 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 244 - 251 Micturitional dryness and attitude of parents towards enuresis in children attending outpatient unit of a tertiary hospital in Abeokuta, Southwest Nigeria *Senbanjo IO1, Oshikoya KA2, Njokanma OF1 1Department of Paediatrics and Child Health, Lagos State University College of Medicine, Ikeja, Lagos State, Nigeria *Correspondence author Dr. Idowu O Senbanjo Department of Paediatrics and Child Health Lagos State University College of Medicine PMB 21266, Ikeja, Lagos, Nigeria Tel: (+234) 08067777363 E-mail: senbanjo001@yahoo.com Code Number: hs11037 Abstract Background: There is significant variability of the age at which children achieve dryness.
Key words: children, dryness, enuresis, parents, attitude Introduction Urinary incontinence is uncontrollable leakage of urine.1 This could be of the organic or functional type.2 In organic urinary incontinence, there is an underlying disease process that affects the anatomical layout or neural control of the urinary tract. However, in functional urinary incontinence, there are no structural or neurological abnormalities identified. Functional incontinence covers a heterogeneous group of disorders that include enuresis, urge syndrome, dysfunctional voiding and vaginal voiding. The majority of cases of urinary incontinence seen in children are included in this category.2 According to the International Children's Continence Society; 1, 2 enuresis or nocturnal enuresis is wetting episodes that occur in discrete amounts during sleep. On the other hand, day time incontinence or diurnal enuresis is unintended voiding of urine that occurs during the day or wake portion of twenty-four hours.1, 2 Enuresis is commoner in childhood than day time incontinence with about 80 % of children with enuresis wetting only at night.3 In the United States of America, about 5 - 10% children still wet the bed by age 7 years and less than 5 % are affected by age 10 years.4 In Igbo-Ora, a rural community in southwestern Nigeria, the prevalence of nocturnal enuresis among children aged 6 to 12 years was 17.6 %.5 There is no particular age by which the normal child will achieve control of micturation while asleep.3, 6 According to evidence of physiological maturation, 10 % of children are capable of establishing such control by 2 years of age, 48 % by 2.5 years and 78 % by 3 years.4 However, there are factors such as psychosocial events (e.g. acrimonious divorce) and medical disorders such as diminished bladder capacity, inadequate production of Anti Diuretic Hormone (ADH) at night, constipation and Urinary Tract Infection (UTI) which affect the development of continence in a child.6, 7 In the African context, the underlying pathology may be difficult to exclude than in developed countries as a result of constraints to doing laboratory test and prior blind treatment with antibiotics. Additionally, the age of expected dryness vary from one society to the other.6 This could lead to delayed presentation to the hospital of cases of enuresis that need to be evaluated and treated. Although bedwetting has a high rate of spontaneous remission, its occurrence bring social stress, emotional stigma and inconvenience to both the child and the family.8-10 Children who wet the bed experience parental disapproval, sibling teasing and a lower self esteem.11 This study was therefore carried out to determine the age of dryness, knowledge and attitude of parents about enuresis, prevalence of enuresis and factors associated with dryness and enuresis among apparently healthy urban Nigerian children. Methods This is a cross-sectional hospital-based study of micturational habit of children seen at the outpatient unit of Federal Medical Centre, Idi-Aba, Abeokuta between 1st of June to 31st of August, 2006. The hospital has 250 beds and provides primary, secondary and some tertiary health care. Abeokuta is in southwestern Nigeria and the capital of Ogun state. It has a population of 416800 people. Sampling The subjects were children who have recovered from acute illnesses such as malaria, septicaemia, diarrhoea disease and bronchopneumonia and are been followed-up at the general paediatrics outpatient clinic between 1st of June to 31st of August, 2006. Using the estimated prevalence of enuresis of 17.6 % by osungbade and Oshiname, the minimum sample size (n) for the study was calculated as follows: n = z 2 p (1 p) ÷ d 2. Where: `z' is the critical value and in a two-tailed test it is equal to 1.96, `p' is the estimated prevalence of stunting, `d' is the absolute sampling error that can be tolerated. In this study, it was fixed at 5 percent. Therefore the minimum sample size: `n' = 1.96 2 x 0.176 x (1 0.176) ÷ 0.05 2 = 223. Those with sickle cell disease, neurological disorders and clinical features suggestive of urinary tract infections were excluded from the study. Also excluded from the study were those whose age was doubtful and those