 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
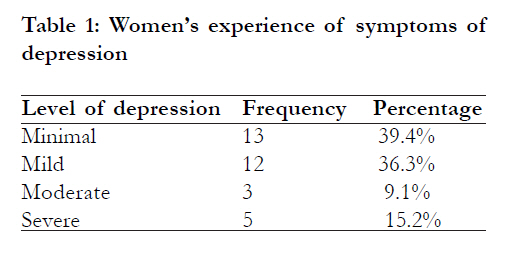
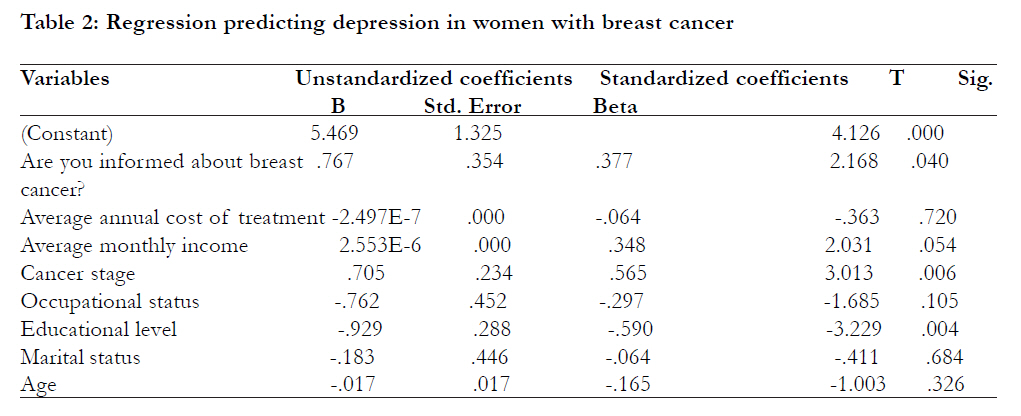
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 341 - 345 Measured effect of some socio-demographic factors on depression among breast cancer patients receiving chemotherapy in Lagos State University Teaching Hospital (LASUTH) *Akin-Odanye, EO1, Asuzu Chioma C1, Popoola Abiodun O2 1 Department of Guidance and Counselling, University of Ibadan, 2Consultant Radiation Oncologist, Lagos State University Teaching Hospital Code Number: hs11076 Abstract Background: Breast cancer is a disease predominantly found amongst women. It is a disease which threatens an organ that is intimately associated with a woman’s self image, sexuality, as well as her reproductive and nurturing capacity. These threats have serious psychological implications for women living with breast cancer. Key words: Breast, cancer, woman, depression, chemotherapy Introduction A woman ’s breast is an organ whose psychological functions are as important as its physical determinant of feminine attractiveness. The breast is related not only to core gender identity but also to the concepts of motherhood and caring. Any disease that threatens the breast will invariably endanger a woman’s sense of psychological wellbeing. Breast cancer is a disease predominantly found amongst women though one in a hundred men are annually being diagnosed of the disease1. The treatment for breast cancer is hinged upon the surgical removal of an organ that is tied intimately to a woman’s sense of femaleness, sexuality and mothering capacity2. Massie and Holland,3 studied the psychological reactions to breast cancer in individuals and confirmed that it is a disease which threatens an organ that is intimately associated with self image, self esteem, sexuality, femininity and reproductive and nurturing capacity. They concluded therefore, that breast cancer is a source of significant stress and depression for any woman. Massie and Holland,3 conclusion was further buttressed by the work of Zainal, et al4 who reported a 51% prevalence of psychological distress as determined by the ‘Distress Thermometer’ and 32% prevalence of depression and anxiety as measured by the Hospital Anxiety and Depression Scale (HADS). Women with breast cancer who have had a mastectomy feel mutilated and experience depression and loss of femininity. Breast cancer diagnosis and treatment are traumatic to patients. The interaction between such patients with other people results into various emotional and behavioural side effects of which anxiety and depression are the most frequent2. It follows then that the discovery of a lump in a woman’s breast, has both physical implication seen in the need for her to navigate through the healthcare system and an emotional implication characterized by deep feelings, emotions, and fears. This condition was described by Lackey, Gates, and Brown5 as “dual experience trajectory”. Furthermore, studies indicate that arounda quarter of female breast cancer patients exhibit clinically significant distress in the first year after diagnosis,6. Younger age has consistently been associated with increaseddistress in cancer patients7 . In a sample of women diagnosed with primary breast cancer, factors including younger age and greater number of postsurgical treatments were associatedwith higher psychological distress8. Cancer stage is a key predictor ofdistress, with the potential for psychological distress occurringat various points including diagnosis, treatment, follow-up, and recurrence. Treatment side effects of radiotherapy and hormone therapy, such as nausea, weight gain, pain and fatigue, may also causedistress,9 and breast surgery may generate concerns about body image10 especially amongst Africans and African-Americans who may have difficulty in finding prostheses that match their skin tone11. Cultural background may affect the process of adaptation. African-American women are more likely to view a diagnosis of cancer as a death sentence, suggesting that convictions related to outcome may influence diagnostic delay or treatment refusal5. African-American women are more likely to have mastectomies, less likely to have breast reconstruction, less likely to be given a rationale for treatment decisions, and often do not ask questions about their illnesses12. These factors could lead to depression in breast cancer patients if they go unchecked. The diagnosis of depression in people with cancer can be difficult due to the problems inherent in distinguishing biological or physical symptoms of depression from symptoms of illness or toxic side effects of treatment. This is particularly true of individuals who are receiving active treatment or those with advanced disease. Cognitive symptoms such as guilt, worthlessness, hopelessness, thoughts of suicide, and loss of pleasure in activities are probably the most useful in diagnosing depression