 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
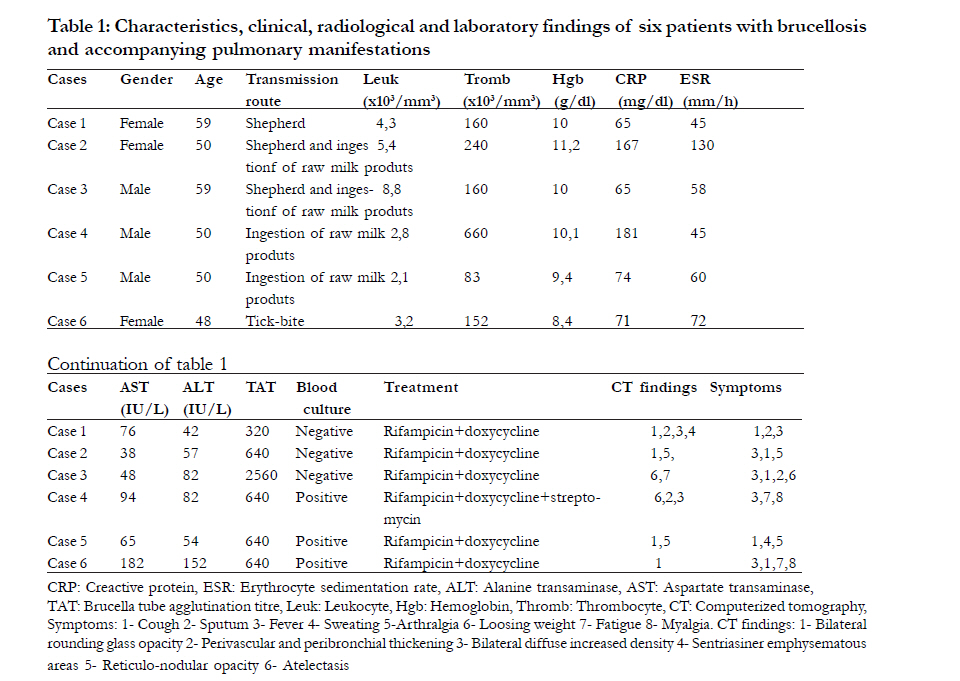
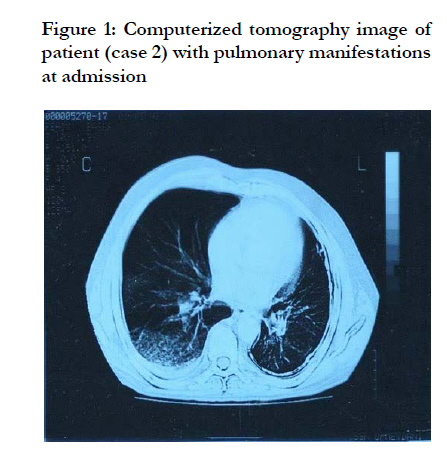
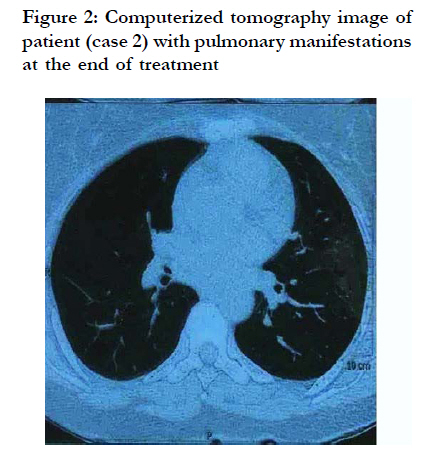
African Health Sciences, Vol. 11, No. S1, Aug, 2011, pp. S112-S116 Pulmonary involvement of Brucellosis: a report of six cases Simsek F, Yildirmak MT, *Gedik H, Kantürk A, Iris EN Department of Infectious Diseases and Clinical Microbiology, Ministry of Health, Okmeydaný Training and Research Hospital, Istanbul, Turkey Code Number: hs11067 Abstract Background: Pulmonary involvement of brucellosis rarely occurs due to inhalation of infected aerosol or hematogenous overspreading. Keywords: Brucellosis, pulmonary, manifestations Introduction Brucellosis is a zoonotic disease that occurs by contact with infected meat or the placenta of infected animals such as cattle, goats, camels, dogs, and pigs’, or ingestion of unpasteurized milk or cheese; or by inhaling airborne agents, and rarely by transplantation and sexual course. Symptoms include weakness, fatigue, malaise, body aches, depression and anorexia1-4 . Signs and symptoms as well as the tube agglutination method, which tests for anti-Opolysaccharide antibody that titers of 1:160 or higher, are diagnostic5. Pulmonary involvement of brucellosis rarely occurs due to inhalation of infected aerosol or hematogenous overspreading. Cough, mucopurulent sputum and flue-like symptoms are the most relevant symptoms in pulmonary involvement of brucellosis10. Acute bronchitis, or bronchopneumonia are diagnostic aspects with radiological findings such as reticulonodular infiltration, diffuse glass round opacitiy, abscess, hilar lmyphadenopathy and pleural effusion with computerized tomography (CT) imaging of lung5. This study aimed to reveal the pulmonary manifestations of brucellosis that occur rarely in Brucella infections in the context of six cases in this report. Methods Between 1998 and 2008, 82 patients diagnosed with brucellosis were treated and followed up at the department of infectious diseases and clinical microbiology, Ministry of Health Okmeydani Training and Research Hospital, a tertiary hospital with 1,200-bed capacity. Among these 82 patients we identified six brucellosis cases with pulmonary manifestations. Clinical, radiological and laboratory findings of these six patients were evaluated, retrospectively. The diagnosis of brucellosis was based upon evidence of contact with animals known to harbour the organism, or a history of ingestion of raw unpasteurized milk or its products and signs and symptoms consistent with brucellosis as described previously. The diagnosis was confirmed by a positive blood culture and/or a four-fold increase in titres, or a single serum tube agglutination test titre of 1:160 or more using Brucella abortus 99 antigen (manufactured by Pendik Veterinary Control andResearch Institute, Ýstanbul, Turkey). Blood culture was implemented using manufactured bottle of Becton Dickinson (BD) Bactec automated system (New Jersey, USA). Patients with respiratory symptoms were examined with radiography of the chest and CT at the beginning and the end of treatment. In addition, sputum was examined with Gram and Ehrlich Ziehl Neelsen (EZN, acid-fast) stains and inoculated into aerobic and Loewenstein-Jensen medium (Merck Schuchardt OHG, Germany) and MGIT (Becton Dickinson, Sparks, USA). Pleural fluid aspirates were collected and sent for