 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 255 - 261 Causes of injuries resulting in a visit to the emergency department of a Provincial General Hospital, Nyanza, western Kenya Ogendi JOK1, *Ayisi JG 2,3 1 School of Public Health & Community Development, Maseno University, Kisumu, Kenya *Correspondence author John G. Ayisi Centre for Global Health Research Kenya Medical Research Institute P.O. Box 1578 Kisumu 40100, Kenya. Tele: (+254)-35-22923/4 E-mail:john.ayisi@yahoo.com JAyisi@kisian.mimcom.net Code Number: hs11039 Abstract Background: There is increasing importance of trauma not only as a major cause of surgical admissions, but also
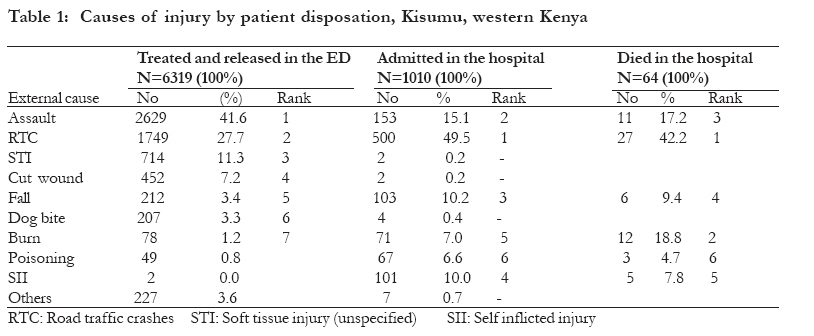
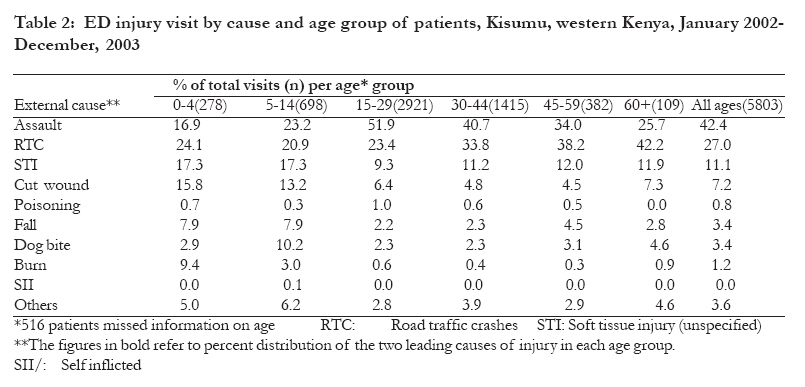
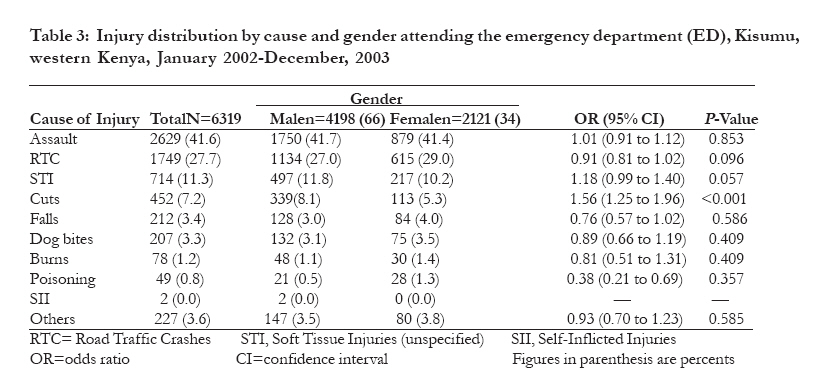
a significant cause of morbidity, mortality and disability. Keywords: Emergency, visit, hospitalization, Kenya, Africa Introduction In sub-Saharan Africa, even though injury ranks third as a major cause of death and permanent disability among the adult population after tuberculosis and HIV/AIDS1, it remains largely a neglected health problem2,3. Kenya, like other developing countries, lacks organized efforts to reduce the burden of injuries. A number of studies in different regions of Kenya have documented the increasing importance of trauma not only as a major cause of surgical admissions, but also a significant cause of morbidity, mortality and serious permanent disability4-8. Important measures of morbidity include rates of hospitalization and duration of stay. The use of emergency department (ED) data provides a cost-effective opportunity but largely an unused source of information for determining injury causes, identifying subgroups of the population at highest risk, associated risk factors and planning for interventions within a health facility catchment area4,9, since up to 50% of patients visiting hospitals are due to injuries10,11. The direct medical costs to hospitals that are already resource constrained and indirect costs of lost productivity on the national economy due to prolonged hospitalization explains need for injury prevention and control. This study sought to provide information on the external causes of injuries requiring ED visit and/or hospitalization and describe the burden due to injuries in a large publicly funded provincial general and referral hospital in Nyanza region, western Kenya. Methods Setting/study facility Nyanza Provincial General Hospital, a large publicly funded hospital with 400 beds, in western Kenya, serves a catchment population of more than 4.4 million people, including the neighbouring areas of Western and Rift Valley provinces. The ED personnel register and document the cause of injury in the medical records for all cases that are admitted and treated for injury routinely on a 24-hour basis, based on the ninth Revision of WHO International Classification of Diseases, Clinical Modification (ICD-9-CM) 12. Selection of cases A retrospective on-site medical record review of injury-related ED visit and/or hospital admissions from 1st January 2002 through 31st December 2003 were reviewed. However due to limited resources, time constraints and its completeness, only data for 2003 were used for in-patient information to compute the length of stay (LOS) and in-hospital deaths, both of which were used as proxies for injury severity. Training of data extractors A data collection manual was prepared by the authors, who specified the aims of the study and items to be collected to three research assistants that were trained on-site, and supervised by them. At the commencement of the study, the authors and field assistants dual-filled 20 records and compared their results to ensure they were collecting information consistently in accordance with data collection manual instructions. Data collection Data for cases that accrued in the study period above were extracted from medical records of both ED and inpatient onto a designed