 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
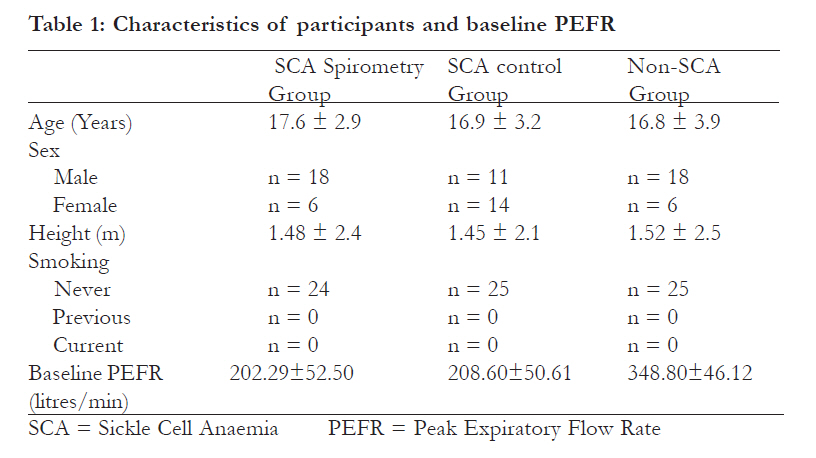
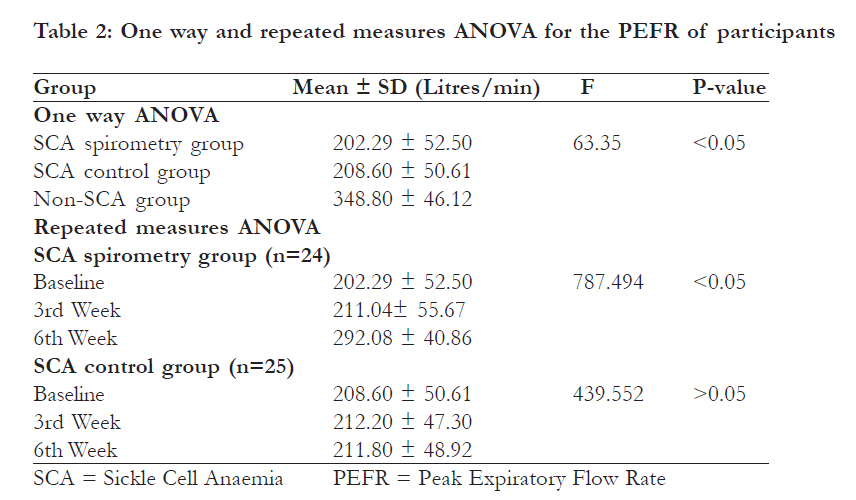
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 303-308 Non Communicable Diseases: Local incentive spirometry improves peak expiratory flow rate in teenage sickle cell anaemia patients: a randomized pilot trial *Adeniyi AF1, Saminu KS2 1 Department of Physiotherapy, Faculty of Clinical Sciences, College of Medicine, University of Ibadan, Ibadan, Nigeria Code Number: hs11070 Abstract Background : Efforts to promote better health of sickle cell anaemia (SCA) patients in low-income countries through the use of cheap and available alternatives are desirable. Introduction Sickle cell anaemia (SCA) is a serious problem placing excessive demands on both the patients and their families. In Africa and the Caribbean, SCA is the commonest inherited disorder with about 200, 000 to 250, 000 children born per year. 1 Among people with SCA (homozygousfor sickle haemoglobin), the median age at death is 42 years for males and 48 years for females with haemoglobin SS (Hb-SS).2 In the Cooperative study of sickle cell disease (CSSCD), approximately 85 percent of children and adolescents with SCA and 95 percent of patients with sickle cell-haemoglobin C disease (heterozygous for haemoglobin S and C) survived only up to 20 years of age.3 Disorders of pulmonary functions are a likely contributor to the problem of life expectancy in these individuals. Pulmonary function is claimed to be abnormal in 90% of adults with SCA.4 It is likely that this reflects intrinsic lung disease in these patients and the mechanisms of the dyspnoea are more complex than originallyappreciated.4 The Peak expiratory flow rate (PEFR) studied in matched pairs of children with homozygous sickle cell disease revealed a highly significant reduction in PEFR of children with multiple episodes of acute chest syndrome when compared with those without.5 Similarly, measured forced vital capacity (FVC), forced expiratory volume in first second (FEV1) and PEFR in SCA subjects were significantly lower (p<0.001 respectively) than values obtained from nonsickle cell subjects.1,6 The effect of SCA on pulmonary functions becomes greater with increasing age and this has implications for the timing of commencement of treatment aimed at reducing chronic pulmonary morbidity in patients with SCA.1 Despite clinical advances, SCA remains a difficult, chronic medical condition for many children and youth. Therefore, additional treatment strategies, including complementary and alternative medicine therapies, would be welcome to enhance the clinical care of SCA patients.7 Peak expiratory flow is a useful measure of pulmonary health status and is frequently utilised in asthma management.8-9 Studies have demonstrated the benefits of physical activities in modification of expiratory flow rates in asthmatic patients10-11 but because of the possibility of exerciseinduced bronchoconstriction, exercises have general been used with caution among this group. However, PEFR is also found to be in the decline for many SCA patients, but the line of management does not usually include exercises. This study therefore examined whether simple daily chest exercise such as maximum inspiration and exhalation would lead to positive modification of PEFR in SCA teenagers. Methods This study was a randomized controlled pilot trial of SCA patients recruited from outpatient haematology clinics of a tertiary health facility, Aminu Kano Teaching Hospital, and a secondary health facility, Murtala Mohammed Specialist Hospital both of which are in Kano, North-Western Nigeria. It was conducted to investigate the effects of a locally designed incentive spirometry technique on the PEFR of teenage SCA patients. All SCA teenagers who were receiving care at both health facilities were potential participants for the study and they were invited for a preliminary meeting with the investigators. They were all assembled and the details of the exercise programme and assessments were presented to them, after which those who were interested were booked for recruitment into the programme based on whether they met the eligibility criteria. The eligibility criteria included being within