variables jointly and significantly accounted for 37% of variance observed in the reported psychopathology of participants. F test revealed that psychosocial domain contributed 16.3%, demographic domain contributed 15.5 %, self reported medical illness contributed 7% and personality (So) which contributed 3%. In order to identify significantpredictors among the 42 variables, a test of multicollinearity was conducted and two factors (Number of father's wives and number of mother's children) were removed because their tolerance score was below 1 and VIF greater than 1061. The remaining forty were subjected to a stepwise regression analysis. Result is presented in table 3. Table 3 shows that 18 steps finally emerged after the stepwise eliminated non-significant factors. In all, eight factors were psychosocial (*=08), six were self-reported medical status (**= 6), three demographic (+=3), and one was personality (++=1). The beta weight for each factor indicates the kind of relationship that exists between the factor and psychopathology. Model one of the stepwise showed that there was a negative linear relationship between the level of education and adolescent's psychopathology score (B =-0.32; p<0.0001) while model eighteen showed "How cigarette is obtained" to be positively related with psychopathology (Table 3). The last question seeks to establish whether the adolescents with higher reported antisocial behaviour also report high psychopathology. A t-test for independent sample was employed and the result is presented on Table 4 below. The results in Table 4 above shows that adolescents with high antisocial tendency had significantly higher psychopathology scores compared to adolescents with low antisocial tendency (t (885) = -13.5; P<0.0001). Discussion This exploratory study examined the influence of 42 factors previously implicated in literature on psychopathology among Nigerian adolescents. Not all factors associated with adolescent psychopathology were examined For example, the role of genetic and neurobiological factors previously identified in literature for the development of adolescent psychopathology64, 65,66,68,69 were not included in this study. The factors examined were grouped into domains of psychosocial, demographic, self reported illnesses and personality (table 2). Multiple regression analysis showed that all the factors jointly explained 37% of variance observed in the reported psychopathology of the participants (table 2). F test revealed that psychosocial domain, demographic, personality (So) and self reported illnesses significantly influenced and respectively explained the 16%, 15%, 7% and 3% variance observed in the adolescent's reported psychopathology scores. The result added to previous empirical evidences17, 18, 19, 20 in support of some existing theories that provide explanations for adolescents' psychopathology. The stepwise regression analysis showed three demographic factors (table 3, models 1, 5 &6) as significant predictors of reported psychopathology among adolescents (contributing 6%, 3%, and 2% respectively) to the variance observed. The linear relationship in the first model implied that a higher report of psychopathology corresponds with lower level of education but no causal link is implied. There is a strong support from past findings for this result9, 8, 28, 61. Literature is not specific about which one leads to the other between low educational attainment and psychopathology. However, certain externalizing psychopathology (e.g, attention deficit and hyperactivity disorders) might be precipitated by low educational attainment, while some other forms of psychopathology might be responsible for low educational attainment9, 8, 28, 61. The relationship seems complex and requires further assessment and research. Areas of residence and ethnic group were other demographic factors identified as significant predictors in the model. The result gained support from literature7, 21. From past findings, certain characteristics described each residential area and the characteristics of suburban and core areas were found to be similar39, 56. Adolescents in both areas are described as having a low social class status, live in overcrowded houses and have less stimulatory neighbourhoods39, 56. The elite are described as people of high profile who occupy the middle and high social class strata. They can afford private schools, live in well built, well fenced houses in structured neighbourhoods39, 56. On the other hand, the transitional areas abhor both the elite and the traditional people (core). Their low cost houses are seen side by side with the high profile houses56. Further study may compare the level of psychopathology among adolescents from these varied areas. The influence of ethnicity on psychopathology in Nigerian adolescents needs further investigation given the diversity of culture and ethnic groups in Nigeria. This study was conducted within a Yoruba ethnic dominated area. From the psychosocial domain, familial factors (parental neglect, number of father's children, mothers level of education as well as whom the child grew up with) were all positively and significantly related to reported psychopathology among the adolescents (Table 3, models 3, 12, 14 and 15). These factors have been shown to be strong risk factors for adolescent psychopathology in past studies19,22,23, 27. All cigarette smoking indices were significantly related with psychopathology. Models 2 and 9 on Table 3 indicate that tobacco smoking and number of sticks smoked daily are significantly related to reported psychopathology symptoms. Abuse of substances (e.g. tobacco smoking and alcohol) has been previously found to be related to adolescent psychopathology63, 64. This result did not implicate a causal relationship; researchers are of the opinion that psychopathology may both precipitate and/or result from adolescent substance abuse65, 66, 