 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 329 - 333 Actual and perceived substance use of health science students at a university in the Western Cape, South Africa *Steyl T, Phillips J
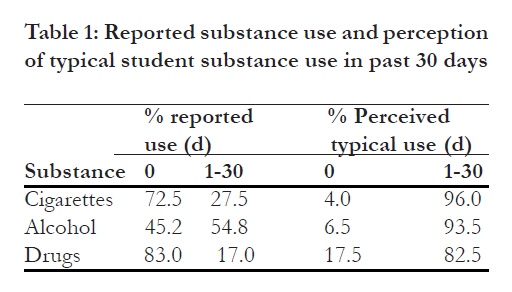
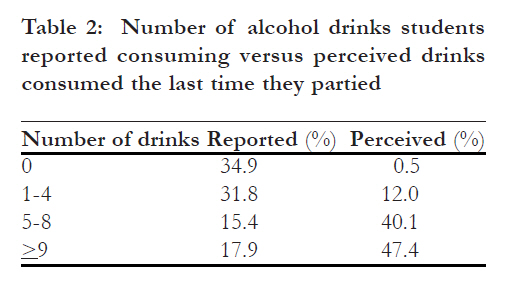
Department of Physiotherapy, University of the Western Cape, Bellville, South Africa Code Number: hs11074 Abstract Background: Substance use among youth is a worldwide epidemic that impacts negatively on the health sector as well as the family and society. Early student life is a time of tremendously high motivation to conform to the behaviours, values, and attitudes that are valued by the youth culture. They observe their peers’ behavior and alter their own behaviour with their peers’ norms and expectations. This compliance with perceived peer norms can however lead to increased smoking, alcohol and drug use. Substance use among youth is a worldwide epidemic. Not only does it have a negative impact on the health sector, but it also impacts negatively on the family and society in terms of crime and social development 1. Various studies suggest that students entering the university put themselves at risk through unhealthy behaviours. Universities are often settings where students experience independence and freedom from direct adult supervision and support networks for the first time2,3. This freedom, however presents new stressors associated with a different structure to daily life and greater responsibilities. Students enter an environment where normative values may be different from parental values, thus causing them to question individual beliefs, values and goals. Young adults begin to assume responsibility for many lifestyle choices affecting their health. Some of these choices are healthy, whereas others such as using tobacco, alcohol or drugs may not be4,5. Recent evidence from the World Health Report suggests that tobacco and alcohol are among the top ten risk factors leading to disease and injury in developing nations6. This leads to an increase in medical costs, as well as an increase in crime, motor vehicle accidents, and early mortality7,8. The use of other drugs has frequently been found to be associated with smoking. Adolescents and young adults are likely to use alcohol and tobacco concurrently. Both of these substances have been implicated as ‘gateway’ drugs, increasing the likelihood of subsequent illicit drug use9. Studies revealed that tobacco use was significantly greater among students who binge drink and smoke marijuana3,10. Among youths, the use of alcohol and other drugs has also been linked to unintentional injuries, physical fights, academic problems and illegal behaviour11. Furthermore, Naimi et al12 pointed out that drug use contributes directly and indirectly to the HIV epidemic. An important risk factor for adolescent smoking, alcohol and drug use is perceived peer norms. Early student life is a time of tremendously high motivation to conform to the behaviours, values, and attitudes that are valued by the youth culture. Youths observe their peers’ behaviour and alter their own behaviouraccording to their peers’ norms and expectations. Health science students are the future health professionals who will promote healthy living and disease prevention. Being a student in a health science course, however, does not ensure health promoting behaviours. Since health science students are in an inimitable position to influence and inspire other students to lead a healthy lifestyle, it is of utmost importance that they fully understand the consequences of engaging in health risk behaviours. Misperceptions regarding peers engagement in risky behaviour can however have a causal effect on health science students’ own behaviour, consequently leading to increased risky behaviour among health science students. Therefore the overall aim of the study was to determine and analyze health risk behaviours among students of a Health Science Faculty at a university in the Western Cape, South Africa. In this paper only the association between actual risk and perceived risk for substance use will be discussed. Method A cross-sectional study was conducted among students of a Health Science Faculty at a university in the Western Cape, South Africa. The population for this study included all full-time undergraduate 2 nd year health science students of the 2006 academic year (508 students). Second-year university students represent a homogeneous population who have presumably adjusted to university life and are free of the stresses of final-year examinations. Webb et al13 also argue that it is unlikely that these students will radically change their lifestyles in subsequent university years. Instrument Participants were given a self-administered questionnaire consisting of two sections. Section one was a self-constructed section measuring demographic and socio-economic characteristics of the participants. Section two included items from the National College Health Risk Behaviour Survey (NCHRBS) as well as the American College Health Association National College Health Assessment (ACHA-NCHA). Content validity, applicability of the items, and the level of understandability were assessed by piloting the questionnaire on 20 students who were not included in the study, followed by a focus group discussion. The results indicated that the instrument was relevant to the population and it was easily used by the students. Only a few grammatical changes were made before the final questionnaire was administered to the participants. Data collection A conveniently selected sample of 201 2 nd year students, ranging from age 18 – 24 years, with a mean age of 22.16 years (SD=4.68, median= 20.0), completed and returned the questionnaires. The overall response rate was 58.3%. Although the low response rate was a concern, other college and university studies also obtained approximately 50% participation rates, so the response rate for our study is not out of line14. Data analysis To determine the correlation between actual and perceived health risk behaviours, the health risk behaviours were treated as categorical data and chisquare analyses were