 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
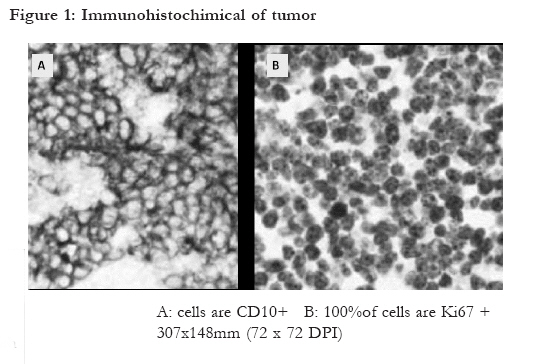
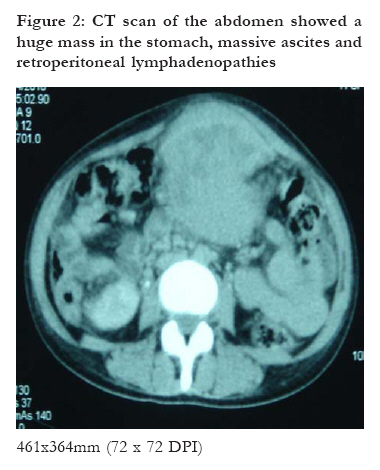
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 288 - 289 Epigastric discomfort during pregnancy presenting as gastric Burkitt lymphoma *Tazi I, Nafil H, Mahmal L Hematology Department, CHU Mohamed VI, Cadi Ayyad University Marrakech, Morocco *Corresponding author Dr. Illias Tazi Hematology Department CHU Mohamed VI Cadi Ayyad University Marrakech Morocco Email: tazi_illias@hotmail.com Code Number: hs11045 Key words: pregnancy, Burkitt lymphoma, epigastric discomfort Case Report A 26 years old female patient, in her first pregnancy with an unremarkable medical and family history, visited another hospital with lack of appetite, early fullness, vomiting, night sweat and easy fatigability of two months duration. Patient was nine months pregnant in her admittance. However, she had not gained any weight within last 4 months despite the pregnancy. The patient linked all other symptoms to her pregnancy. She had to undergo emergency caesarean section due to foetal distress and delivered a viable foetus. She was later transferred to our medical department for further investigations and management. On admission, the patient was experiencing significant abdominal pain, general malaise, nausea, vomiting, and constipation, and was unable to tolerate oral intake. At the time of admission, examination revealed a cachectic, febrile patient with peripheral lymphadenopathy. An abdominal examination revealed a tender mass 6x4 cm in size in the epigastric region with an enlarged liver, which was felt separately from the mass. The spleen was not palpable and free fluid was present in the abdominal cavity. However, there was no pedal edema in any of the four limbs. Right facial paralysis developed one day before admission but there were no other neurological abnormalities detected. Upper gastrointestinal endoscopy demonstrated a tumor originating from the cardia and invading throughout the distal corpus. Histologic examination of gastric biopsies showed a diffuse infiltration of the mucosa by atypical lymphoid cells with a CD20+, CD3- immunophenotype and a diagnosis of "de novo diffuse large B-cell lymphoma" was made initially by the local pathologist. Initial gastric biopsies were reviewed by an hematopathologist and additional immunostains and molecular studies were performed. Immunohistochemistry showed that the lymphoid cells were CD20+, CD5-, CD10+, BCL2- and 100% of tumour cells were Ki67 positive (Fig 1). The patient was diagnosed as gastric Burkitt lymphoma. Appropriate investigations were performed to stage the lymphoma. Computerized tomography of the abdomen showed a huge mass in the stomach, massive ascites and retroperitoneal lymphadenopathies (Fig.2). Tumoral invasion was detected in liver. Laboratory investigations showed haemoglobin of 8 (normal range 1216) g/dL, mean cell volume (MCV) of 83 (8098) fL, white cell count of 7,400/L (4,00010,000/L) and platelets of 280,000/L (150,000300,000/L). The bleeding time and coagulation time were normal. Erythrocyte sedimentation rate was 30 (016) mm/hr and LDH was 1600 (70240) U/L. Liver function, transaminase level and kidney functions were normal. Human immunodeficiency virus serology was negative. The bone marrow contained approximately 80% blast cells with basophilic cytoplasm and vacuolation. Cerebrospinal fluid examination revealed blast cells. The patient was classified as stage IV according to the Murphy classification. After initiating chemotherapy including cyclophosphamide, vincristine and prednisolone, her condition deteriorated rapidly and progressed into fatal tumor lysis syndrome. The patient died afterward. Gastric cancer during pregnancy is extremely rare, with a reported incidence of 0,1%1 and the outcomes have been generally poor2,3. Delay in diagnosis has been attributed to lack of suspicion due to their rarity, presence of non-specific gastrointestinal symptoms in pregnancy and reluctance of physicians to undertake any invasive investigations such as endoscopy due to the risk to pregnancy. Gastric cancers in pregnancy are usually diagnosed in the advanced stages. Most authors have suggested that early diagnosis from early work up is the best way to deal with this condition4. It is important to remember gastric cancer or gastric lymphoma as a differential diagnosis of upper gastrointestinal symptoms that do not resolve with a course of empirical treatment especially in those with family history of cancer. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11045f1.jpg] [hs11045f2.jpg] |
| |||||||||

{kind=link}
{kind=link}