 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 2, April-June, 2011, pp. 296 - 300 Papillary thyroid carcinoma presenting as a lateral neck cyst Al-Ashaa Y 1, Hefny AF1, Joshi S 2, *Abu-Zidan FM3 1Department of Surgery, Al Ain Hospital, UAE *Correspondence author Ashraf Hefny Department of Surgery Al Ain Hospital P O Box 17666 Al-Ain, United Arab Emirates Fax :( +971 3) 7672067 E-mail: ahefny@uaeu.ac.ae Code Number: hs11047 Abstract Background: Solitary lateral cervical cystic mass is an uncommon presentation of papillary thyroid carcinoma.
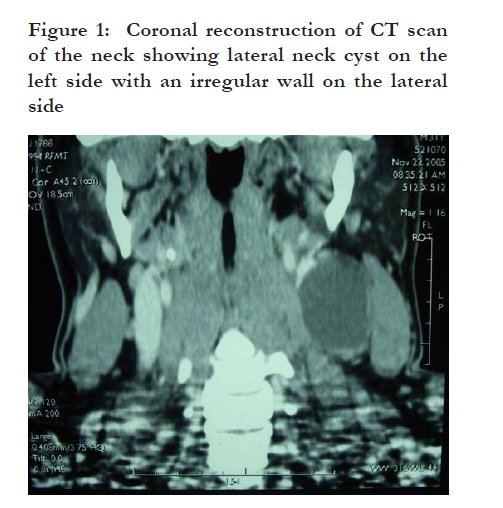
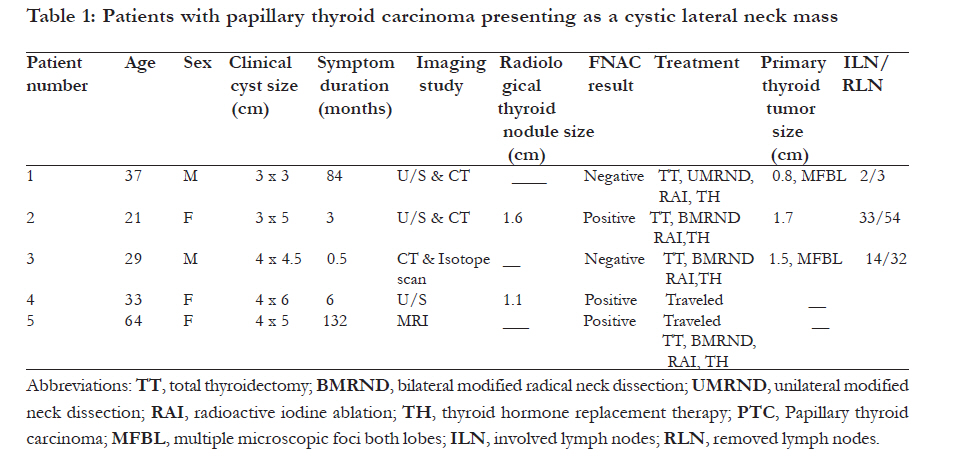
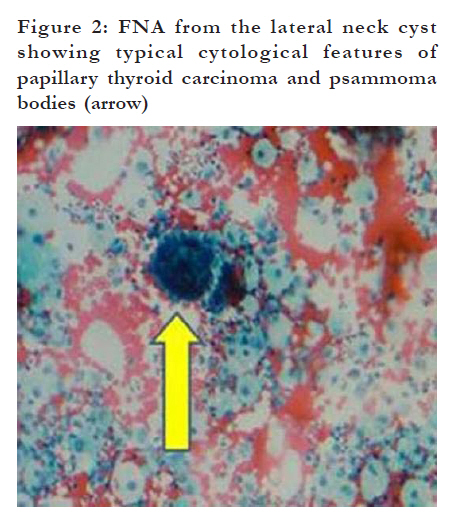
Key words: Cyst, Neck, Thyroid neoplasm. Introduction Cystic neck masses appearing in the anterior or posterior triangles of the neck are usually benign. However, they may occasionally have a sinister origin and should be investigated rigorously.1 Solitary lateral cervical cystic mass is an uncommon presentation of papillary thyroid carcinoma (PTC). If the results of the ultrasound scan and fine needle aspiration cytology (FNAC) are inconclusive, excisional biopsy of the cyst is essential for early diagnosis and management. 2 Herein we report our recent experience in the diagnosis and management of PTC presenting as a lateral neck cyst. Methods Patients who had PTC and presented as a painless lateral neck cyst at the Department of Surgery, Al Ain Hospital, between April 2005 and June 2009 were retrospectively studied. Their clinical features, diagnosis and management were reviewed. During the same period, 26 patients had thyroidectomy for treatment of PTC, three of them had lateral neck PTC cyst (11.5%). The diagnosis of PTC presenting as neck cyst has been confirmed by FNAC or excisional biopsy of the cyst. Materials obtained by FNAC were used to prepare direct smears, cytospin smears, and cell blocks. After the excision of the cyst or thyroidectomy, histopathological examination of formalin fixed paraffin-embedded microscopic slides with Hematoxylin & Eosin (H & E) staining were performed. Thyroglobulin, epithelial membrane antigen, calcitonin and carcinoembryonic antigens were used for immunohistochemical staining. This study has been approved by Al Ain Medical District Human Research Ethics Committee, Al Ain, UAE (Ethical Approval Number: AAMD HREC 09/17). Results Presentation Five patients (2, males, 3 females) were studied. The patients had a median (range) age of 33 (21-64) years. They had a painless slowly growing lateral neck mass of median (range) duration of 6 (0.5-132) months. In one patient, a recurrent lateral neck cyst was developed over 11 years following its primary local excision. In another patient, there was a family history of thyroid cancer, the type of which was unknown. Clinically, the size of the cyst ranged between 3 and 6 cm in diameter. In three patients the mass was located in the supraclavicular area while it was in the suprahyoid region in the other two. No masses were palpable in the thyroid gland. Investigations Ultrasound scan of the neck was performed in three patients. The cysts had heterogeneous echogenicity with no areas of microcalcifications. Multiple enlarged cervical lymph nodes were reported in two patients and increased vascularity in one. Thyroid nodules were detected in two patients. CT scan of the neck has shown that the neck masses contained cystic and solid elements (Fig 1). Thyroid nodule was detected only in one patient. Preoperative thyroid radioisotope scanning was preformed in one patient and