whom the parents or guardian could not remember the age at which they became dry at day and at night. In all, eleven patients were excluded from the study. They include seven children whose mothers could not remember the age at which they became dry, three children with cerebral palsy and one child with fever and supra pubic tenderness. Ethical clearance Ethical clearance was obtained from the Federal Medical Centre Research/Ethics Committee and informed consent was taken at contact from accompanying parents or guardians. The data collected from the guardian or the patients, using a structured questionnaire included the age, sex, birth order, family setting, parent/guardian age, knowledge and attitude of parents about enuresis and the socioeconomic status of the parents using the method recommended by Oyedeji.12 The parents' occupation and highest education attained were scored from 1 (highest) to 5 (lowest). The mean score for both parents gives social class falling within the 1 5 range. Definitions Enuresis was defined as bedwetting at least once a month in a child aged more than 5 years. Primary nocturnal enuresis was defined as present when the patient had never achieved a period of nighttime dryness > 6 consecutive months while secondary nocturnal enuresis was considered present when the patient had experienced a period of nighttime dryness of at least 6 consecutive months.1, 13, 14 Daytime wetting (diurnal enuresis) was defined as unintended voiding of urine occurring during the day.1, 14 Data analysis and presentation Data analysis was by descriptive and inferential statistics using theSPSS for windows software version 11. This was done in two parts:
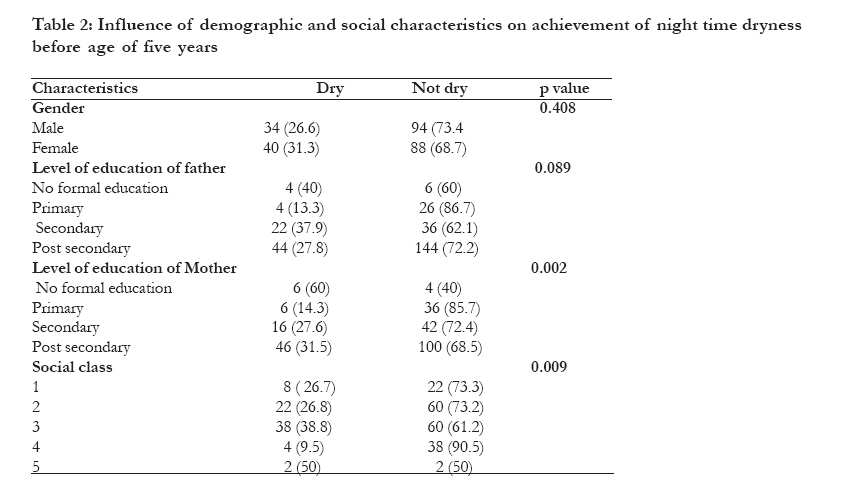
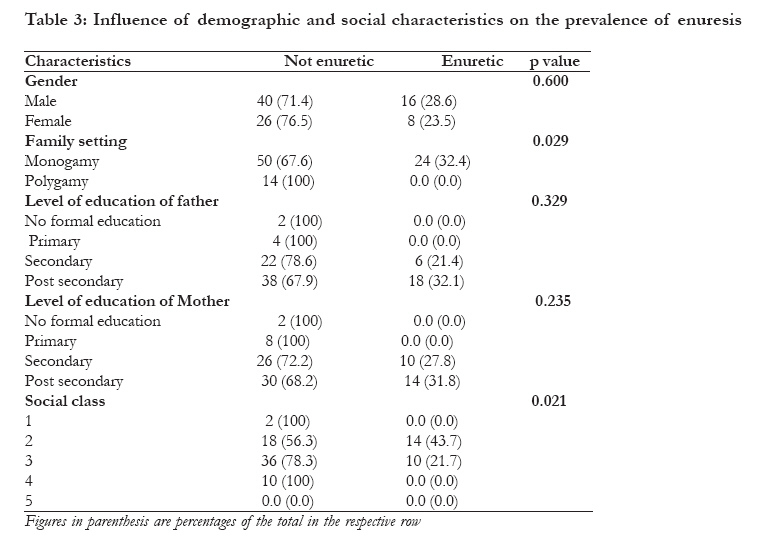
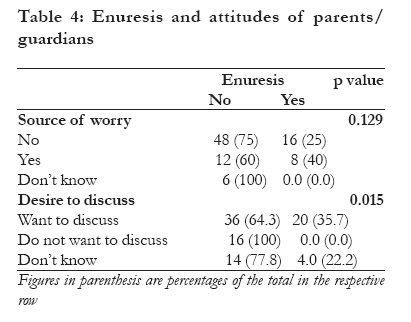
Univariate analyses were carried out for all major variables of interest like demographic, socio-economic and urinary habits. The means, standard deviations (SD) and confidence interval was calculated for continuous variables while ratios and proportions were calculated for categorical variables. Means were compared by the student's t test. Proportions and ratios were compared using the Pearson Chi squared (÷2) test. A p value of less than 0.05 was taken as statistically significant. Results Epidemiological features of the study population A total of 346 children were seen during the study period. Their ages range from 12 168 months while the mean age was 50.1 + 34.3 months. Two hundred and fifty six (74%) children were less than 60 months old while 90 (26%) were 60 months old and above. Sex distribution shows that 184 (53.2 %) children were males while 162 (46.8 %) were females giving a female: male ratio of 1: 1.1. The predominant tribe was Yoruba comprising 83.8 % of the study population. Distribution of the families shows that 32 (9.2 %), 114 (32.9 %), 144 (41.6 %), 52 (15 %) and 4 (1.2 %) were in social class 1, 2, 3, 4 and 5 respectively. Three hundred and six (88.4 %) families were of monogamous setting while 40 (11.6 %) were polygamous (Table 1). Two hundred and eighty four (82.1 %) of the respondents were mothers, 32 (9.2 %) were fathers while 30 (8.7 %) were aunts, sisters or brothers. Their mean age was 397.2 + 84 months. Knowledge and attitude of parents about enuresis All the respondents were aware of enuresis. The age at which parents/guardians expected their children to achieve continence ranges from 12 to 144 months and the mean was 48.2 + 22.7 months. Behavioural disorder was the commonest listed cause of enuresis (45.7 %). Other parents said it was a health problem (9.8 %), psychosocial (6.4 %), familial (0.6 %) and witchcraft (0.6 %). Ninety (26.5 %) of the respondents said it was normal for children to bed wet and another 36 (10.4 %) of the respondents gave other reasons such as excessive play in the afternoon, drinking too much water and parental negligence. Two hundred and eighty (80.9 %) respondents declared that enuresis is not a source of worry to them while 56 (16.2 %) respondents admitted it is a source of worry. Ten (2.9 %) respondents could not say whether it is a source of worry or not. One hundred and seventy eight (51.4 %) of the respondents desire to discuss the problem of enuresis with health workers, 104 (30.1 %) respondents were not interested in discussing while 64 (18.5 %) respondents didn't know whether they were willing to discuss or not. Micturational dryness and prevalence of enuresis Out of the 256 children who were aged less than 60 months, 162 (63.3 %) children had achieved dryness at day time while 74 (28.9 %) children had achieved dryness at night time. The mean ages at achievement of micturational dryness at day time and at night time were 23.1 + 12.5 months (95% CI = 20.8 25.4) and 26.2 + 12.7 months (95% CI = 23.1 29.3) respectively. Even though female children achieved dryness both at day time and at night time earlier than male children, the mean difference was not