 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 271 - 278 Uterine Leiomyomata in South Western Nigeria: a clinical study of presentations and management outcome Okogbo F O, *Ezechi OC2, Loto OM3, Ezeobi PM2 1Dept. of Obstetrics & Gynaecology, Irrua Specialist Teaching Hospital, Edo State Nigeria *Correspondence author Dr. Oliver C. Ezechi Sexual and Reproductive Health Research Unit Clinical Sciences Division Nigerian Institute of Medical Research P. O. Box 488 Surulere, Lagos, Nigeria Email: oezechi@yahoo.co.uk Code Number: hs11042 Abstract Background: Uterine leiomyoma is remarkably common, however only a subset of women have their fibroids
clinically detected, symptomatic, or warrant surgical treatment. Its removal is commonly associated with complications. To
prevent or control the occurrence of this complication requires the understanding of the factors associated with the complications.
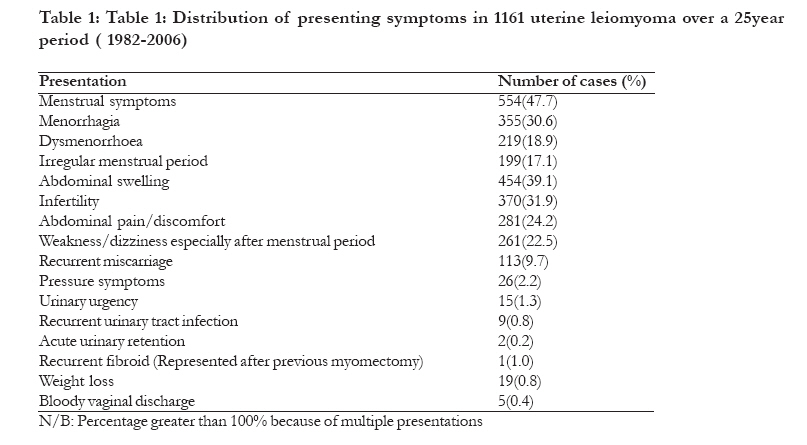
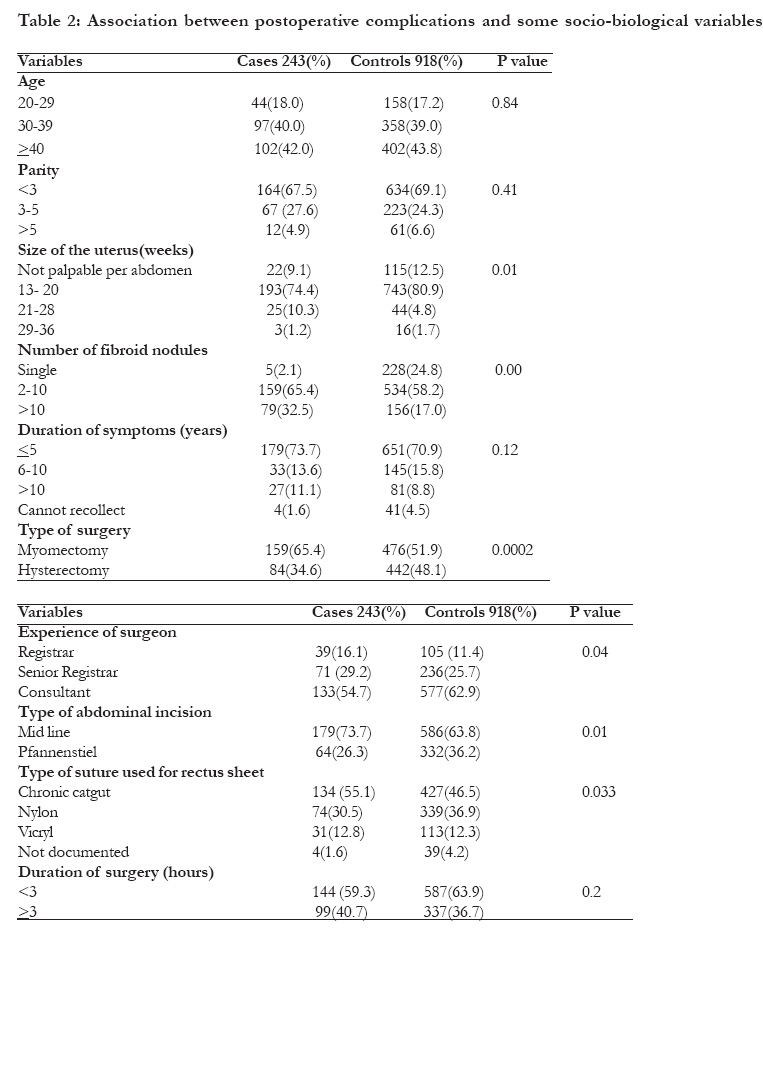
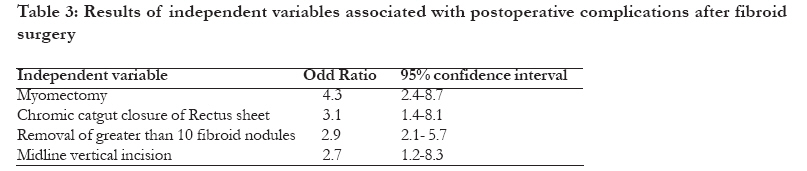
Key words: Uterine fibroid, Leiomyomata Introduction Uterine fibromyoma, more correctly termed leiomyomata but variously referred to as myomas, leiomyofibromas, fibroleiomyomas and myomas, are the commonest pelvic tumour in women 1,2. It is benign, monoclonal tumour of the smooth muscle cells of the myometrium. They are composed of large amounts of extracellular matrix containing collagen, fibronectin, and proteoglycan. Collagen type I and type II are abundant, but the collagen fibrils are formed abnormally and are in disarray, much like the collagen found in Keloid formation12, 3. Uterine leiomyomas are remarkably common, however only a subset of women have their fibroids clinically detected, have associated symptoms, or have surgical treatment. . They occur in 20- 25% of women over the age of 30years, although most are symptomless2, 3, 4,5,6,7. A random sampling of women aged 35 to 49 who were screened by self-report, medical record review, and sonography found that by age 35 the incidence of leiomyomas was 60% among African- American women; the incidence increased to over 80% by age 508. Although the precise cause of leiomyoma is unknown, advances have been made in the understanding of the hormonal factors, genetic factors, growth factors, and molecular biology of these benign tumours1,2,5,6 . It is commoner among the Negroid than the Caucasian race and have been estimated to be 3-9 times more common in Negroes than in Caucasians9, 10, 11. Whether this higher prevalence among the blacks represents a genetic difference, as there is often a family history of fibroids or is perhaps associated with a higher cellular injury or inflammation resulting from an environmental agent, an infection, or hypoxia commoner in the Negroid race which has been proposed as mechanisms for initiation of leiomyoma formation1,4. Uterine leiomyomas are also commoner in nulliparous and relatively infertile women5, 6, 7, 9. Although the presence of leiomyoma is almost never associated with death, leiomyoma may cause morbidity and affect quality of life1, 5. They are mostly symptomless, especially when small and even when of considerable size2, 5,6,10. Most symptomatic patients present with abdominal mass, abdominal discomfort, abnormal uterine bleeding, pressure symptoms and infertility1,2, 5,6,10. The diagnosis of uterine leiomyoma is mainly clinical but ultrasonography is also useful. Often diagnosis of uterine leiomyoma is made incidentally at investigation for other illness 5,6,10. The management of uterine leiomyoma ranges from the expectant, conservative to definite surgery. Myomectomy is the treatment