culture and serological examinations except for three cases, from which sufficient amounts of aspirate could not be obtained. The Mantoux test (purified protein derivative) was administered to all cases. Complete blood count and erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) level with tests of liver and renal functions were carried out on all cases. Both drugs including doxycycline in a dose of 200 mg/24-h and rifampicin 600 mg/24-h were given to all cases for six weeks. Only one patient (case 4) was treated with combination of doxycycline and rifampicin for six weeks and streptomycin 1 gr/ 24-h (for two weeks). Results Six patients with pulmonary manifestations were evaluated. Patients’ (n=6) age ranged from 48 to 59 years and they showed equal gender distribution (Table-1). Possible transmission route for patients were reported as shepherd (cases1,2,3), ingestion of raw milk or products (case 2,3,4,5), and tick-bite (case 6). Crimean-Congo Hemorrhagic fever was eliminated in that patient (case 6) with serologic test. Cases 2 and 3 were married and occupied with livestock. All patients presented with fever and cough. The duration of these symptoms varied from 3weeks to 3months (mean of 7weeks). Other symptoms were expectoration in two (cases 1,3) and sweating in one (case 5), arthralgia in two (cases 2,5), loosing weight in one (Case 3), fatigue and malaise in two (case 4,6). Leukopenia (< 4500 / mm3) was in three (cases 4,5,6) and thrombocytopenia (< 150000 / mm3) was in two (Cases 4,5) and hemoglobin values ranged between 8,4 and11,2 gr/dl, CRP levels ranged between 65-181 mg/dl, alanine transaminase (ALT) values were higher than normal levels (42 IU/ml) in all patients except case 2 and aspartate transaminase values were higher than upper of normal range (40 IU/ml) at admission for all patients. Physical examination of the chest was normal in cases 1,4,5,6; and there were and crepitations in cases 2,3. Radiological examination showed pneumonic patches and consolidation in two (cases 1,4), bilateral glass round opacity in four (cases 1,2,5,6), perivascular and peribronchial thickness increase in two (cases 1,4), pleural effusion in two (cases 3,4), sentri-acinar emphysematous images in case 1, and athelectasis in case 3 (Figure-1). In all cases, the serological examination for Brucella revealed elevated titres in the agglutination test between 1/320 and 1/2560. Culture grew Brucella spp. from the blood of three patients (cases 4,5,6). Sputum cultures grew only commensals. All patients responded to treatment within seven to 10 days and were treated for six weeks except for case 4 for eight weeks due to hepato-splenic brucellosis. The CRP levels and control CT images of all patients were normal at the end of treatment (Figure-2). Discussions Brucellosis is an endemic disease in Turkey, especially in certain cities where livestock is mostly kept. The disease is encountered throughout the world but is hyperendemic especially in the Mediterranean basin where Turkey is located and the Arabian peninsula, India, Mexico, middle and South American continent5,7 ,8. According to the Ministry of Health in Turkey, the number of brucellosis cases were reported as 37 cases (0,17/100.000) in 1970 when official notification was not executed appropriately, 1,177 cases (2,34/100.000) in 1985, 5003 cases (8,69/100.000) in 1990, 8,506 cases (13,46/100.000) in 1995, 10742 cases (15,83/100.000) in 