conducted. Cramer’s V test was employed to compare actual and perceived substance use by frequency of individual use. Results Overestimated consumption patterns for the typical student behavior were found when perceptions of typical student behaviour were compared to actual reported behaviour. [Table - 1] summarizes the reported substance use (cigarette smoking, alcohol use and drug use), and the perception of typical student use in the 30 days preceding the study. More than a quarter (27.5%), of the students reported smoking in the past 30 days, while 96.0% believed that the typical student smoke cigarettes on one or more days during the 30 days preceding the study. The majority (83.0%) of the students reported not using any drugs in the 30 days preceding the study, but only 17.5% believed that students did not use any drugs in the 30 days preceding the study. The comparison between the reported number of alcoholic drinks versus perceived number of alcohol drinks consumed the last time students partied are summarized in [Table - 2]. Almost one third (31.8%) of the students reported consuming between 1 and 4 drinks the last time they partied. Contrary to this, the majority (47.4%) of students believed that the typical student consumed >9 alcoholic drinks the last time they partied, whereas only 17.9% reported to consuming this number of alcoholic drinks. [Table - 3] summarizes the comparisons of actual versus perceived substance use by frequency of individual use. A statistically significant chi-square emerged for the alcohol use analysis. For all three analyses a larger than expected number of students who engaged in substance use, reported that the typical student engaged in these risky behaviours. However, as can be seen from the Cramer’s V statistic, effect sizes were all fairly low. Using guidelines of .1 corresponding to a small effect and .3 corresponding to a medium effect, all effect sizes were in the small range. Discussion Several researchers have highlighted that students generally misperceive the frequency with which their peers engage in smoking, alcohol and drug use and that these misperceptions have a causal effect on individual behaviour 15,16. It is also further believed that students may be more likely to engage in behaviour when they view the behaviour as typical or normative. In the current study it is clear that students viewed smoking as typical or normative for students. Smoking is often portrayed by various media outlets as being typical or normative of university life. Therefore students may perceive that smoking is engaged in more frequently than it actually is. These misperceptions of peer norms clearly have important educational or prevention program implications. The same trend for overestimating peer use, was found for both alcohol and drug use. The findings coincide with results from Jones et al17 who stated that many university students overestimate the extent to which their peers use alcohol. The same was true for drug use, as the study highlighted that a larger than expected number of students who used drugs, reported that the typical student used drugs. These findings clearly indicate that educational and awareness programs regarding alcohol and drug use should take perceptions of peer alcohol and drug use into consideration. Some researchers18 are also of the opinion that normative re-education in which students’ beliefs about peer drinking rates are higher, should be challenged. Noteworthy is the co-occurrence of smoking, alcohol and drug use. Several researchers have reported that cigarette smoking in adolescence represents a crucial entry-point to illicit drug and alcohol use9,19-21. Gledhill-Hoyt et al21 furthermore reported that students who engage in polydrug use are at greater risk for alcohol-related motor vehicle accidents as well as problems such as property damage and getting in trouble with the police than students that only use one substance or binge drink. These findings should be kept in mind when preventative programs are developed as these programs should not only concentrate on one risk behavior but multiple risk behaviours. Health education has become an increasingly important part of health and medical care. Health professional students are potentially well suited to be health educators. They are knowledgeable about the causes and risk factors of diseases. However, Kamwendo et al. (2000) noted that the educator’s role is complicated by the fact that he or she is not only a conveyer but also a recipient of information. Furthermore the educator will have to make a decision about his or her own health behaviour. If they do not adhere to the advice advocated by medical authorities, they end up in the awkward position or conveying conflicting messages to patients or clients. Given the results of the study, prevention programs should be started in early adolescence as literature suggests that the engagement of many health risk behaviours among university students are a continuation of engagement in such behaviours in high school. This however does not mean that health promotion activities at university level are futile as universities offer an important avenue for healthrelated services and education to a large number of young adults. University health educators should however not only provide appropriate health promotion programmes, but should also encourage students to take responsibility for their own unhealthy lifestyles23. Conclusion Health science students are the future health professionals that are in an inimitable position to promote a healthy lifestyle amongst fellow students. Misperceptions regarding peers engagement in risky behaviours can however have a causal effect on their own behaviour. Since the participants in this study were health professional students, a population that is theoretically knowledgeable about the risks of engaging in these behaviours, it is clear that prevention or health promotion programs should take the factors influencing engagement in risk behaviours into consideration. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11074t1.jpg] [hs11074t3.jpg] [hs11074t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}