data collection form, and variables included: 1) demographics (age and gender); and 2) cause of injury (both external and nature of injury or clinical manifestation); 3) specialized facility utilization; and 4) if admitted, length of stay and outcome. Supervision of information extraction from ED notes, clinical notes and discharge summaries by the lead, who by then was a master of public health student, at the School of Public Health & Community Development, Maseno University, Kisumu, Kenya. Data Analysis We performed separate analyses for patients treated solely at the ED and those admitted. We used proportions to describe the frequencies by gender and age was grouped as 0-4, 5-14, 15-29, 30-44, 45-59 and 60 and above. Chi-square test and Odds Ratios (ORs) and their 95% confidence intervals were computed to compare proportions. Statistical Package for Social Sciences (SPSS) software for windows version 10.0 was used for data analysis. P< 0.05 was considered statistically significant. This study received ethical approval of the Nyanza Province Hospitals Ethical Review Board, and the hospital administration allowed access to the medical records. Results Causes of Injury Of 15,365 patients who visited the study hospital's ED during the two-year period, 6319 (41%) were injury patients, with a mean age was 25.5 (range 1-95) years. Majority were male 4198/6319 (66%) [95% CI: 65% to 67] and 2121/6319 (34%) (95% CI: 32% to 35%) were female, with a male to female ratio of nearly 2:1. The top three leading causes of injuries visiting ED, and which accounted for 80.6% of hospital visits were: assault (41.6%), road traffic crashes (27.7%) and unspecified soft tissue injuries (11.3%). The other causes included cut-wounds (7.2%), dog bites and falls each contributed just above 3%, while burns and poisoning constituted 1.2 % and 0.8% respectively. Injury-related admissions were analysed only for the year 2003 data. Of the 3253 admitted cases, 1010 (31%) were hospitalized. RTCs were by far the leading cause of hospitalization accounting for nearly 50% of the admissions, and also accounted for 42.2% of all injury deaths, followed by assault (Table1). In contrast, burns though relatively infrequent among injury patients treated at ED and discharged, were most life threatening and accounted for almost a fifth (18.8%) of all recorded injury-related deaths (Table 1). Others 227 3.6 7 0.7 - RTC: Road traffic crashes STI: Soft tissue injury (unspecified) SII: Self inflicted injury comprised 50% (2921/5803), while those aged 30-44 years comprised 25% (1415/5803). The lowest frequency of injuries was found in older people aged 60 and above (1.9%). Table 2 illustrates variations of injury by external cause across the six age groups. Most injuries occurred in the most economically productive age group 15-44 years, who represented 75% (4336/5803) of all injury cases, of whom young adults aged 15-29 years for cuts which occurred more significantly among males than females, 8.1% versus 5.3% (OR=1.56; 95%CI: 1.25 to 1.96; p<0.001) (Table 3). The two most frequent causes of injury in each age group are shown in bold. Overall, assault was the most leading cause of injury in our study hospital accounting for slightly over 50% of the visits in teenagers and young adults aged 15-29 years, and together with RTC were either the first or second leading cause of injury in nearly across all age groups. Soft tissue injury (unspecified), cut wound and fall mostly affected children less than 15 years old. Burns occurred most among the under fives and dog bites was mostly in children 5-14 years. Analysis of causes of injury by gender
among visits to ED showed no gender differences, except
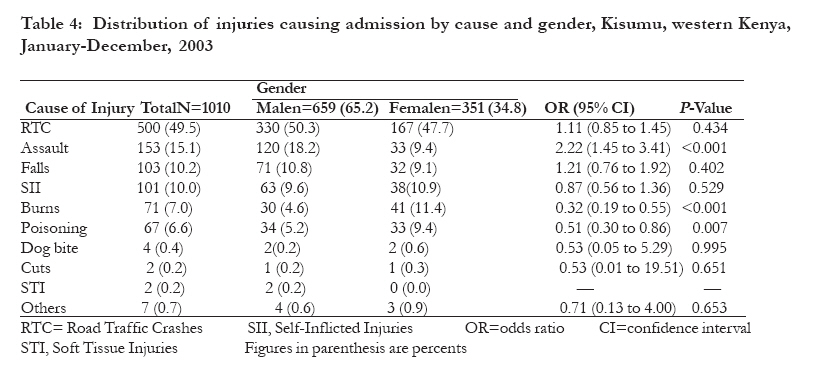
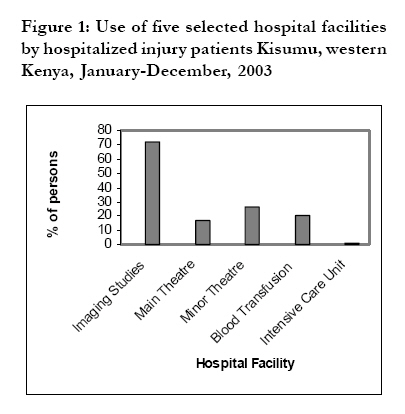