in people with cancer. Very few studies have examined the presence of depression as well as the factors that could predict it in Nigerian breast cancer patients, which is what this study was set to examine. Purpose of the study The purpose of this study was to determine the presence of depression in breast cancer patients and to determine if cancer stage, marital status, average monthly income, occupational status, being informed about the kind of cancer, average annual cost of treatment and educational level could predict depression in this group of patients. Methods Procedure The research proposal passed through ethical review boards the approval of which was submitted to the Head of Department of the Cancer Screening Centre at Lagos State University Teaching Hospital (LASUTH) where permission was granted for the researchers to have access to the patients. Patients that qualified to take part in the study were female adults with histology reports showing that they had breast cancer. A purposive sampling of the total population of breast cancer patients who were willing to participate in the study was used in selecting participants. On each clinic days, the researchers explained the purpose of the study to the patients in the waiting room and they were informed that participating in the study was a voluntary exercise that would not affect their treatment in the hospital in any way. Participants were assured of the confidentiality of whatever information they divulge. The 33 participants who agreed to take part in the study were given the informed consent form to fill as well as the research instrument. The patients returned the instrument immediately after filling it. Instrumentation The main instrument used in this study was the Beck’s Depression Inventory II (BDI-II) to which was attached a section assessing certain characteristics of the respondents that could serve as a basis for comparison among the breast cancer patients such as age, educational status, marital status, cancer stage, monthly income, average annual cost of treatment and a question on whether they were well informed about breast cancer. The BDI-II was used to determine the level of depression in people living with breast cancer. The BDI-II is a 1996 revision of the BDI13, developed in response to the American Psychiatric Association’s publication of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, which changed many of the diagnostic criteria for Major Depressive Disorder. The BDI-II is a self-rating scale that contains 21 questions. Each of the 21 items has a list of four statements arranged in increasing severity about a particular symptom of depression ranging from 03, with 0 indicating no problem at all and 3 indicating the most severe condition. The maximum obtainable score is 63 and the minimum obtainable score is 0. The higher the score the more depressed the patient. 0 to 13 = minimal depression, The BDI-II is positively correlated with the Hamilton Depression Rating Scale with a Pearson r of 0.71, showing good agreement. The test was also shown to have a high one-week test–retest reliability (Pearson r =0.93), and high internal consistency (a =.91)14. The instrument was validated in English language amongst cancer patients in the University College Hospital (UCH) Ibadan, Nigeria and found to have a coefficient alpha of .8740 and a one week test-re-test reliability of Pearson r =0.60. A few of the respondents who showed interest in participating in the study could only speak Yoruba language (which is a common means of communication in Lagos State and other western parts of Nigeria) so the items on the BDI-II were orally translated into Yoruba and their responses ticked for them. Result The participants had an age range of 33 to 96 and a mean age of 50.73. Of the respondents, 58.1% were adequately informed about breast cancer, while 41.9% were not informed about breast cancer. Furthermore, 60.6% of the respondents were currently unemployed while 39.4% were currently employed. 21.3% had no formal education, 42.4% had secondary school education and 36.3% had tertiary education. 87.9% of the respondents were currently married, 9.1% were currently unmarried and 3% was currently unmarried but in a relationship. [Table - 1] shows that of the 33 patients in the study, 39.4% experienced minimal depression, 36.4% experienced mild depression, 9.1% experienced moderate depression and 15.2% experienced severe depression. [Table - 2] shows that educational level (Beta = .590, t = 3.229 , df = 24 p< 0.05), cancer stage (Beta = .565, t = 3.013 , df = 24, p< 0.05), being informed about type of cancer (Beta = .377, t = 2.168 , df = 24 p< 0.05) and average monthly income (Beta = .348, t = 2.031 , df = 24 p = 0.05) significantly predicted depression in women with breast cancer. Age, marital status, occupational status and average annual cost of treatment did not contribute significantly to the prediction of depression in the respondents. Discussion