of choice for young women especially those of low parity who are still desirous of children or those who want to maintain their menstrual function5. For older women, hysterectomy is the treatment of choice. Other conservative surgical technique for treatment of fibroid includes hysteroscopic resection of small sub-mucoid fibroid, laser myomectomy, uterine artery embolization and bilateral uterine artery ligation1,2,4, 5,6,7 . The objective of this study is to evaluate the sociodemographic, clinical characteristics and outcome of uterine leiomyoma management in two tertiary hospitals in South Western Nigeria. Methods A retrospective review of all cases of uterine leiomyoma seen and managed surgically at the Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria and Havana Specialist Hospital Lagos, over a 25 year period from January 1st 1982 to December 31st 2006. The hospital numbers of all surgery for uterine fibroid during the study period were obtained from the theatre register. The case records of these patients were thereafter retrieved from the medical record library of these hospitals. Relevant information were extracted from the case records using a data capture form designed specifically for the study. Cases of uterine polyp were included in the analysis only if histologically confirmed as fibroid polyp. Information extracted included sociodemographic, clinical presentation and findings, management modality, operative findings and treatment outcome. The coded data were entered and analyzed using SPSS for windows version 10.0. Frequency tables were computed for all variables separating cases (patients that had postoperative morbidities and mortality) from the controls (uncomplicated cases). Continuous variables were treated as individual elements and then as combined summary measures. Tests of statistical significance were performed based on 95% confidence interval or X2 test with Yate's correction or student's t test as appropriate. As most uterine fibroid are asymptomatic, with only a subset of women having their fibroids clinically detected, have associated symptoms, or have surgical treatment. The data in this study provides information on the latter group. Results Thirteen thousand five hundred and thirty seven women were admitted into the gynaecological ward for various gynaecological conditions during the period under review. One thousand two hundred and fifty nine thousands (9.3%) of the cases were cases of uterine leiomyoma managed surgically. Of the 1259 women with surgically managed fibroid, 92.2 %( 1161) of case records retrieved had adequate information and thus used for the analysis. Demographic characteristics The age of the patients ranged from 20 to 64 with a mean of 39.4± 7.3 years. Age group 30-39 has the highest proportion of cases accounting for 40.2% (467) of all cases seen during the period, with 85.0% (987) of cases aged 30 years and above. There was a rise in the prevalence from 0% below 20 years to a maximum of 40.3% at age group 30-39 and reduction in incidence thereafter from 32.9% (382) at the age range 40-49 to 0.42% (5) at the age group 60 and above. The prevalence at the age groups 20-29 and 50-59 were 15.0 %( 174) and 11.5% (133) respectively. The parity of the women ranged from 0 to 9, with a mean of 1.9± 2.1. Majority (68.7%) of the women were Para 2 or less. The prevalence of fibroid among the women decreased from 32.1% in nulliparous to 0.2% in women of Para 9. Clinical presentation The women presented with varied complaints (see table I). The common complaints were menstrual irregularities (47.7%), abdominal swelling (39.1%), infertility (31.9%), abdominal