2000, 14644 cases (20,32/100.000) in 2005, 11,649 cases (16,16/ 100.000) in 2007 and 9,324 cases (12,93/100.000) in 200916. All cases had history of exposure to infected animals or their products. Ingestion of raw milk or its products, animal husbandry, and laboratorial exposure are essential risk factors for brucellosis. Animal husbandry and ingestion of raw milk and its products were reported in five of six cases in this study, except for one patient who had described only tick- bite for a possible transmission route. Patients with unknown transmission route history are rarely presented2,3. Due to the fact that Brucella can invade any tissue in the body and it is endemic in Turkey, it should be considered in differential diagnosis of prolonged symptoms including fever. It seldom involves the lungs, but transmission by air is seen especially in slaughterhouse workers and laboratory staff. It was cited that pulmonary involvement of brucellosis is seen in 0,6 to 16 percent of all brucellosis cases10-12,17. Pfischner et al revealed that 37 of 228 patients (16%) with brucellosis complained of dry non-productive cough on admission, 24 (11%) had moderate sputum production without hemoptysis and eight (4%) complained of chest pain of an ill-defined type which was not pleuretic in nature21. Buchanan and his colleagues reported that 23% of 160 abattoir-associated brucellosis patients complained of cough but radiological examinations of the chest were normal22. Pure pneumonic infiltration seldom occurs in brucellosis13. Brucella could be seen in Gram preparation of sputum or cultivated from sputum culture rarely19,20. In our study, it was not isolated from sputums of the patients. It was cited that Brucella could be isolated from blood culture between 1580%5. It was isolated from blood cultures of three patients in our study. The pleural fluid, a common feature of pulmonary brucellosis, is characterised as lymphocytic pleocytosis, high protein concentration, increased adenosin deaminase level, and cultivation of B. melitensis17,19. It was isolated from pleural effusion in studies conducted in Balkan peninsula12,20. But thoracentesis was not executed in three of our cases with pleural effusion due to insufficient amount of pleural fluid. Different chest radiographic abnormalities were revealed, including soft miliary mottling, parenchymal nodules, consolidation, chronic diffuse changes, hilar or paratracheal lymphadenopathy and pneumothorax5,10,11. Soft miliary mottling and pneumothorax have been described in the study of Patel et al. The high incidence of lung abnormalities was most probably due to the chronicity of the disease in that study18 . In a study of Hatipoðlu et al, 11 of 100 brucellosis patients were reported with pulmonary manifestations such as nodules, lobar pneumonia, paratracheal lymphadenopathy and pleural effusion14. Pneumonia due to B.melitensis was reported from Turkey as well15. Lubani et al. presented that nine cases with pulmonary symptoms and abnormal signs in the chest due to brucellosis and pulmonary manifestations, recovered with standard therapy without any relapse10. Lubani et al. also reported that in the last six years 1,100 child patients were diagnosed with brucellosis, of whom 51 (4,6%) had the symptom cough and among them four (0,4%) had pulmonary brucellosis10. Of our cases, 7% had pulmonary manifestations such as reticulonodular and pneumonic