for cuts which occurred more significantly among Observations of injury admissions by gender showed that more males than females were admitted due assault, but the converse was true for burns and poisoning (Table 4) Injury severity Using length of stay (LOS) and inpatient fatality as a proxies for injury severity, we found that there were 1010 hospitalizations with a mean LOS of 8.4 (SD18.9) days, with a median value of 4.0 days (range1-315 days) (Table 5). Of major causes of injuries resulting in hospitalization, falls on average resulted in greater mean LOS (15.6) days in comparison to all other injury causes. For total inpatient days, which take into account both the mean LOS and the frequency of hospitalization, RTC accounted for the largest proportion (46.9%) and contributed to 42.2% of all injury related deaths, with an in-hospital case fatality rate (CFR) of (5.4%). Injury due to burns accounted for 18.8% of all injury related deaths, and had the highest CFR (16.9%), followed by that due to assault (7.2%) (Table 5). Overall, 946 of the 1010 (93.7) admitted patients were discharged home, with only 64 dying, giving an in-patient injury-related fatality rate of 6.3%, two thirds of which were men 42/64, (67.7%). Assessment of the utility of specialized services among the admitted cases showed that nearly three-quarters (72%) required X-rays/imaging services, 43.3% required the use of theatre for surgical procedures, 20.0% required blood transfusion, while 1.0% were admitted to the Intensive Care Unit (ICU) (Figure). Of the 10 patients admitted to ICU, 7 (70%) were due to RTC (data not shown). Discussion The leading cause of injury among ED visits was assault (41.6%) and was the second most important cause of injury-associated admissions and in-patient CFR. These findings are similar to those of a study from another area neighbouring western Kenya that previously reported assault as the leading cause of injury with a rate of 40%4, Ethiopia which borders Kenya to the north, (48.5%)13. RTC were the second leading cause of injury, as well as the leading cause of hospitalization, and accounted for most injury-associated in-hospital stay and deaths, and majority of these RTC (39.1%) involved public transport occupants, consistent with previous studies that have looked at intercity highways that traverse rural areas14,15. Our findings support the view that the road is a dangerous place in Kenya, with RTC being an important cause of mortality, morbidity and disability7 and are estimated to contribute 45-60% of admissions in surgical wards, 75% in the National Spinal Injury Hospital and 3000 death annually14,16,17. This calls for enhanced development of appropriate regulations, legislation, training and enforcement of traffic rules for the protection of general public and loss of assets. Since it has been observed that someone involved in a RTC in Kenya is nine times as likely to die as in the United States18, our study along with other previous studies suggest that management of trauma remains a significant challenge for regional hospitals serving rural Kenya. Like what has been observed elsewhere4,6,14,19-22, results from this study show majority of trauma patients to be predominantly individuals in the economically active age group of 21-60 years with a peak at 21-30 years, depleting the economically productive population, which bears a direct impact on the productivity of individuals, families, communities and the country. Overall, there was no difference in the risk of most injuries by gender in this hospital ED on-site medical records review study, except for assault and cut wounds in which more men were at significantly enhanced risk. This can be attributed to predominance to male domination of most of the hazardous occupations and social activities such as alcohol consumptions4,15,23-25. However, unlike females, we observed fewer cases of burns and poisoning in males. These observed differences by gender call for a well designed study to elucidate risk factors for the specified injuries in the identified high risk groups and provide data than can be used to develop specific community-wide interventions, focusing