 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. S1, Aug, 2011, pp. S100-S104 Socio-demographic determinants of stigma among patients with pulmonary tuberculosis in Lagos, Nigeria *Abioye IA1, Omotayo MO2, Alakija W3 1 Department of Medicine, Lagos State University Teaching Hospital, Ikeja, Lagos.
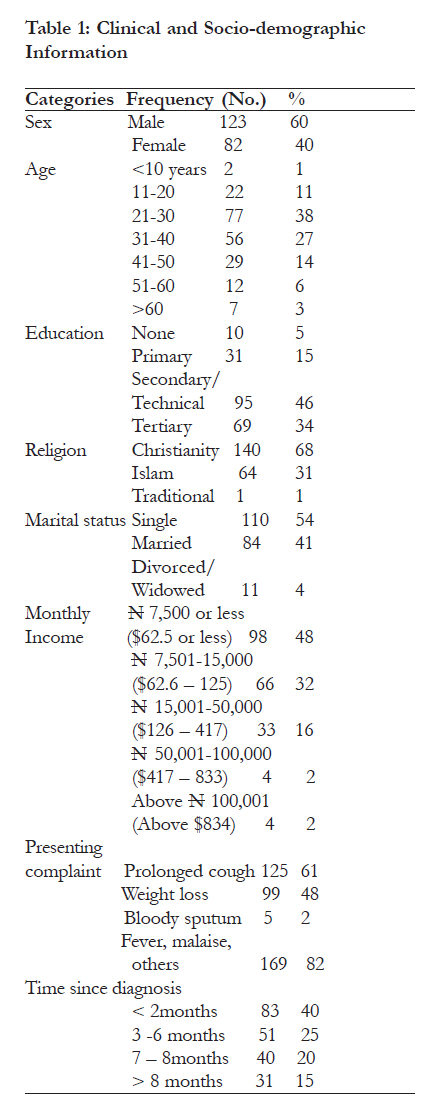
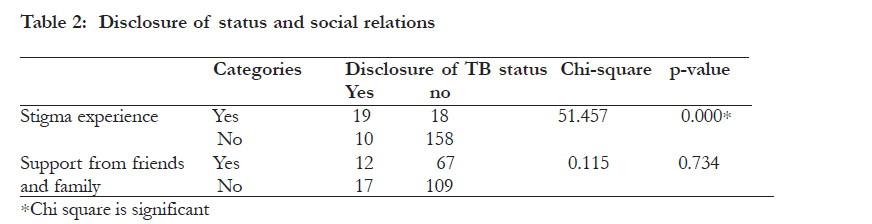
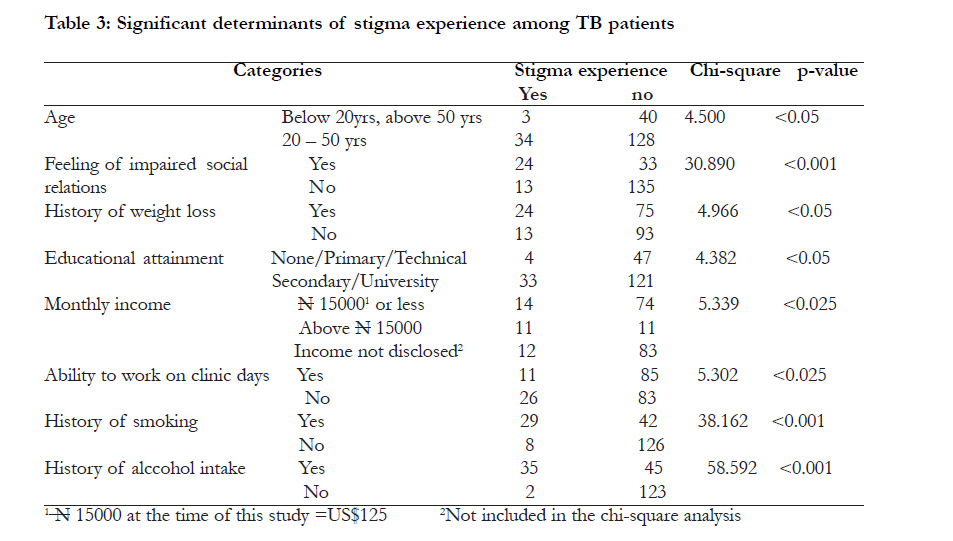
Code Number: hs11065 Abstract Background: Patients living with tuberculosis (TB) experience significant disruption of their social life and are exposed to stigma and discrimination. This situation impacts on treatment adherence by individual patients and on disease control especially in developing nations. Different aetiological propositions have been propounded, including the relationship of tuberculosis with the Acquired Immune Deficiency Syndrome (AIDS). Keywords: Tuberculosis, AIDS, stigma, disclosure, weight loss Introduction Effective control of tuberculosis (TB) has been an arduous international health challenge. The disease infects 8–10 million annually1 and is currently the 7th leading cause of death worldwide2. The disease burden is greatest in Africa and Nigeria ranks fourth among twenty-two high burden countries3. TB is a chronic disease, presenting with prolonged cough and, like Acquired Immune Deficiency Syndrome (AIDS), with marked cachexia as common presenting symptoms. It leads to significant disruption of patients’ life and predisposes patients to stigma and discrimination. Patients experience personal threat, social rejection and social stigma4, with women being worse hit5. Stigma, according to Goffman, is an ‘attribute that is deeply discrediting’ and that reduces the bearer from ‘a whole and usual person to a tainted, discounted one’6. Link and Phelan further define stigma as existing ‘when a person is identified by a label that sets the person apart and links the person to undesirable stereotypes that result in unfair treatment and discrimination’6. Different propositions have been propounded concerning the aetiology of stigma. Fear of being infected is an obvious cause of discrimination6, while scientifically unfounded beliefs about the transmission of the disease have been found to be significant predictors of stigma7. Stigma leads to discrimination, which is the ‘unfair treatment of one person or group usually because of prejudice’ about a specific character they possess8. Stigma and discrimination may affect the extent to which the patient is able to obtain, maintain and complete treatment9. In Ethiopia, stigma was found to be the major cause of non-compliance in the population10. There is increased understanding of the need for emphasis on social and behavioural issues in TB control, for clinical success to be achieved. Most studies on this subject have assessed the common patterns of stigma among TB patients4, 6, 7 , but not the determinants of this social ill. The goal of this study was to evaluate t self-reported stigma experience among TB patients in Lagos, as well as examine its socio-demographic determinants. Methods The study locations were the Chest Clinics of the Lagos State University Teaching Hospital (LASUTH), Ikeja and the Mainland Hospital (formerly Infectious Disease Hospital [IDH]), Yaba. Both are referral centres for tuberculosis care in Lagos, owned by the state government. This was a descriptive crosssectional study, conducted in July 2008, recruiting all patients who had commenced treatment for up to a week. Data collection was quantitative, with the aid of 205 pre-tested self-administered questionnaires. Nineteen questions