pain or discomfort (24.2%), weakness/dizziness or syncopal attack after menstrual period (22.5%) and recurrent miscarriages (9.7%). Six hundred and eighty three (58.8%) had at least two symptoms at presentation. Among these women, only 19.2% (223) of cases presented within a year of the onset of symptoms with a mean of 4.9 ±4.3 years. While Six hundred and seven (52.3%) women presented between 1-5 years of the onset of symptoms, others presented at 6-10years (15.3%) and more than 10years (9.4%). Forty five women (3.9%) could not recollect exactly the time of onset of the symptoms. The uterine size at presentation ranged from non-palpable size to size compatible with pregnancy size of 36 weeks with a mean of 15±9.7 weeks uterine size. The uterine size was compatible with 13 to 16 weeks pregnancy size in the majority of cases (51.7%), while in 10.2%, 34.1% and 4.1% of the cases the uterine size was not palpable per abdomen, 17 to 20 weeks and above 20 weeks respectively. Pfannenstiel in 765 (65.9%) and 396 (34.1%) respectively. Myomectomy was the commonest surgical procedure performed in six hundred and thirty five (54.7%) cases. In 71 cases of myomectomy, tuboplasty (68) and polypectomy (3) were performed as an additional procedure. Other surgical procedures performed in the remaining five hundred and twenty six cases were hysterectomy and polypectomy in 509 (43.8%) and 17 (1.5%) cases respectively. Among the 509 patients that had hysterectomy, 29(5.7%) had vaginal hysterectomy and the remaining 447 (87.8%) and 33 (6.4%) had total abdominal hysterectomy (TAH) and subtotal hysterectomy + bilateral salpingoopherectomy (BSO) respectively. Among the cases that had TAH, 234 (52.3%), 194(43.4%) and 12 (2.7%) had TAH alone, TAH + BSO and TAH + unilateral salpingoopherectomy respectively. Pelvic adhesiolysis was performed as an additional surgery in 254(21.9%) cases. The rectus sheet was closed with chromic catgut in 561(48.3%), nylon in 413(35.6%) and vicryl in 144(12.4%) cases. In 43(3.7%) cases the suture used for the closure was not documented. The duration of surgery ranged from 65 to 373 minutes with a mean of 127± 29. In the majority (63.0%) of cases the surgery lasted less than 3 hours. In 27(2.3%) the duration of surgery was not documented. Post-operative complications Postoperative complications occurred in 20.9 %( 243) of the women. The most common complications were postoperative pyrexia (13.5%), blood loss warranting transfusion (12.8%), postoperative anaemia (10.4%), wound infection (8.7%), vault infection (5.1%) and prolonged hospital stay (4.2%). Other complications recorded were wound dehiscence (2.5%), vesicovaginal fistula (0.3%), ureteric injuries (0.3%), bladder injuries (0.6%), and death (0.2%). The association between postoperative complications and some demographic, clinical and operative procedures is shown in table 2. Myomectomy, multiple leiomyoma, uterine size greater than 20 weeks, duration of surgery, surgery by younger surgeons, midline incision and chromic catgut closure of Rectus sheet had significant association with postoperative complications. Discussion Uterine leiomyoma are the most common female reproductive tract tumour, however majority of cases are asymptomatic2, 3, 4,5,6,7. Several studies have documented an increased incidence of uterine leiomyoma in black women and women of African descent4, 9, 10, 11. In this study it accounted for 9.3% of all gynaecological cases over the 25 years period. The finding is similar to 9.8% reported from Lokoja Nigeria, but higher than 7.8% and 8.4% reported from two Nigerian cities of Zaria and Ilesa respectively6,7. As the