the age of 13-19 years, not in any crisis and not smoking. Additional criteria also included consent to measurements and availability for re-assessments. They were however, informed of their freedom to withdraw from the study at any point in time. In order to compare the baseline PEFR of SCA patients with that of non-SCA individuals, we also assessed the PEFR of 25 age, height and sex matched apparently healthy controls who were not SCA patients (non-SCA group). The non-SCA participants were recruited from the Bayero University, Kano community. Ethical approval for this study was obtained from the Ethical Committee on Research of the Aminu Kano Teaching Hospital, Kano. Locally designed incentive spirometry An unused sterile surgical glove firmly tied with rubber band to the other end of an unused sterile injection syringe with its piston removed formed the incentive apparatus used for the exercise. This was self administered and was designed for single patient use. To exercise, the participants took in deep breath as much as they could (spirometry) and exhaled into the apparatus through the free end of the syringe that served as the mouthpiece. The inhalation and exhalation were allowed only once but they were encouraged to take in so much air that was capable of inflating all the finger points of the glove at one maximum exhalation. The bulging of the finger points of the gloves gave the necessary incentive expected to encourage maximum inhalation and exhalation. The idea behind this setup was that for a patient to be able to fully and strongly inflate the surgical gloves in one exhalation, he/she would have to take in deep air. By so doing, the lungs were adequately expanded and the airways were cleared, with every exhalation aimed at full inflation of the gloves. This exercise was done at three repetitions per session, thrice daily and for six consecutive weeks. The participants were asked to fill a diary indicating that the daily regimens were carried out. Participants in both SCA spirometry and SCA control groups reported to the clinic at the end of the third and sixth weeks for re-assessment of their PEFR. The participants in the SCA spirometry group had 378 spirometry sessions in six weeks while those in the SCA control group had none, although like those in the spirometry group, they were compliant with all prescribed drugs. The non-SCA group did not go through the spirometry programme but only had their PEFR assessed. Data Collection Peak Expiratory Flow Rate (PEFR) The PEFR was measured using the PEAK flow meter (a portable peak flow meter by Creative Biomedics, Inc. USA). While the participant was in standing position, the indicator of the peak flow meter was taken to the ‘0’ point. The participant was asked to inhale as deeply as possible, and then wrap his/her lips around the mouthpiece (open end of the syringe) in order to seal the mouthpiece and exhale air forcefully at once. The final position of the indicator was the subject’s PEFR measured in litres/ minute. The measurement was taken three times and the highest recorded. The PEFR was assessed in the clinic at the beginning of the study (baseline) and at the end of the third and sixth weeks in both spirometry and control groups while it was done only once for the non-SCA group. A survey of both centres identified only 49 teenage SCA patients who met our eligibility criteria out of 61 who were receiving treatment at the centres. They agreed to participate fully in the six week incentive spirometry programme and subsequently randomized into either of the SCA spirometry or SCA control groups of 24 and 25 participants respectively. The randomization was done using a fishbowl technique without replacement and the choice was concealed from the SCA participant who blindly picked either “A” or “B”, representing groups A or B from a “lucky dip”. Through the toss of a coin, groups “A” and “B” were later on decided as “SCA spirometry group” and “SCA control group”. As a way of blinding, the investigators were not involved in the assessment of the PEFR of the SCA and the non-SCA participants. The assessments were done by two other physical therapists that were not part of the investigating team. The PEFR score of each participant was identified by a