concerning the clinical history, socio-demographic variables and patient-reported experience of stigma were employed for this study. Patients with limited literacy skills were guided. Analysis was done using the Statistical Package for the Social Sciences (SPSS, version 12.0; SPSS Inc. 2003). The results were presented in texts and in tables. Bivariate analysis of the relationships between stigma experience and socio-demographic variables was also done using Chi square tests and significance was set at p value <0.05. Currencies are quoted in naira, conversion equivalence in US dollars at the prevailing rate at the time of the study (US$1=N120). Ethical approval for the study was obtained from the administration of the hospitals and verbally from patients before recruitment for the study. Results Clinical and socio-demographic information Of the 205 patients recruited, 102 wee from LASUTH and 103 from IDH. The majority of the patients were male (123; 60%), with 82 females (40%). The mean age was 32.9 years (±12.3). Most patients in the study had attained secondary education or higher (81%). Above half of the study population were not married (Table 1). In both centres, loss of weight was a very common presenting symptom among the patients (51%- LASUTH; 56%- IDH). Prolonged cough, the cardinal symptom of tuberculosis, was seen in 61% of the study population. Most patients were diagnosed with TB less than 2 months prior to the study (Table 1). A sizeable proportion of patients (98; 48%) earned below the minimum statutory wage of N7500 ($62.5) as recommended by the national government. TB and social relations About 72% of respondents [147] believed having TB had adversely affected social relationships in their daily life. Of these, TB affected relations with patients’ spouses (27.5%), family (38.5%), friends (30.5%) and co-workers (27.5%) and this was not mutually exclusive. Only 81 patients [39.5%] acknowledged enjoying support from family or friends. Thirty-five percent reported reduced attendance of parties and social engagements, and 24% (49) reported significantly dwindled participation in recreation and sports. Of the 71 patients who had a current or prior history of smoking, 42% discontinued smoking on account of TB. Only three percent persisted despite TB infection. Eighty respondents reported a history of alcohol intake, and 41% of them discontinued on account of TB. However, 9% persisted in the intake of alcohol. TB and stigma Thirty-seven patients (18%) reported a previous experience suggestive of stigma or discrimination. Stigma experience was significantly determined by disclosure of TB status to friends and colleagues. Disclosure of TB status did not significantly determine whether or not patients obtained support from family and friends (Table 2). Patients presenting with history of weight loss,
previous smoking or alcohol history were more likely
to experience stigma. Furthermore, stigma
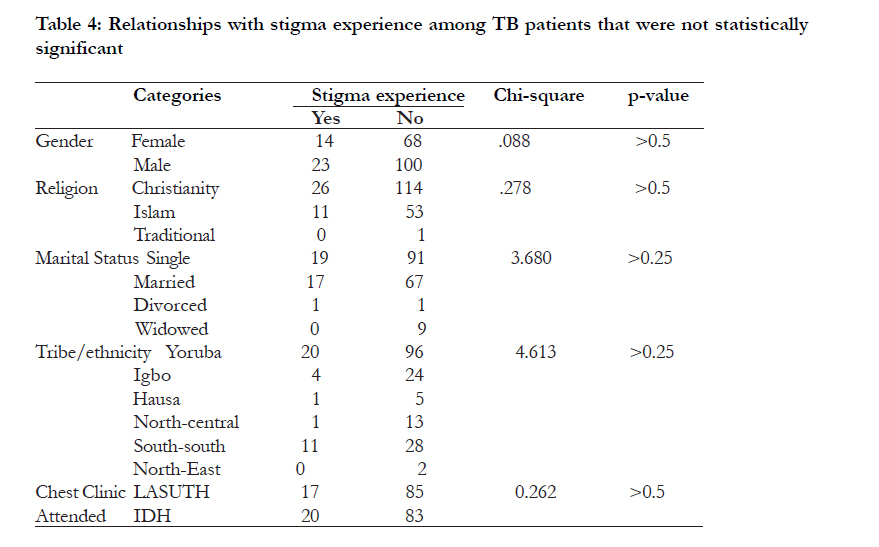
experience was more likely among patients who did
not attain secondary education or whose monthly income was On the contrary, stigma experience was not also not significantly determined by the centre at significantly determined by patient’s sex, religion, which the patient was receiving care (Table 4). marital status or ethnic group. Stigma experience was also not significantly determined by the centre at which the patient was receiving care (Table 4). Discussion Stigma faced by TB patienss is vague and not easily assessed11.Weight loss is a common presenting feature to TB and HIV/AIDS, making it possible for people to conflate both diseases12. Up to 48% of patients