 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
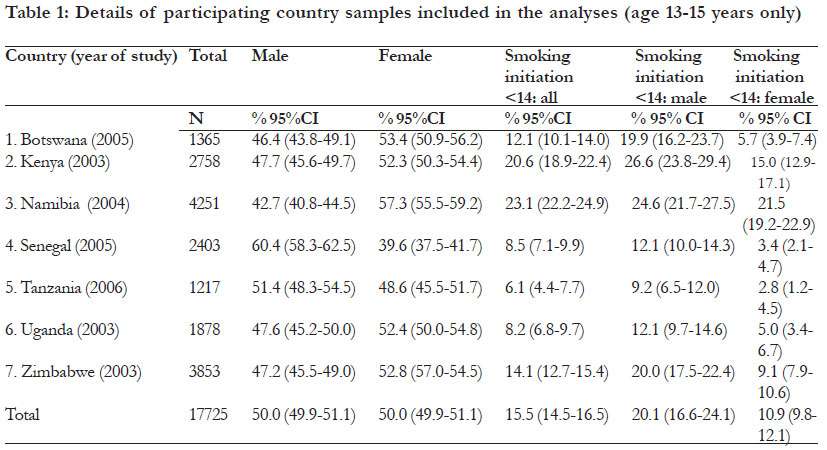
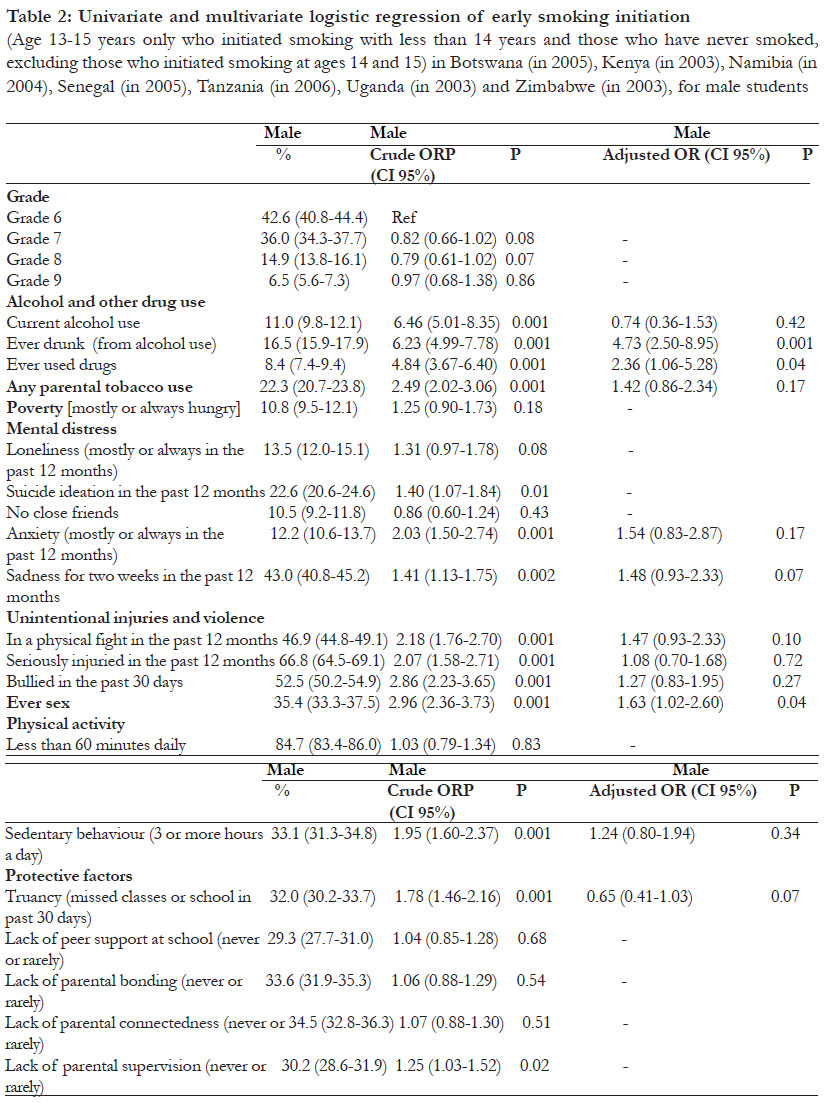
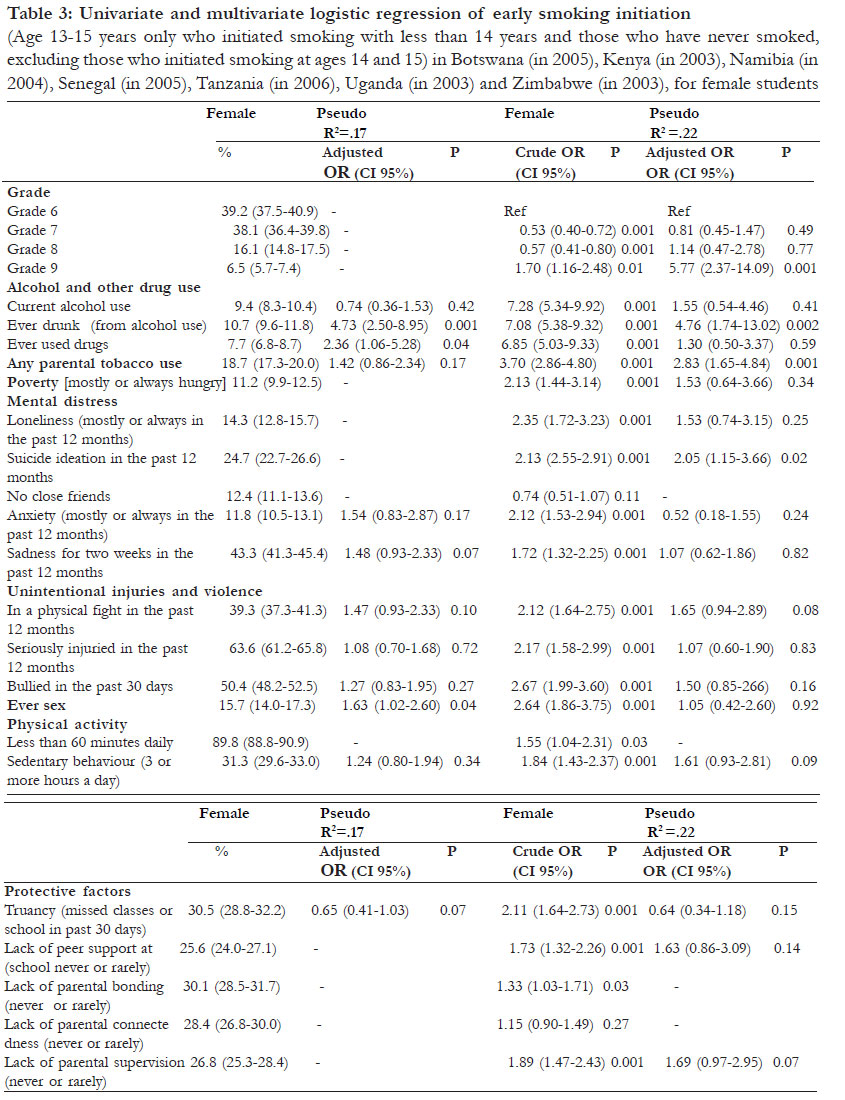
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 320 - 328 Early smoking initiation and associated factors among in-school male and female adolescents in seven African countries *Peltzer K1,2 1 HIV/AIDS/STI/and TB (HAST), Human Sciences Research Council, 134 Pretorius Street, Pretoria 0002, South Africa, 2 Department of Psychology, University of Limpopo, South Africa Code Number: hs11073 Abstract Objective: This report examines the prevalence and common correlates of early smoking initiation among male and female school children across seven African countries. Key words: Smoking; Early initiation; Adolescents; Psychosocial correlates, Health-compromising behaviours, Protective factors, African countries Introduction The age of smoking initiation is an important determinant of an individual’s probability of becoming addicted to tobacco, probability of smoking cessation, and risk of adverse health outcomes1. Adolescents who begin to smoke at or before age 13 are twice as likely to remain smokers in adulthood as are those adolescents who begin to smoke at age 17 or later2. Early initiation of cigarette use is associated with higher levels of nicotine dependence and serious health outcomes3. The firstuse smoking experience is a symbolically significant and enduring life event4. Various studies have identified variables associated with the likelihood that an individual will experiment with smoking or become a regular smoker. These include low socioeconomic status, access to tobacco products, perceptions that tobacco use is normative, smoking by peers and siblings, lack of parental involvement, low academic achievement, lack of cigarette refusal skills, low self-esteem, high perceived benefits of smoking, low perceived risks of smoking, engagement in other health risk behaviours such as substance use and sexual risk behaviour, community, family, and school variables5,8 . Little information is available about the prevalence of and relationship between early smoking initiation and a range of psychosocial factors among an adolescent population in Africa9. Based on the Global Youth Tobacco Survey (GYTS) of 1999 and 2002 among adolescents in South Africa ever smokers (even one or two puffs) were 46.7% in 1999 and 37.6% in 2002. Among ever smokers, 18.5% in 1999 and 16.2% in 2002 first smoked cigarettes before the age 10 years10, and among a nationally representative sample of in-school adolescents in 2002 30.5% of learners reported ever having smoked cigarettes (ever tried smoking cigarettes) and 6.2% of learners had smoked their first cigarette (tried a cigarette) before the age of 10 years11. According to and based on the Demographic and Household Survey of 2003, 7.0% of males and 7.9% of females among 15 year-olds ever had smoked any tobacco products12. Therefore the aim of this study was to examine the prevalence and common correlates of early smoking initiation among school children across seven African countries. Methods Description of survey and study population This study involved secondary analysis of existing data from the Global school-based health survey (GSHS) from seven African countries (Botswana, Kenya, Namibia, Senegal, Tanzania, Uganda and Zimbabwe, Swaziland and Zambia did not collect information on smoking). All African countries from which GSHS datasets were publicly available were included in the analysis. From all but two cof the countries national samples were