The result of the first research question confirms the presence of depressive symptoms in Nigerian breast cancer patients. This is similar to the findings of other studies of symptoms of psychological distress in cancer patients4, 6,15. The second research question showed that educational level, being informed about type of cancer, cancer stage, and average monthly income significantly predicted depression in women with breast cancer. In this study educational level and being informed about breast cancer could have predicted depression in breast cancer patients because the more educated an individual is the better able he or she will be in sourcing information about a variety of issues including health related issues like breast cancer. Studies have demonstrated that women with breast cancer ideally prefer to receive information about the disease and its treatment from their physician16. The surgical consultation about the diagnosis of breast cancer and its treatment is often understandably an upsetting time for women. It is opined that empowering women with knowledge about their treatment options and possible side effects would further help reduce depressive symptoms in breast cancer. More than the giving of information however, how the information is presented is also very important especially when prognosis is poor. The insensitive manner in which patients are sometimes informed about their condition could serve as a source of heightened emotional distress in breast cancer patients. The finding in this study that cancer stage predicted depression is supported by studies17,18 whose findings opined that advanced disease is a risk factor for depression. This is likely to be so because having advanced cancer is often associated with increased level of pain and higher level of existential concerns related to fear of death or fear of being abandoned when the financial and psychological cost of care becomes unbearable to friends and relatives. Average monthly income significantly predicted depression in this study. This is supported by the study by Fagbenle, et al19, where they opined that in Nigerian cancer patients psychological distress is often linked with high cost of treatment in the face of economic impoverishment and having to travel long distances in order to receive quality treatment. An individual’s average income would determine how much would be available to pay for treatment and other associated cost. Occupational status, that is being currently employed or unemployed did not predict depression in breast cancer patients in this study. Being employed generally has beneficial effects on psychological health: it brings interest, income, fulfilment, social contacts, and status, and provides structure and a sense of control20, 21. Studies have shown that the advantages of employment are weaker in married women22, 23, more so if they have children24, 25, most so when the children are of pre-school age26. Fulltime employment is particularly demanding27, 28 especially when coupled with health challenges. Occupational status not predicting depression in cancer patients in this study could be as a result of social support received from friends and relatives by patients towards offsetting some of their medical bills as only 39.4% of the participants were currently employed while 60.6% were currently unemployed. This could also account for why average annual cost of treatment did not predict depression as most of the patients do not even know how much they have spent though they agree that they have spent a lot. Often, payment for treatments are done by family members and other caregivers, who are often the ones laden with the responsibility of going around to buy and pay for all that is needed for treatment of the patients. The finding that marital status did not significantly predict depression is unlike the findings in similar studies which indicated that people who are married are less likely to develop depression than single people18, 29. However, other studies noted that marital status has different associations with affective disorder in women from different cultures30, 31. Conclusion This study has confirmed the existence of depressive symptoms in breast cancer patients and also reported that knowledge, educational level, average monthly income and cancer stage predicted depression in breast cancer patients. Five percent of breast cancer patients in this study experienced severe depression, which underscores the need for psychological interventions to be developed in order to help cancer patients experiencing depression and other forms of psychological distress to overcome emotional challenges brought about by a cancer diagnosis. Acknowledgement The study participants are appreciated for their cooperation in filling the questionnaire during the course of data collection. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11076t2.jpg] [hs11076t1.jpg] |
| |||||||||

{kind=link}
{kind=link}