presented with weight loss in this stud. This was less than the 73% obtained by Odusanya et al in their study of patients in LASUTH in 200413. In the current study, weight loss was found to be a significant determinant of stigma experience. Studies in Thailand using focus groups among health centre staff, TB patients with or without HIV and HIV patients observed that the increased awareness of HIV/AIDS may be a cause of delays in presenting in the clinic for TB treatment.14 Similar observations were made by investigators in London studying African patients.15 More so, pulmonary tuberculosis is regarded by the World Health Organisation (WHO) as an AIDS-indicator condition.16 This complicated relationship between HIV/AIDS and TB exposes TB patients to stigma. Further, TB patients with more severe symptoms have been reported in Thailand to have experienced greater stigma.12 Most patients understand TB through the medical model and perceive themselves as disease vectors17. In our study, TB was observed as affecting relations with patients’ spouses and their family, as well as with friends and co-workers. Many patients did not disclose their TB status, in anticipation of stigma experience, which they believed to be a corollary of disclosure. Unfortunately, most of those who disclosed were stigmatised. The London study reported actual stigma experiences to be rare, although patients felt stigmatised by the diagnosis itself15. ‘External’ or ‘enacted’ stigma is rooted mainly in fear and judgment of what is different, leading to blame, distancing, and discrimination. ‘Internal stigma’ -also described as felt, imagined, or self stigma - is the product of the internalization of shame, blame, hopelessness, guilt, and fear of discrimination.18 One U.S. study found that internal stigma contributes significantly to levels of depression, anxiety, and hopelessness in people living with HIV18. These may lead to diagnostic and treatment delays as well as noncompliance to treatment schedule, treatment failures and, possibly, drug resistance. Stigma experience was more common among patients in the working age groups [20 – 50years], on lower rungs of the socioeconomic ladder, with limited education and those who miss work due to clinic attendance. In the London study, experience of TB in a known person was found to mitigate stigma.14 Patients’ present or previous habits, especially those with a possible social impact, like smoking and alcohol consumption also affected their stigma experience. Conclusion The self-reported experience of stigma among TB patients in this study was significant. Weight loss, low socio-economic status, current or previous smoking or alcohol consumption and disclosure of TB status were identified as significant socio-demographic determinants of stigma among TB patients. Patients’ work conditions may also have an impact on stigma experience. Recommendations Health workers should pay closer attention to counselling patients who face the risk of stigma. The significance of disclosure should be discussed carefully with them. Local health agencies, as an extension of direct observation, may create support groups and forums for patients to share experiences. This is a practical way to mollify the stigma experience of patients, this may improve treatment adherence and contribute to disease control. Further research is required to explore the relationship between weight loss and stigma experience among tuberculosis patients. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11065t1.jpg] [hs11065t3.jpg] [hs11065t2.jpg] [hs11065t4.jpg] [hs11065f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}