specific research number assigned to each participant. The PEFR scores were submitted to the investigators as soon as they were available. Analysis of Data The baseline PEFR scores of the three groups were compared using one way Analysis of Variance (ANOVA), while the changes in PEFR over the six weeks period in each of SCA spirometry and SCA control groups were compared using the general linear model repeated measures. Scheffe ’s post hoc was further used to reveal periods of significance within the groups. Independent t-test was used to compare the PEFR of SCA spirometry and SCA control groups at the end of the sixth week. Significance level was set at 5% and data were analysed using the SPSS version 15. Results The participants in the SCA spirometry group went through the spirometry exercise for six weeks each. The mean ages for the SCA spirometry, SCA control and non-SCA groups were 17.6 ± 2.9, 16.9 ± 3.2 and 16.8 ± 3.9 years respectively. Their mean heights were 1.48 ± 2.4 m, 1.45 ± 2.1 m and 1.52 ± 2.5 m respectively [Table - 1]. At baseline, the mean PEFR in the non-SCA group (348.80 ± 46.12 l) was higher than that of SCA spirometry and SCA control groups. This difference was statistically significant (F = 63.35; p < 0.05) when compared with the two SCA groups [Table - 2] [Table - 3]. Discussion The main finding of this study was that teenagers with Sickle cell anaemia (SCA) had lower peak expiratory flow rate (PEFR) values compared to their age, sex and height matched apparently healthy, non-SCA individuals. However this improved significantly after a six-week period of daily breathing exercises using a local form of incentive spirometry. The improvement, which began to manifest after three weeks of daily use of the apparatus, continued through to the sixth week. The mean PEFR of the SCA spirometry group attained at the sixth week did not however reach that of their matched non-SCA teenagers. The SCA control subjects who did not take part in the exercise did not have any significant improvement in their PEFR at the end of the six weeks. The fact that we were able to achieve improvement in the SCA spirometry group and not in the SCA control group might have been because the former were taken through the thricedaily local incentive spirometry, which helped to improve their inspiration and exhalation capacity. However, the fact that they did not reach the PEFR levels of their matched non-SCA individuals in six weeks of daily exercise implies that six weeks of the spirometry was not enough to normalize the PEFR of teenage SCA patients. Based on the comparison of PEFR scores of the SCA and non-SCA patients, our study supports the findings of previous studies that lung function parameters are impaired in SCA patients.1,4-6 These studies found that in addition to Forced Vital Capacity (FVC) and timed forced expiratory volume (FEV1), PEFR was also on the downward trend in SCA patients. The reason for the reduced PEFR found in the group of teenage SCA patients may not be unconnected to the accumulating pulmonary fibrosis that decreases lung compliance5 or it may be the result of repeated lung damage caused by episodes of pulmonary vasoocclusion12 and these episodes could start from childhood.1 The improvement in PEFR seen in this study following six weeks of incentive spirometry could be because the inflation of the surgical glove used in the locally designed apparatus required maximal exhalation of inspired air. Incentive spirometer measures the inspiratory capacity of the lungs and is designed to encourage deeper inspiratory effort.13 The ability to inflate the glove through exhalation was a sequel of the participant’s deep inspiratory effort. The fact that we found reduced PEFR in our sample of teenage SCA patients compared to non-SCA subjects, as well as the fact that the PEFR of the SCA spirometry group improved following a period of breathing exercise makes PEFR a relevant tool in assessing responses to breathing exercise in SCA patients. This is also of major implication for clinical practice because it implies the need for routine treatment, which could begin with complementary therapies including exercises. Recently though, Sylvester et al.14 found that in a group of Afro-Caribbean children, peak