 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. S1, Aug, 2011, pp. S40-S45 Antimicrobial susceptibility patterns of E. coli from clinical sources in northeast Ethiopia *Kibret M1, Abera B2 1 Department of Biology, Science College, Bahir Dar University, Bahir Dar, Ethiopia Code Number: hs11056 Abstract Background: Escherichia coli is the leading cause of urinary tract, ear, wound and other infections in humans. Increasing
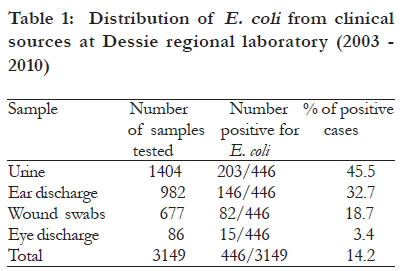
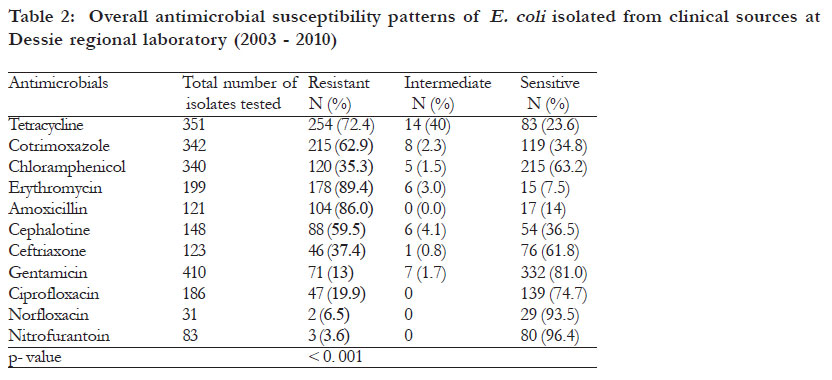
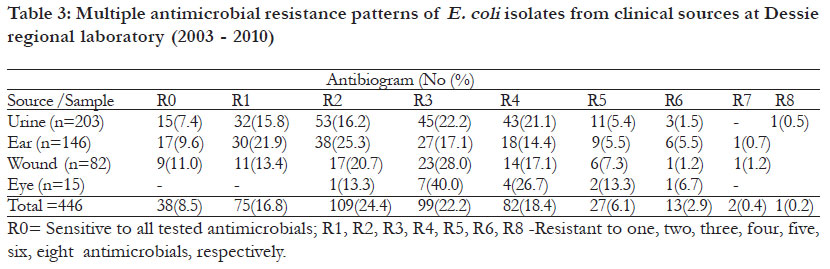
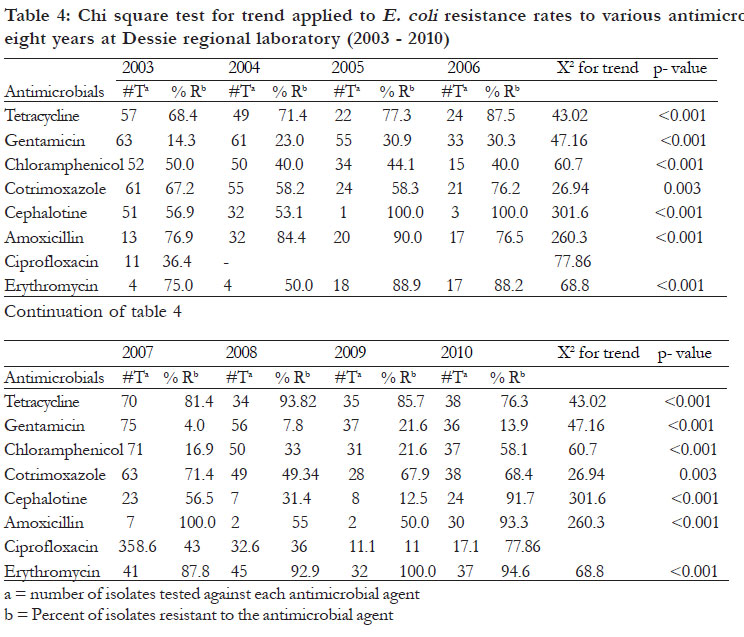
rates of antimicrobial resistance among E. coli is a growing concern worldwide. Key words: E. coli, antimicrobial susceptibility, Ethiopia Introduction Escherichia coli is a common inhabitant of the human and animal gut, but can also be found in water, soil and vegetation. It is the leading pathogen causing urinary tract infections1,2,3 and is among the most common pathogens causing blood stream infections4, wounds, otitis media and other complications in humans5, 6. E. coli is also the most common cause of food and water-borne human diarrhea worldwide and in developing countries, causing many deaths in children under the age of five years7. Antimicrobial resistance in E. coli has been reported worldwide and increasing rates of resistance among E. coli is a growing concern in both developed and developing countries8, 9. A rise in bacterial resistance to antibiotics complicates treatment of infections. In general, up to 95 % of cases with severe symptoms are treated without bacteriological investigation10. Occurrence and susceptibility profiles of E. coli show substantial geographic variations as well as significant differences in various populations and environments11. In Ethiopia, a number of studies have been done on the prevalence and antimicrobial resistance patterns of E. coli from various clinical sources5, 12, 13. The aim of this study was to determine antimicrobial susceptibility of E. coli from clinical sources at Dessie Regional Health Research Laboratory. Methods Study design A retrospective review was done on results of cultures of urine, ear discharge, pus swab from wounds, and eye discharge that had been performed from 2003 - 2010 at Dessie Regional Health Research Laboratory. The sex and age of patients. As well as E. coli isolates and antimicrobial susceptibility data were collected from the registration records using a standard data collection form. Culture and identification The specimens were collected from public and private hospitals and health centers. As the standard operation procedures show, clean-catch midstream morning urine specimens are collected using sterile wide mouth glass containers. Urine samples were plated on Cystine Lactose Electrolyte-Deficient medium (CLED), MacConkey agar and, Blood agar (Oxoid, Basingstoke, UK) using calibrated wire loops and then incubated aerobic atmosphere at 37oC for 24 hours. From positive cultures, uropathogens were identified according to the standard operational procedures as per the standard microbiological methods14. A significant bacterium