majority of the uterine fibroids are symptomless, the incidence remains speculative2, 5,6,7,9. In a study that utilized ultrasound scan to screen women for leiomyoma, the prevalence ranged from 4% in women 20 to 30 years of age to 14.5% in women aged 30 to 40 years of age and 33% in women 40 to 60 years of age12. Other studies reported that 5.4 to 77% of women have uterine leiomyomas, depending on the population studied and diagnostic method used4, 12,13. The lower prevalence reported in this study and other studies from Nigeria 5,6,7,10,11 may be as a result of the fact that only women that presented with clinical features of uterine fibroid were screened and also the denominator being the women studied ranged from 20-64 years with a mean of 39.4 years. This finding is similar to the findings from other studies6, 7. This also in keeping with the observation that uterine leiomyoma occurs mostly after puberty 2, 4, 5. In the Caucasians population uterine leiomyoma tend to occur around the age of 30years and commonly causes symptoms between ages 35 and 45 years2, 4, 5 . In this review, majority, 837(72.1%) of the cases occurred in the third and fourth decades of life; in keeping with similar reports from our envirnmen5, 6, 7. The reasons for the high incidence of fibromyoma as from third decades is highly speculative, however female sex hormones have been implicated, particularly stimulation by oestrogen unbalanced by progesterone as a result of persistent anovulation 4,5, 6, 7,9. Nulliparous and primparous women accounted for 44.4% of cases in this review in keeping with observations that leiomyoma are common in the nulliparous or relatively infertile women5, 6, 7,9. Women of Negroid origin tend to develop fibroid at a younger age despite having had children6, 7 . Compare to Caucasians, Negroid women are reported to have a 3-9 times increased incidence of uterine fibroid age for age. This has been attributed to genetic and racial factors4,9 . Attributing symptoms specifically to uterine fibroid is somewhat problematic because of its high incidence in the population, variable clinical presentation and often asymptomatic nature. However evidence largely drawn from uncontrolled studies, showed that uterine fibroid are commonly identified in women who have menorrhagia, pelvic pain, obstructive symptoms, infertility, or recurrent pregnancy loss4. Abnormal uterine bleeding was the commonest presenting symptoms in these women with confirmed uterine fibroid. The incidence of abnormal uterine bleeding of 47.7% in this study is comparable to 52.2% reported in Ilesa, Nigeria6, 7. The cause of the increased uterine bleeding is not always clear but have been variously been attributed to increase surface area and hyperplasia of endometrium, increased vascularity of the uterus, interstitial fibroid nodules that prevent myometrial contraction and functional ovaries often found in association with uterine fibroid9. However a population based study did not find any evidence relating general abnormalities in menstrual cycle length or heaviness to the presence of uterine fibroids4,14 . The number of women in this study reporting infertility as a presenting symptom (31.9%) is higher than 27% reported in Jamaican women15, but similar to 37.1% reported in Lokoja, Nigeria5. However it is much lower than 87.2% reported by Emembolu in Zaria Nigeria7. There is a well-recognized association between uterine fibroid and infertility; however the actual contribution of fibroid in infertility remains controversial. Many of the studies examining relationship between fibroid and infertility are retrospective and non-randomised4. Current