expiratory flow was not a useful method of monitoring the respiratory status of children with SCA. In a Nigerian survey however, pulmonary function (including PEFR) was found to be reduced in children and young adults with SCA compared to controls although, for both groups, it was directly related to body composition.15 This study had a few limitations that may warrant careful interpretation of the outcomes. First, the study was a pilot study and the sample was not large which may have implications bordering on sufficient statistical power to detect treatment effect. The inability to arrive at adequate sample size for adequate statistical power may be because of our eligibility criteria. Ab-initio we had set out to recruit only participants who would comply with the exercise regimen since it required more of selfdirected participation outside the hospital setting. At the point of recruitment prior to randomization, the demand was made clear and those who would not be able to comply declined to participate. This, in addition to the teenage age requirement for participation reduced the sample available for the study. Sample size was not determined since only a total of 49 participants signified their intention to participate and they were all recruited. In view of the size of the sample, we acknowledge that part of the outcome may be due to chance. However, likely bias in the study could have been reduced by the fact that this study had a randomized group assignment of participants, investigators were blinded to theassessments of outcomes and the comparison of SCA spirometry group with SCA control (nonspirometry) group as well as comparison with non-SCA teenagers. The second limitation was that this study required that the SCA spirometry group participants carried out sessions of the spirometry out of the hospital settings without the strict supervision of any health personnel. The authenticity of their compliance may not be fully ascertained as some may not follow the regimen strictly. However, because the recruitment exercise spelt out this requirement with detailed documentation of the activity diary, and because significant improvement was actually noticed in the PEFR of the SCA spirometry group, it could be taken with fair confidence that the participants carried out the spirometry as prescribed. The outcome of this study may also be influenced by a number of confounders that we did not account for. Such factors include motivation, diet, prior participation in physical exercise and exposure to clinical levels of dusts and other pollutants. However, all the participants in this study were selfreported that they had never smoked. A major strength of this study on the other hand was that we were able to demonstrate the effective use of a cheap, available, fun-filled and locally assembled apparatus to improve the PEFR of teenage SCA patients. This can be easily assembled for use during admission in the hospital and after the period of hospitalization since the materials are available both in and outside the hospital setting. Conclusion The PEFR was lower in the SCA teenagers than their age, sex and height-matched apparently healthy non-SCA teenagers. Furthermore the PEFR showed significant improvement from third to sixth week following a thrice daily incentive spirometry using a locally assembled apparatus. However, the improvement noticed at the sixth week among the SCA spirometry participants did not reach the PEFR of non-SCA teenagers. Exercise that will improve PEFR in teenage SCA patients should be routine in order to improve their pulmonary status. This may help to reduce one of the burdens among a myriad of problems faced by these individuals with this genetic disorder. It is also desirable to have wide researches to generate normative PEFR and other lung function parameters for both SCA and non-SCA children and adolescent of African origin. Acknowledgement We thank the participants, their health care providers and the health facilities from where data for this study were collected. We also thank the Physical therapists who participated in the data collection. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11070t2.jpg] [hs11070t3.jpg] [hs11070t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}