on particular subpopulations when targeting prevention programmes for selected injuries. Self-inflicted injuries were rarely reported in the study health facility. Suicides may be underestimated, because the taboo around suicide may preclude reporting, however those who reached the hospital were found to be severely injured to require hospitalization. Although Kisumu is on shores of Lake Victoria, the greatest freshwater lake in Africa, we were surprised of no reported cases of drowning/near drowning as causes of injury, suggesting that injuries leading to immediate death may have been underestimated by our study26. Our study also assessed the length of hospital stay and utility of specialized hospital services. In comparison to reports on trauma in other East African hospitals, the mean hospital stay of 8.4 days in our study facility is similar to the previously reported7,17. On average, patients with RTC and burns accounted for more than half of the in-hospital stay and together with assault accounted for more than two thirds of all in-hospital injury related deaths. As observed elsewhere, in the absence of Trauma and Injury Severity Score27, our results agree with others that suggest that LOS can be used as a surrogate in epidemiological studies to identify and characterize patients with severe injuries28. Our findings also show that nearly three quarters (72%) of trauma patients in our study hospital required X-rays and that quite several needed blood transfusion and use of theatre facilities. These have important implications for manpower training and deployment, as well as planning for providing the necessary resources for trauma management in similar publicly funded health institutions that are already facing constrained funding. The overall in-hospital mortality rate of 6.3 % in our study hospital is comparable to other previously reported rates of 6-10%7,29 by studies in a similar environment, but higher than the 3.5% reported in a recent study at Kijabe mission hospital in Kenya's Rift Valley Province17. Unlike our study hospital, the Kijabe study was done in a hospital with a well developed protocol for trauma management including triage, adoption of advanced trauma life support (ATLS)® guidelines in assessment and resuscitation, and early definitive management of injuries30, suggesting that even in the context of limited resources, a team approach combined with appropriate training and adequate equipment can ensure good outcomes for the majority of injury patients. Key points
Study limitations This study only looked at a single hospital and the use of hospital discharge diagnoses has been found to be problematic31, among them being missing data on certain variables, and lack of access to hospitals for patients in many parts of Africa, hence potential for selection bias as patients who did not come to this facility or sought care in other hospitals were not included. We had no direct information on the severity of injuries, hence our use of proxies such as LOS. Conclusion Our study shows that the use of non-fatal ED in conjunction with in-patient injury-related mortality data can provide a foundation for injury research for a better understanding of their causes, imperative for policy, practice and estimation of their economic impact. Acknowledgements To Dr. John Odondi, the Medical Superintendent and Mr. Olongo of records department of Nyanza Provincial General Hospital for their invaluable support throughout the study. M/s Edgar Otumba, Steven Otieno and Albert Mandela for help in data extraction. This study received the financial support of the Maseno University Institute of Research and Postgraduate Studies, and was part an MPH thesis for JOKO. We thank the Director KEMRI for his permission to publish this work. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11039t2.jpg] [hs11039t5.jpg] [hs11039f1.jpg] [hs11039t4.jpg] [hs11039t3.jpg] [hs11039t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}