evidence suggests that submucosal and intramural fibroids that distort the uterine cavity can impair in vitro fertilization attempts16. The impact of intramural and subserosal fibroids that do not distort the intrauterine cavity is unclear. Despite the lack of clear evidence of their role in preventing conception , submucosal fibroid, intramural fibroids that distort the uterine cavity , fibroids larger than 5cm, and multiple fibroids are often treated in patients with otherwise unexplained infertility17 . However one fact is clear, infertility either voluntary or involuntary is likely to be followed in time with the development of uterine fibroid, and on the other hand, once fibroid have developed, fertility is likely to be decrease or in abeyance18. More important is the frequent association between chronic pelvic inflammatory disease with fibroid as the cause of the infertility2,19. In this study pelvic adhesions warranting adhesiolysis as an additional surgery probably resulting from chronic inflammatory diseases were observed in 21.9% of the patients. The possible role of fibroid in early miscarriage was strengthened by this study. One hundred and thirteen women in this review (9.1%) presented with recurrent miscarriage. However the role of fibroid in early miscarriage has remained controversial. Given the conflicting data 9.1% in this study, 32.3% reported by Emembolu7 and 41% by Buttran and Reiter2 - and the potential observational bias and methodological problems in the studies examining this association, a causal relationship should not be assumed4,20. The size of the fibroid at presentation ranged from non palpable to size compatible with 36 weeks pregnancy size with a mean of 15±9.7 weeks size. The uterine size was compatible with 13 to 16 weeks pregnancy size in the majority of cases (51.7%). The relatively large size of fibroid in this study is probably related to late presentation of the women. The average time before presentation in this study was 5 years. Only 19.2% of the women presented within a year of the onset of symptoms. The preponderance of corporal fibroid in this study is consistent with the report of previous studies. Also multiple fibroid rates of 79.9% in this review is similar to findings from other studies, 5, 6,7,21. Myomectomy was the commonest surgery performed in this study, accounting for 54.7% of cases. The remaining had hysterectomy (43.8%) or polypectomy alone (1.5%). With the large number of women of low parity, presenting with infertility and recurrent miscarriage in this review, myomectomy being the commoner surgical procedure is expected. Myomectomy was often done in patients with associated infertility to improve their fertility potential or when the fibroid is asymptomatic in women who have not completed their family size. Hysterectomy is usually performed in women who had symptomatic fibroids and had completed their family size. The decision to retain the ovaries often depends on how far or close a patient is to menopause5,22 . Two hundred and thirty four (20.2%) women had hysterectomy only while two hundred and seventy five (23.7%) had hysterectomy with either unilateral or bilateral oophorectomy. Vaginal hysterectomy and subtotal hysterectomy was performed in 29(2.5%) and 33 (6.4%) women respectively. Total abdominal hysterectomy is the usual operation for uterine fibroid when indicated except in few cases of associated genital prolapse or where the whole uterus cannot be removed because of pelvic adhesions5,6,7. In this study 29 women had vaginal hysterectomy because of associated genital prolapse and 33 women subtotal hysterectomy because severe