was considered if urine culture yield < 105 colonyforming unit (CFU/ml. Samples from discharging ears, eye swab, and pus from wound were collected using sterile cotton swabs14. Specimens were inoculated onto 5% Sheep’s blood agar, chocolate agar, mannitol salt agar and MacConkey agar plates (Oxoid Ltd, Basing stoke Hampshire, UK). The plates were incubated at 37oC aerobically and examined after 24 and 48 hours. Antimicrobial susceptibility tests According to the standard operational procedures, antimicrobial susceptibility tests were done on Mueller-Hinton agar (Oxoid, Hampshire, England) using Kirby Bauer disk diffusion method15. The antimicrobial agents tested were: tetracycline (30 μg), nitrofurantoin (300 μg), erythromycin (15 μg), chloramphenicol (30 μg), gentamicin (10 μg), ciprofloxacin (5 μg), cephalotin (30 μg), cotrimoxazole (25 μg), ceftriaxone (30μg), norflaxocin and amoxicillin (10μg) (Oxoid, England). Resistance data were interpreted according to National Committee for Clinical laboratory Standards (NCCLS)16. Reference strains of E. coli ATCC 25922 and S. aureus ATCC 25923 were used for quality control for antimicrobial susceptibility tests16. Statistical analysis The chi-square test was employed to compare the proportion of bacterial isolates with patient sex and age; and comparison of antimicrobial resistances. Pvalue of < 0.05 was considered to indicate statistically significant differences. Ethical consideration Ethical approval was secured from Research Ethics Committee of Bahir Dar University. Permission from Dessie Regional Health Research Laboratory was also obtained. Results Between 2003 and 2010, a total of 3149 samples were analyzed for isolation and identification of bacteria and antimicrobial susceptibility testing. E. coli was isolated from 446 (14.2%) samples. Of these positive cases, the isolation rate of E. coli was the highest in urine samples 203 (45.5%), followed by 146 (32.7%) in ear discharge, 82 (18.7%) in wound swabs and 15 (3.3%) in eye discharge (Table 1). The overall susceptibility patterns of E. coli isolates from various clinical sources is displayed in Table 2. Significantly high resistance rates to erythromycin (89.4%), amoxicillin (86.0%) and tetracycline (72.6%) were documented (p=0. 001). On the other hand, significantly high degree of sensitivity rates to nitrofurantoin (96.4%), norfloxacin (90.6%), gentamicin (79.6%) and ciprofloxacin were detected (p=0. 001). As shown in table 3, the overall rate of multiple drug resistance was 74.6% and only 38 (8.5 %) of the isolates were sensitive to eight antimicrobials tested. Site specific multiple antimicrobial resistance rates were 100%, 76.8%, 75.7% and 67.8% for eye discharge, urine, wound swab and ear discharge samples respectively. The chi-square test for trend shown in table 4 demonstrates increased resistance rates to seven antimicrobials. In 2003, E. coli resistance to tetracycline were 68.4%, to gentamicin 14.3%, chloramphenicol 50.0%, cotrimoxazole 67.2%, cephalotin 56.9%, amoxicillin 76.9% and erythromycin 75.2%. However, in 2010 the resistance rates were tetracycline 76.3 %, gentamicin 