it has shown diffuse goiter with general poor uptake. No nodules were detected (Table 1). FNAC of the cystic masses were performed in all patients. Aspirates were haemorrhagic to brownish in colour in all. It has shown PTC in three patients (Fig 2). FNAC was negative for PTC in two patients (true positive 60%, false negative 40%). In one patient, thyroglobulin immunohistochemical staining of FNAC was performed and it was positive. Excisional biopsy of the cystic masses was performed in two patients with negative FNAC. It has shown PTC in both patients. Operations Three patients had total thyroidectomy and modified radical neck dissection. Postoperatively, all the patients had radioisotope scanning and underwent radioactive iodine ablation followed by thyroid hormone replacement therapy. Histological examination of the thyroid gland revealed PTC with multiple bilateral cervical lymph nods involvement in all ofthe three operated patients as indicated in table 1. Follow up Two patients were followed up for 5 years and were completely free of the disease. In one patient who had the operation overseas, a lung metastatic lesion was discovered one year postoperatively and she underwent radioactive iodine ablation therapy for two years. Two patients were lost for follow up. Discussion The most common benign lateral cervical cysts are branchial cleft cysts, dermoid cysts, teratoma, epidermoid cysts, and cystic hygromas. Due to the increasing incidence of oropharyngeal carcinoma, cystic masses of the neck can also be metastases from an oropharyngeal or tonsillar tumour. 3, 4 Rarely, PTC presents as a lateral cystic neck mass without palpable lesion in the thyroid gland. 5 The origin of these cysts is controversial. Some authors think that it represents a malignant transformation of ectopic thyroid tissue. Others think that it represents a secondary metastatic spread from occult thyroid lesion to the lymph node which underwent central liquefaction with cystic formation. 6, 9 Papillary thyroid carcinoma is a slowly growing neoplasm which explains the relatively long duration of the neck masses in our patients with range of (0.5-132) months. One of our patients has a recurrent cystic lesion eleven years after the primary excision of the cyst. Previous history of thyroidectomy or positive family history of thyroid cancer may raise the suspicion of thyroid metastasis. In all of our patients, no masses could be detected by the clinical examination of the thyroid gland which adds to the difficulty of the diagnosis. 10 The long duration of such cysts in young aged patients can lead to incorrect provisional diagnosis of benign cysts. 2 Ultrasound scan has shown cystic lesions with irregular thick wall and solid echogenic components adherent to the wall. Usually it is difficult to differentiate between the cystic metastasis of PTC and branchial cyst depending on ultrasonography.10 In two of our patients, a thyroid nodule has been detected by ultrasound. Computed tomography (CT) scan typically shows cystic masses of irregular thick wall with the presence of intracystic enhanced solid component. 1 In one patient, CT scan of the neck has shown thyroid nodule and multiple bilateral cervical lymphadenopathy. Intravenous iodine containing contrast media during CT scan can interfere with radio active iodine uptake by the thyroid for several weeks. Nevertheless, this effect is transient and is unlikely to be significant when one considers the time frame of using radioactive iodine later on. 11, 12 While ultrasound scan is the best modality for delineating the tumor within the thyroid, CT scan and magnetic resonance imaging (MRI) are better modalities once the tumor has breached the capsule. FNAC is less sensitive in the diagnosis of cystic neck masses compared with solid masses having a false negative rate ranging from 50% to 67%. 