statistically significant (p=0.12, p=0.64 respectively). By the age of 36 months 86 (51.8 %) children had achieved daytime dryness while only 34 (20.5 %) children had achieved night time dryness (Table 1). Table 2 shows that achievement of day time dryness was statistically significantly related to low maternal education (p= 0.022) and low socioeconomic class (p= 0.009). Out of the 90 children who were more than 60 months old, 20 (22.2 %) children wet only at night, while 4 (4.4 %) children wet both during the day and at night. All the children had primary enuresis. The prevalence of enuresis was higher in males than females (28.6 % vs. 23.5 %) but this was not statistically significant (p = 0.6). Table 3 shows that as the level of education of father and mother increases, there was a corresponding increase in the prevalence of enuresis although these were not statistically significant (p = 0.33, p = 0.24 respectively). The children with enuresis were only from social class 2 and 3 with those in social class 2 having a higher prevalence than those in social class 3 (43.7 % vs. 21.7 %) and this difference was statistically significant (p = 0.021). All the children with enuresis were from monogamous homes while none came from polygamous homes. This difference was also statistically significant (p = 0.029). Table 4 shows that a statistically significant proportion of the mothers expressed desire to discuss enuresis with health workers (p = 0.015) Discussion Majority of children possess the ability to control their bladder at the age of 18 to 24 months and are therefore ready to start toilet training at this age.15 In most countries of the world today, there is a gradual increase in the age at which control is attained.16 The expected age of 48.2 + 22.7 months by parents in this study is higher than that for children from United State of America who are expected to be toilet trained by age of 36 months.17 Also, the achievement of dryness at daytime by only 51.8 % of children aged 36 months is lower than that reported by Robson where by age 36 months, 98 % of children have achieved daytime dryness.6 This may be as a result of the difference in the method of toilet training and other postnatal factors which may affect development of micturational dryness rather than developmental immaturity. The various methods of toilet training in use today were described decades ago. Although less known, assisted toilet training has been used in China, India, Africa, South America, Central America and parts of Europe for centuries before the western methods were described.18 This method starts very early in life with the mother observing for the signs of elimination emanating from the baby. Once these signals are seen by the mother or the carer, the child is placed on the potty to eliminate, while held by the mother or carer. Brazelton in 1962 described child oriented gradual training approach.19 The principle behind this is that the child must exhibit the parameters of toilet readiness. A decade later, Azrin and Foxx20 designed a more rapid and structured behavioural method that is based on the principle of conditioning and imitation. It should be stated that there is no agreement on what is the best training method. DM Mota et al implicated other factors affecting dryness and these include use of disposable diapers even among low social class, mothers life styles such as working away from home and mothers domestic chores delegated to third party.16 This same factors could apply to the Nigeria setting as a result of changing lifestyle and rapid urbanization. In agreement with the findings of a study conducted on children from Pelotas, RS, Brazil, 16 children of mothers with low level of education and from poor homes achieved dryness earlier than those from high social class. This depicts the setting in some African tribes where mothers start to train their children earlier basing their decision on age rather than development. These same cultural context was seen in a descriptive cross-sectional study conducted in the United States which found out that children of African-American race were more strongly associated with toileting success than white children.17 The prevalence of enuresis of 26.7 % in this study is higher than 17.6 % obtained for a rural community in south west Nigeria.5 It is also higher than the prevalence of 8 13 % reported for Asian and European countries.21-23 However, it is closely related to the prevalence of 21.3% among children aged 60 to 192 months in Ehor community, Edo state, Nigeria.24 There were more males than females affected with enuresis though not statistically significant unlike the finding from other studies.21, 25 Socio-economic factors are known to affect the prevalence of enuresis. Several studies indicated that unemployed parents, low educational level and professional status of parents, large family size and low family income are all associated with the development of