included, while from Tanzania it was only the Dar es Salaam region and from Zimbabwe three areas: Harare, Bulawayo and Manicaland. The aim of the GSHS is to collect data primarily from students of age 13 to 15 years. In each country, the questionnaire comprises multiple core modules, core-expanded questions and countryspecific questions, and a standardized scientific sample selection process and common school-based methods are followed. Further details of the GSHS can be obtained at http://www.who.int/chp/gshs. Measures The GSHS 10 core questionnaire modules address the leading causes of morbidity and mortality among children and adults worldwide: tobacco, alcohol and other drug use; dietary behaviours; hygiene; mental health; physical activity; sexual behaviours that contribute to HIV infection, other sexuallytransmitted infections, and unintended pregnancy; unintentional injuries and violence; hygiene; protective factors and respondent demographics 13. Substance use variables Cigarette Cigarette use was assessed with (1) “How old were you when you first tried a cigarette?” Response options were 1=I have never smoked cigarettes, 2=7 years old or younger, 3=8 or 9 years old, up to 6=14 or 15 years old; the dependent variable of interest, early initiation of smoking at or before the age of 13 years. (2) “During the past 30 days, how many days did you smoke cigarettes?” Response options were from 1=0 days to 7= all 30 days, coded 1=1 or 2 to all 30 days, and 0=0 days). (3) “During the past 12 months, have you ever tried to stop smoking cigarettes?” Response options were either did not smoke or ‘yes’ or ‘no’. (4) “During the past 7 days, on how many days have people smoked in your presence?” Response options were 1=0 days to 5=all 7 days; coded 1=2-5, 1 or more days and 0=0 days. Further, (5) parental tobacco use was assessed with the question “Which of your parents or guardians use any form of tobacco?” (Response options were 1=neither, 2=my father or male guardian, 3=my mother or female guardian, 4= both, 5=I do not know, coded 1=2 or 3 and 0=1, 4 and 5). Alcohol Alcohol use was measured with three variables: a) during the past 30 days, on how many days did you have at least one drink containing alcohol. Response options were from 1=0 days to 7=all 30 days; Coded 1=1 or 2 to all 30 days, and 0=0 days. b) Excessive drinking: During your life, how many times did you drink so much alcohol that you were really drunk? Response options were from 1=0 times to 4=10 or more times; Coded 1=1 or 2 to 10 or more times, and 0=0 times. Response options were from 1=0 times to 4=10 or more times; Coded 1=1 or 2 to 10 or more times, and 0=0 times. Drugs During your life, how many times have you used drugs, such as glue, benzene, marijuana, cocaine, or mandrax? Response options were from 1=0 times to 4=10 or more times; Coded 1=1 or 2 to 10 or more times, and 0=0 times. Sexual risk behaviour The question considered here was “Have you ever had sexual intercourse?” Response option was “Yes” or “No”. Poverty A measure of poverty was derived from a question reporting the frequency that a young person went hungry because there was not enough food at home in the past 30 days (response options were from 1=never to 5=always, coded 1=most of the time or always and 0=never, rarely or sometimes). Unintentional injury and violence Being in a fight was measured with the question “During the past 12 months, how many times were you in a physical fight?” Response options were from 1=0 times to 8=12 or more times (coded 1=1 time to 12 or more times and 0= times). Bullied was measured with the question “During the past 30 days, on how many days were you bullied?” Response options were from 1=0times to 7=all 30 days (coded 1=1 or 2 days to all 30 days, and 0=0 days). “During the past 12 months, how many times were you seriously injured?” (Serious injury was defined as “when it makes you miss at least one full day of usual activities (such as school, sports, or a job) or requires treatment by a doctor or nurse). Eight options were provided, ranging from 1=0 times to 8=12 or more times. A response of “0” was described as not having sustained a serious injury, whiles a response of one or more times was classified as having experienced a serious injury. Mental distress variables Loneliness During the past 12 months, how often have you felt lonely? (Response options were from 1=never to 5=always) (Coded 1= most of the time or always and 0=never, rarely or sometimes). Suicide ideation ‘‘During the past 12 months, did you ever seriously consider attempting suicide? (Response option was 1 = yes and 2 = no, coded 1 = 1, 2 = 0). No close friend ‘‘How many close friends do you have?’’ (Response options 1 = 0 to 4 = 3 or more, coded 1 = 1, 2-4 = 0.). Sadness During the past 12 months, did you ever feel so sad or hopeless almost every day for two weeks or more in a row that you stopped doing your usual activities? (Response option 1=yes and 2=no) (Coded 1=1, 2=0). Physical activity Leisure time physical activity was assessed by asking participants: “Physical activity is any activity that increases your heart rate and makes you get out of breath some of the time. Physical activity can be done in sports, playing with friends, or walking to school. Some examples of physical activity are running, fast walking, biking, dancing, football. Do not include your physical education or gym class.” “During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?” Response options were from 1=0 days to 7=7 days, coded 1=7 days and 0=0 to 6 days. Leisure time sedentary behavior was assessed by asking participants about the time they spend mostly sitting when not in school or doing homework: “How much time do you spend during a typical or usual day sitting and watching television, playing computer games, talking with friends, or doing other sitting activities.” Response options were from 1=less than 1 hour per day to 6=more than 8 hours per day, coded 1=3 or more hours a day and 0= less than 3 hours a day. Protective factors These included school attendance, peer support at school, parental or guardian supervision, connectedness, and bonding) Data analysis In order to compare study samples across countries each country sample was restricted to the age group 13 to 15 years. Younger and older participants were excluded from the analyses. Data analysis was performed using STATA software version 10.0 (Stata Corporation, College Station, Texas, USA). This software has the advantage of directly including robust standard errors that account for the sampling design, i.e. cluster sampling owing to the sampling of school classes. In further analysis, the age of first smoking variable was recoded into two categories: early smoking initiation (below 14 years) 1 and never smoked cigarettes10. This definition of those ever having tried a cigarette covers a range of people, including those who experiment, those who might eventually become regular smokers, those who already smoke regularly, those who have stopped smoking, those who might stop in the near future and those who smoke occasionally. The case sample for this current analysis included participants who responded that their smoking initiation was at