 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 252 - 254 Outcomes and Reasons for Dacryocystorhinostomy (DCR) at KCMC, a Tanzanian referral hospital, 2001-2006 *Whitaker JKH, Hall AB, Dhalla KH Department of Ophthalmology, Kilimanjaro Christian Medical Centre, Kilimanjaro, Tanzania *Correspondence author Dr John Whitaker BMBS MRCS Heaton Mersey Medical Centre Didsbury Road, Stockport SK4 3BT, UK Tel: +441614269400 Fax: +441619479689 Email: johnwhitaker@doctors.net.uk Code Number: hs11038 Abstract Background: External dacryocystorhinostomy (DCR) is a surgical intervention aimed to treat blocked nasolacrimal
ducts of almost all causes. To date there is only limited data available from the Sub Saharan African setting.
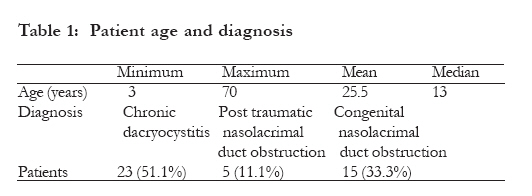
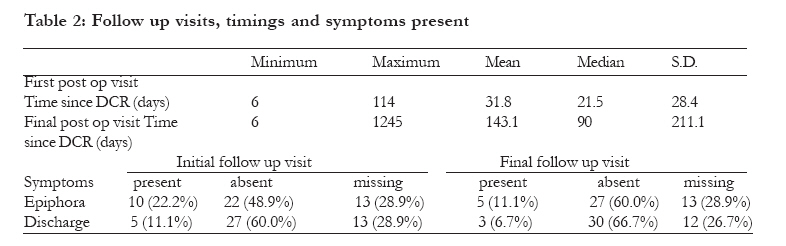
Key words: DCR, Dacryocystorhinostomy, Africa, Outcome Introduction External dacryocystorhinostomy (DCR) is a surgical intervention aimed to treat blocked nasolacrimal ducts of almost all causes. It has been shown to be an effective treatment with over 90% of patients experiencing resolution of symptoms in both western and developing world settings.1-9 There are however limited published data on the efficacy of this intervention in Africa. Our study aimed to provide further information on the indications for and outcomes of external DCR at Kilimanjaro Christian Medical Centre from January 2001 to April 2006 and compare these outcomes with other western and developing world settings. Methods Computerized records of all patients undergoing external DCR operations from January 2003 to April 2006 were systematically searched. Computerization of records was only introduced in January 2003 hence written records of all external DCR patients for the 2 years January 2001 to 2003 were manually searched. All available files were obtained and reviewed. Patient details, diagnosis, operation, hospital stay, outcome at first and final follow up, and total follow up period were all recorded. The results were analysed using Statistical Package for the Social Sciences computer software. Results Thirty two patients were identified from computer records. 30 of these patients' notes were available. 23 patients were identified from the written theatre records. 15 of these patients' notes were available. Reasons for missing notes were not clear but may include miswritten hospital identification number in theatre records. All DCR operations were performed under general anaesthesia. Table 1 shows the patient age range and recorded diagnoses. Table 2 records the patient follow up information. All the patients whose symptoms of epiphora had not resolved after DCR had had a diagnosis of chronic dacryocystitis initially, however this was not statistically significant (p=0.256). Symptoms of discharge completely resolved in 90.9% (30/33) of patients and symptoms of epiphora resolved in 84.4% (27/32) of patients for whom the information was available. Over half the cases 23/45 (51.1%) were children less than 13 years old. 1/15 (6.7%) child had persistent symptoms of epiphora compared to 4/17 (23.5%) adults although this was not statistically significant compared with 3/15 adults (20.0%) (p=0.116). Discussion The number of patients in this retrospective study is small since DCR was not a very common procedure at KCMC during the studied time period. Only 10 per year were performed at KCMC, a major centre for Ophthalmology in East Africa, undertaking a total of 2,454 ophthalmic operations in 2006 alone. The patient follow up period was often short and highly variable. Possible reasons for this may include patients preferring to follow up at local centers or simply failing to return due to cost, transport or time restrictions. More optimistically, perhaps satisfaction with treatment requiring no further intervention kept the patients from returning. Despite these important limitations the study still offers an indication of the success of External DCR in this population. This study revealed a relatively high proportion of DCR's performed on children. 51% of patients were under the age of 13 with 33% of all DCRs having a presumed congenital aetiology. A study from Nepal found only 17.2% of operated cases were on patients under 20 years of age.2 A study from Iran found this figure to be only 12 %.3 A study of Ethiopian patients found that only 10% of operated cases were under the age of 14.4 A presumed aetiology of congenital nasolacrimal duct obstruction is not found commonly as an indication for DCR. A study of 206 consecutive cases of DCR conducted in an Iranian hospital found only 1% were on patients with congenital nasolacrimal duct obstruction.5 A study of 169 consecutive DCR procedures from a US hospital contained only 5% due to presumed congenital nasolacrimal duct obstruction.6 In our retrospective analysis we were not able to establish which patients with presumed congenital nasolacrimal duct obstruction had undergone initial syringing and probing of their nasolacrimal duct. It may be however that late presentation of the patient could deem this procedure less effective and hence the requirement for DCR. Promptness of nasolacrimal probing and intubation because of early presentation and referral could explain why so few patients with congenital nasolacrimal duct obstruction required DCR in a study from the USA .6 Whether expediting referral to KCMC from onset of symptoms or a more rigorous administration of probing and syringing might reduce the need for DCR in our population is unclear. Certainly the results show that outcomes for external DCR were not significantly different for either children or adults and that a clear improvement of symptoms was found in the vast majority of cases. This study provides information on the outcomes of external DCR in the African population. An 84.4% cure rate of epiphora and 90.9% cure rate of discharge is consistent with findings in other developing countries and represents a good outcome.1-9 The largest reported African study of external DCR cases is a prospective review of all cases scheduled at Menelik II Hospital, an Ethiopian tertiary referral centre, from June 2005 until May 2006.4 128 eyes were operated on in the year studied, significantly more than at KCMC, yet with a comparable success rate of 93%. The most common aetiology found was also chronic dacryocystitis, 73% of cases. Their prospective study found patient satisfaction with the scar to be high with 84% rating it as excellent. This aspect was not assessed in our study but external DCR has been shown elsewhere to be an intervention associated with high patient satisfaction even in countries where expectation of medical care is likely higher such as the US.6 Though limited by its retrospective design and small number of cases, this study gives further support to the continued use of External DCR in skilled hands for treatment of blocked nasolacrimal duct of any cause. References
Copyright 2011 - African Health Sciences
The following images related to this document are available:Photo images[hs11038t2.jpg] [hs11038t1.jpg] |
| |||||||||

{kind=link}
{kind=link}