pelvic adhesions making it difficult to remove the entire uterus. The postoperative complication ranged from post operative pyrexia (13.5%), blood loss warranting blood transfusion (12.8%), postoperative anaemia (10.4%), wound infection (8.7%), vault infection (5.1%) and prolonged hospital stay (4.2%).Wound dehiscence (2.5%), vesicovaginal fistula (0.3%), ureteric (0.3%) and bladder injuries (0.6%) were other complications recorded. Its heart warming that majority of the patients did not have complications. Post operative pyrexia is a common feature of surgical practice in the tropics. This may be due to wound infection, malaria infection or as a result of oozing of blood into the myomectomy and peritoneal cavity5,6,7,19. However in this study wound infection (8.7%) and vault infection (5.1%) contributed significantly to rate of postoperative pyrexia recorded. Post operative anemia occurred in 10.4% of cases. This may be related in part to blood loss during surgery and possibly preexisting anaemia. The blood transfusion rate of 12.8% in this study was much lower than 59.8% reported by Anate in North central Nigeria5. The lower transfusion rate in this study may be due to the use single myometrial incision when possible and routine application of tourniquet during myomectomy in our institutions. These two technique have been shown to reduce blood loss during myomectomy23. Majority of the patients were discharged home within seven days; however 4.2% stayed beyond seven days. This finding is similar to reports from other studies5, 6, 7. Two deaths were recorded in this study from disseminated intravascular coagulopthy from severe blood loss. Table 2 shows the relationship between postoperative complications and selected variables. It shows that only myomectomy, multiple leiomyoma, uterine fibroid size greater than 20 weeks, duration of surgery, surgery by younger surgeons, midline incision and chromic catgut closure of Rectus sheet were associated with postoperative complications. However after controlling for potential confounders (Table 3), only myomectomy (OR= 4.3), midline vertical incision (OR=2.7), chromic catgut closure of Rectus sheet (OR=3.1) , and removal of greater than 10 fibroid nodules (OR=2.9) retained independent significant association with postoperative complications. Myomectomy is generally associated with higher morbidity than hysterectomy, not only that it is technically more difficult but associated with longer operation time, greater tissue injury and blood loss. Midline vertical incision and use of chromic catgut for rectus sheet are factors know to be associated with increased morbidity post laparotomy. With increased number of fibroid nodes, surgery is likely to be prolonged with increased tissue injury, blood loss and surgeon fatigue. These are factors known to be associated increased postoperative morbidity. Conclusion Uterine fibroid is common in our environment and usually presents with menorrhagia, pelvic pain, recurrent miscarriage and infertility. The surgery may be complicated by post operative pyrexia, blood loss, wound infection and even death. Midline incision, closure of rectus sheet with chromic catgut and myomectomy were associated with postoperative complications in this review To avoid postoperative morbidities associated with surgical management of fibroid, pfannenstiel incision where feasible, use of non absorbable or delayed absorbable sutures and hysterectomy in women who have completed family should be adopted. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11042t2.jpg] [hs11042t1.jpg] [hs11042t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}