13 FNAC was positive for PTC in only three of our patients and the other two patients had negative result (false-negative rate of 40%).The cystic fluid which doesn't have the characteristic opaque yellow colour of typical branchial cyst should raise the suspicion of cystic metastatic PTC.14 The aspirates for cystic metastases of PTC are often red or brown in colour because of thyroglobulin. Thyroglobulin immunohistochemical staining and assay of the aspirate will add to the accuracy of the FNAC in the diagnosis of PTC. 15 Ultrasound guided FNAC that can obtain material from the wall and solid part of the cyst increases the accuracy of FNAC. 14, 16 Excisional biopsy is essential to detect papillary thyroid carcinoma in patients with negative FNAC. 13 If clinical or radiological suspicion of malignancy is present, frozen section analysis of the specimen may help to proceed for a total thyroidectomy with modified radical neck dissection at the same setting. In our patients, the excised cysts had scanty lymphoid tissue possibly presenting lymph nodes remnants. In one of the excised cysts, multiple lymph nodes were attached to its wall showing metastatic PTC. Adequate surgery by removing the cyst, all of the thyroid tissue and accessible involved lymph nodes is essential for better prognosis. 16 Surgical planning should be considered in the light of available expertise. 16 Three of our patients had cyst excision and total thyroidectomy. PTC was found in all thyroidectomy specimens of the operated patients with multiple lymph node metastases. This observation supports the hypothesis that these cysts are metastatic in nature. All patients underwent postoperative radioisotope scanning. It is highly sensitive and specific having high positive predictive value and can identify remnants of thyroid tissue and metastasis. All operated patients had radioactive iodine ablation and thyroid hormone replacement therapy. Currently there are no national guidelines for the management of lateral neck cysts. We recommend that cases presented with unusual neck cyst in adult life should be taken seriously. Thorough history and clinical examination followed by ultrasound and CT scanning of the neck including the thyroid gland are essential. If ultrasound guided FNAC was inconclusive, excisional biopsy is mandatory. The early diagnosis and treatment without prolonged delay is an important factor in decreasing the mortality rate in such patients. 1 Conclusion Our study supports the hypothesis that PTC presenting as a lateral cystic neck mass is actually ametastasis to the cervical lymph nodes. The medical and personal history is usually misleading. High index of suspicion should be adopted when managing unusual neck cysts located in unusual sites in adults. Diagnostic thyroid ultrasound and neck CT scan may display the primary thyroid lesion. This would require total thyroidectomy and modified radical neck dissection. If FNAC guided ultrasound of the cyst is inconclusive, excisional biopsy is essential to rule out malignancy and to avoid the delay in the diagnosis and management. References
Copyright 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11047f1.jpg] [hs11047f2.jpg] [hs11047t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}