age 13 years or before. The control sample included those participants who have not initiated smoking. Those who initiated smoking at 14 or 15 years (3.5% of the sample) were excluded from this analysis. Associations between alcohol, drug use, socioeconomic status, mental distress, physical inactivity, protective factors and early smoking initiation among school children were evaluated for boys and girls separately and the odds ratios (OR) were calculated. Logistic regression was used for evaluation of the impact of explanatory variables for early smoking initiation (binary dependent variable); variables found significant at p<0.01 level at univariate analysis were included in the multivariable analysis. In the analysis, weighted percentages are reported. The reported sample size refers to the sample that was asked the target question. The two-sided 95% confidence intervals are reported. The p-value less or equal to 5% is used to indicate statistical significance. Both the reported 95% confidence intervals and the p-value are adjusted for the multi-stage stratified cluster sample design of the study. Results Sample characteristics, early smoking initiation and smoking behaviour The final total sample included 17,725 school children aged 13 to 15 years from seven African countries. At the participant level, response rates varied from 76% in Uganda to 95% in Botswana. There were 50% female and 50% male school children. In all 15.5% of the 13-15 year-old school children reported early smoking initiation; this was overall significantly higher among boys (20.1%) than girls (10.9%). Namibian, Kenyan, Zimbabwean and Batswana 1315 year-old school children had the highest prevalence of early smoking initiation (23.1%, 20.6%, 14.1% and 12.1%, respectively), and Tanzanian and Ugandan had the least (6.1% and 8.2%, respectively) (see [Table - 1]). From the early smoking initiators 50.9% are current smokers. Of the current smokers, 30.8% initiated smoking at 7 years or less at 25.0%, 8 or 9 years at 18.1%, 10 or 11 years at 15.9%, 12 or 13 years and 22.2%, and 14 or 15 years 18.9%. Further, 82.4% of the current smokers had smoked in the presence of others at least for one day during a whole week and 56.9% of the current smokers had tried to stop smoking in the past 12 months. Overall, there were 10.2% current smokers of whom 12.9% among boys and 7.5% were girls. Early smoking initiation and its relationship with social and behavioural variables In univariate regression analyses boys and girls with early smoking initiation at less than age 14 were more likely to report alcohol use, drug use, parental or guardian tobacco use, mental distress (suicide ideation, anxiety, sadness), unintentional injuries and violence (having been in a physical fight, seriously injured or bullied), ever had sex, sedentary leisure time behaviour and protective factors (truancy, lack of parental supervision). Further, in univariate regression analyses among girls, loneliness, physical inactivity, lack of peer support at school and lack of parental bonding were associated with early smoking initiation. In multivariable analysis, early smoking initiation among boys was associated with ever drunk from alcohol use (OR=4.73, p=0.001), ever used drugs (OR=2.36, p=0.04) and ever had sex (OR=1.63, p=0.04), and among girls associated with higher education (OR=5.77, p=0.001), ever drunk from alcohol use (OR=4.76, p=0.002), parental or guardian tobacco use (OR=2.83, p=0.001) and suicide ideation (OR=2.05, p=0.02) see [Table - 2] and [Table - 3]. Discussion This study found that 15.5% had experienced smoking