enuresis.22, 23, 26, 27 These acts as stressors to the child and therefore affect its rate of developmental milestones achievement. The relationship between enuresis and children from high socioeconomic class in this study could not be readily explained. It might be due to the fact that the highly educated and those in high socioeconomic classes are carrier parents who do not have time for an early toilet training of their children. In this study, none of the children with enuresis came from polygamous homes. This may be due to the fact that in Africa, polygamy and extended family has social networks that help in reducing stress Heredity has an influential role in the causation of enuresis.20 Several previous studies reported incidence rates of 40 76 % of a history of enuresis in families of wet children.22, 23, 27 In this study we did not report age of dryness of parents because most could not remember. Even though there is no role for genetics in the treatment of enuresis, family history of age at dryness might be helpful in determining when a child becomes dry. This can be an important clue as to whether reassurance is all that is needed in the way of treatment or further investigations to search for possible underling causes of enuresis. All the parents/guardians were aware about enuresis but only very few correctly identified it as a health problem. This is probably why many of these children never sought medical care. Many parents considered enuresis as a benign condition that is self limiting and therefore need not be treated. This is corroborated by the attitude of parents where majority of them show no worry at all about enuresis. This trend is similar to what is seen in Turkish families who do not have a high level of concern about enuresis.27Despite this believe, about half of the parents/guardians and especially those with enuretic children desire to discuss the problem of enuresis with their health workers. It is therefore important that health workers initiate and enquire from parents about enuresis whenever they are attending to children particularly those with age greater than five years. From our findings, emphasis must be placed on children from polygamous homes and high social class. Once diagnosis of enuresis is made, such a child must be properly evaluated to identify the cause if there is any and then treat. The most important aspect of evaluation is a meticulous history. This can establish the diagnosis, lead to more precise treatment and minimise the need for costly and invasive investigations. Physical examination must be comprehensive. This must include measurement of blood pressure, inspection of external genitalia, palpation of the renal and supra-pubic areas and thorough neurological examination of the lumbo-sacral spine and lower extremities. Of all the laboratory studies, the most important screening test is urinalysis. White Blood Cells (WBC) or bacteria on microscopic urinalysis may suggest urinary tract infection; presence of red blood cell in urine may be associated with urinary obstruction while presence of glucose will suggest diabetes. A random or first morning urine specific gravity greater than 1.020 excludes diabetes insipidus. Where no cause could be identified, the parents and the child must be reassured that it can be successfully managed to remove guilt feelings on the part of the parents and embarrassment to the child and parents. Some of the methods of managing enuresis such as reducing fluid intake with evening meal, taking the child to bathroom to void prior to bed time, waking up the child at interval through the night and prize for the child for every dry night are known locally and can thus be recommended. Study limitations It was difficult to clinically exclude all cases of urinary tract infections especially those with asymptomatic bacteriuria without laboratory test. This could account for the high prevalence of enuresis in the study. Conclusion The percentage of children achieving dryness at age of 36 months is lower than that of their counter part from developed countries. Research is needed to investigate the underlying cause of this apparent delay to dryness. Perhaps there may be need to study the methods of toilet training in this environment and its effect on dryness. The high prevalence of enuresis indicates that it may be a very common problem among children and yet it is not reported. The health workers should make question about enuresis to be a standard part of their history taking particularly for children from polygamous homes and high social class. Acknowledgement We thank all the children and their mothers who spared part of their time to fill our questionnaire. We also thank all the house officers and medical officers who assisted in gathering this information. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11037t2.jpg] [hs11037t4.jpg] [hs11037t3.jpg] [hs11037t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}