infiltrations and pleural effusion in CT images. Aside from inhalation, bacteremia could cause pulmonary involvement which could exhibit pulmonary signs and symptoms. The incidence of pulmonary involvement of brucellosis is therefore very low and likely to be asymptomatic. The pathophysiology of pulmonary brucellosis is unknown. The role of aerosol inhalation is not clear as most of our patients had ingested raw milk or its products. The most probable pathophysiology is bacteremia as Brucella spp. are widely distributed through the bloodstream to various organs including lungs5,23. Brucellae that are not killed by polymorphonuclear leukocytes are ingested by macrophages, where they become localized within organs of the reticuloendothelial system (i.e. liver, spleen, bone marrow) and multiply in macrophages and monocytes24. Probably it needs the reticuloendothelial organs to multiply and also the lung does not contain any reticuloendothelial tissue, so primary pulmonary brucellosis is very rare and occurs due to distribution through the bloodstream and invading macrophages. Except for laboratory staff, airborne transmission could not be considered as another probable transmission route for patients who are shepherd and consume raw milk or its products. Pulmonary brucellosis could be mistaken for tuberculosis and sarcoidosis, so patients with brucellosis and pulmonary manifestations should be examined for tuberculosis with EZN stain of sputum and sputum culture for tuberculosis such as Loewenstein-Jensen, MGIT etc. as in our study and also for sarcoidosis5,23. Although there are no reported cases of patients with both pulmonary brucellosis and pulmonary tuberculosis, this possibility should be kept in mind. Bihilar lymphadenopathy at stage 1 and 2, bilateral pulmonary infiltrates are diagnostic findings of sarcoidosis in chest X-ray so those are not seen in our patients and subsequent to brucellosis therapy CT findings had disappeared25. Treatment of brucellosis is by administration of doxycycline in a dose of 200 mg/24-h combined with rifampicin 600 mg/24-h for six weeks or doxycycline in a dose of 200 mg/24-h for six weeks combined with rifampicin 600 mg/24-h for six weeks and streptomycin 1 gr/24-h for two weeks. In our study the patients were treated with doxycycline plus rifampicin for six weeks, except for one patient whose treatment was extended to two months due to hepatosplenic brucellosis. Improvement was seen in a few days after initiation of treatment in our patients. Response to treatment should be evaluated with clinical recovery and decrease in CRP level since antibody titers decrease very slowly or stay high for many months. All cases recovered clinically and radiologically at the end of treatment in our study. Conclusion Brucellosis, which continues to emerge as a zoonotic disease in Turkey and other countries, should be considered in unusal clinical presentations, such as pulmonary involvement without accompanying symptoms like fever, arthralgia or fatigue. Pulmonary involvement of brucellosis has good prognosis with combined antimicrobial therapy. Acknowledgement We certify that there is no conflict of interest with any financial organization regarding the subject discussed in the manuscript. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11067t1.jpg] [hs11067t3.jpg] [hs11067f2.jpg] [hs11067t2.jpg] [hs11067f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}