initiation before age 14 of which 20.1% wereboys and 10.9% were girls. These early smoking initiation figures seem higher than that found in Zimbabwe among rural secondary school students (6%; 9.0% among boys and 2.8% among girls) 14 but lower than among 15 year-old school children (48.5%; 54% for boys and 45% for girls) in Bulgaria6, and 40% among 13 year-old school children in the WHO European Region and North America from the Health behaviour in school children (HBSC) survey15. This study found large cross-national variations in the prevalence of early smoking initiation that. The observed differences could be associated with the relative economic development of the countries, different emphasis of public health programmes and cultural variation. Country results constitute evidence that should be taken into consideration by national tobacco control policy makers to address the needs of adolescents. Gender differences in early smoking initiation may be interpreted as reflecting traditional norms in many African countries that allow or even encourage more freedom and smoking experiences for boys than for girls. In this study, several tobacco use risk behaviours were identified. From the early smoking initiators 50.9% are current smokers. Of the current smokers, 43.1% had initiated smoking below 10 years of age. Further, 82.4% of the current smokers had smoked in the presence of others at least for one day during a whole week. As high as 40% of the current smokers had not tried to stop smoking. This can be compared to other studies e.g. among 13-15 year-old school children in Seychelles 77.1% of current smokers16 and among urban 13-15 year-old school children in Uganda 76.9% had tried to stop17. Overall, from the total sample there were 10.2% current smokers, (12.9% among boys and 7.5% among girls). These current smoking rates seem similar to information on 13-15 year-old school children from the GYTS for the African region collected from 1999 to 2005 in 25 of 48 WHO member states. In that survey, 9.2%, figures were 13.0% for boys and 5.8% for girls18 and were collected from 2000 to 2007 in 26 of 46 WHO member states, statistics were 8.0%, 13.5% for boys and 5.2% for girls19. The study found that correlates of early smoking initiation included in concordance with other studies: higher in boys8,14,20, higher grades20, low socioeconomic status (poverty among females in univariate analysis)5,6,20, alcohol and drug use5,7,8, sexual risk behaviour (ever had sex) 5,7, school factors (truancy among males) 8, family factors (parental or guardian tobacco use, lack of parental or guardian supervision) 5,6,17, for girls, poor mental health5,6 and violence (having been in a physical fight) 21. It appears that the identified healthendangering behaviours that is, early smoking initiation, alcohol and drug use and sexual risk behaviours are clustered together, as found in other studies22. DuRant et al.8 found that early age of onset of cigarette use was the strongest correlate of the number of health risk behaviours in which young adolescents had engaged in. Findings are consistent with Problem Behaviour Theory23, in which early onset of adolescent smoking behaviour is considered behaviour with underlying influences that are shared with other problems behaviours. The findings suggest that screening for early experimentation with smoking will help identify young adolescents at increased risk for smoking and engaging in multiple health risk behaviours. The connection between smoking activity and various risk factors including problem behaviour such as alcohol and drug use, early