13.9%, chloramphenicol 58.1%, cotrimoxazole 68.4%, cephalotin 91.7%, amoxicillin (93.3%) and erythromycin 94.6%, with an increase in rates of 1.2 -34.8%. Discussion Antimicrobial resistance in E. coli has increased worldwide and its susceptibility patterns show substantial geographic variation as well as differences in population and environment17 . The isolation rate of E. coli in the present study was 14.2% and it was commonly isolated from urine samples (45.5%). These findings are in conformity with reports by other researchers13, 18, 19 . In this study, the overall resistance of E. coli to antimicrobials was high. The result is consistent with the findings of previous studies20 . The resistance rates recorded in this study are higher than the results of Khan et al. 6 and lower than the results of Iqbal and Patel 21 and Okonko et al. 22 . High level of resistance in E. coli was reported to tetracycline from a study conducted in Ethiopia23 and to erythromycin from a study done in Slovenia24 . In all clinical samples, E. coli showed high resistance rates of > 80% to erythromycin and amoxicillin and > 60% to tetracycline. The results of this study are in line with the findings of other studies conducted in different parts of the world25, 26 . However, the antimicrobial resistance rates obtained in this study were higher compared to susceptibility patterns reported from previous studies27,28, 29 . E. coli isolates were sensitive to gentamicin, nitrofurantoin, ciprofloxacin and chloramphenicol. Similar studies conducted in Ethiopia30 and Nigeria31 have reported comparable susceptibility rates. High sensitivity to ciprofloxacin and gentamicin and norfloxacin have been recorded from previous studies conducted in Nigeria and India31,32 . In this study, norfloxacin, ciprofloxacin, gentamicin and chloramphenicol were found to be the most effective antimicrobials against E. coli isolates. Furthermore n this study, a high rate of multiple antimicrobial resistance was recorded, which is consistent with the reports of studies done elsewhere21,33 . The chi-square test for trend demonstrated increased resistance rates to all antimicrobials except ciprofloxacin. Increases in rates of resistance to different antimicrobials have been reported from previous studies conducted in different parts of the world20, 33, 34 . Conclusion The results of this study show high rates of antimicrobial resistance to erythromycin, amoxicillin and tetracycline. Nitrofurantoin, norfloxacin gentamicin and ciprofloxacin are considered appropriate for empirical treatment of E. coli in the study area. Periodic monitoring of antimicrobial susceptibility both in the community and hospital settings is recommended. Acknowledgments We thank Mr Fekadu Birru, Head of Dessie Retinal Health Research Laboratory for supporting this research. We also thank all staff of Microbiology department of Dessie Regional Health Research Laboratory for their proper documentation. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11056t4.jpg] [hs11056g1.jpg] [hs11056t2.jpg] [hs11056t1.jpg] [hs11056t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}