67. Adolescents' reported illness status also relates positively with reported psychopathology symptoms (table 3). Previous studies have reported a positive relationship between some somatic illnesses and psychopathology among clinic adolescents43, 44, but this study is unique in that it sampled non clinic adolescents to report symptoms of clinically diagnosable conditions. Stepwise model showed schizotosomiasis, typhoid, measles, body aches and ordinary cough securing significant linear relationship with reported psychopathology. Some aspects of this relationship may not be as clear as noted earlier 45, 46. Since a causal relationship is not implied, it is possible that there are more adolescents with high psychopathology reports among those who migrate from the street to a flowing river to have a bath and in so doing contacted schizotosomiasis which is a water borne disease. Body aches and pain might be indicative of some other subtle conditions such as physical child abuse which can trigger the development of psychopathology. Acute symptoms of measles and typhoid may be similar to symptoms of psychopathology, particularly the externalizing symptoms which could explain its relationship with psychopathology among the adolescents, but caution must be exercised in interpreting this situation. Further investigation into these conditions may provide better information that will be useful for effective management of adolescent psychopathology. Another identified significant predictor of psychopathology is personality (So) which contributed 0.03% to the explanation of the variance observed in the reported psychopathology of the adolescents (Table 3). Previous studies reported similar findings34, 36, 37. However, the result has implication for further studies which will identify specific psychopathology symptoms that are associated with personality (So). Table 4 has also confirmed the previous findings16, 47, 48, 49 that adolescents with a high antisocial tendency might truly be part of a population within which there is a higher incidence of psychopathology Limitation of study This study has utilized self reported techniques all through. This can not guarantee the objectivity of the symptoms reported by the participants. Future studies may combine both self report and objective diagnostic measures to identify psychopathology and physical illness symptoms. The study has not established any causal link between the variables. Future study may also examine how patterns of psychopathology are predicted by the factors examined in this study. The study has not claimed total coverage of all factors responsible for or that play a role in adolescent psychopathology. Other factors such as genetic and neurobiological 56,57,58,59 should therefore be given adequate attention in this community. More so, the prevalence rate of 15.2% established in this study was based on one standard deviation above the mean score of participants on reported psychopathology. An extensive study which will focus on establishing the prevalence rate of psychopathology among adolescents in Nigeria is therefore suggested. Study implication The study implies that comprehensive assessment is required before commencing treatment for adolescents with psychopathology. Urgent further studies designed to investigate causal factors of psychopathology are implicated as these will aid the development of effective treatment for adolescent psychopathology. The results also imply that experts providing treatment for adolescent psychopathology should not overlook any co-morbid physical illnesses as well as substance use such as tobacco smoking. It also implies that adolescents suffering from psychopathology might benefit from programmes designed to enhance perspective/role taking and improve interpersonal negotiation skills. Also, severely antisocial adolescents, particularly children legally identified and placed in correctional homes should be examined for underlying psychopathology and treatment should be comprehensive. Conclusion This study has provided empirical justification for a multi-theoretical model of explanation for psychopathology among Nigerian adolescents. The study has also provided empirical support for existing ecological, attachment and personality theory in developmental psychopathology to explain adolescent psychopathology, but asserts that a single theory approach will not be adequate to explain adolescent psychopathology. A combination of theories is suggested. A research which is community based would provide better information on children and adolescent psychopathology than clinically based ones in the Nigerian community where children and adolescents suffering psychopathology are rarely referred to experts, and where there are many adolescents suffering in silence due to lack of treatment for their psychopathological symptoms. Recommendation It is recommended that a multidisciplinary and holistic approach is required in the treatment of adolescent psychopathology in the Nigerian community. More comprehensive research into predictor variables is also recommended. The environment of the adolescents, as well as internal factors such as personality should be given full consideration if treatment effectiveness and sustainability will be achieved. Parents are advised to pay more attention to their adolescents and report any strange behaviour observed in their wards to mental health experts who understand their problems and can proffer adequate treatment. This is important to avoid degeneration to greater psychopathology in the later years with its attendant problems. More attention is required from experts towards the treatment of unreached adolescents, particularly those who live on street and in correctional homes. Reference
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11035t3.jpg] [hs11035t4.jpg] [hs11035t2.jpg] [hs11035t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}