smoking initiation and mental distress indicates that prevention programmes should broaden tobacco health promotion and include these factors collectively in health interventions for early adolescents. Future research in Africa should include accessibility of young people to tobacco (legislation, price) and tobacco publicity. Anti-tobacco policies, supported by legislations that prohibit the sale of tobacco to underage children, advertising, etc. have been more effective than educational interventions in reducing the prevalence of tobacco consumption in the developed world (USA and Europe). If African authorities do not follow the example of the policies developed in the countries with more resources, the health of new generations of Africans will suffer the consequences of the smoking epidemic. Limitations of the study This study had several limitations. Firstly, the GSHS only enrolls adolescents who are in school. Schoolgoing adolescents may not be representative of all adolescents in a country as the occurrence of smoking initiation and behaviour may differ between the two groups9. As the questionnaire was selfcompleted, it is possible that some study participants may have misreported either intentionally or inadvertently on any of the questions asked. The questionnaire used in this study measured different concepts such as mental distress, poverty and social cohesion (close friends). These are variables with single items, which are quite limited in their use as quantitative indices. A number of risk factors associated with early smoking initiation found in other studies such as use of other tobacco products, access to tobacco products, perceptions that tobacco use is normative, smoking by peers and siblings, academic achievement, self-efficacy skills, perceived benefits of smoking, perceived risks of smoking, social self esteem, body image, community, and school variables5-8 were not assessed and should be assessed in future studies. Furthermore, this study was based on data collected in a cross sectional survey. We cannot, therefore, ascribe causality to any of the associated factors in the study. Prospective studies are required to follow up smoking behaviour and associated factors in African countries24. Conclusion The study found a high prevalence of early smoking initiation among 13-15 year-olds in seven African countries. Various risk factors have been identified in boys and girls who initiate smoking before age 14 forming a distinct risk group in this setting. Specific interventions are needed for boys and girls in the preteen years, before smoking initiation. Acknowledgements I am grateful to the World Health Organization (Geneva) and the Centers for Disease Control and Prevention (Atlanta) for making the data available for analysis, and the country coordinators from Botswana (Rachel Mosinyi), Kenya (William K. Maina), Namibia (Kornelia K. Abraham), Senegal (Samba Cor Sarr), United Republic of Tanzania (Ursuline S. Nyandindi), Uganda (Jermiahs Twa-Twa) and Zimbabwe (Edwin Sithole) for their assistance in collecting the Global School-based Student Health Survey data. I also thank the Ministries of Education and Health and the study participants for making the Global School Health Survey in the nine African countries possible. The governments of the respective study countries and the World Health Organization did not influence the analysis, nor did they have influence on the decision to publish these findings. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11073t2.jpg] [hs11073t1.jpg] [hs11073t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}