 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
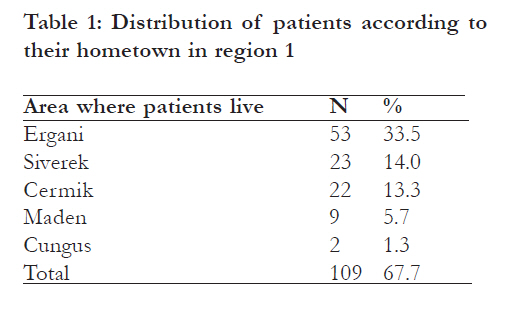
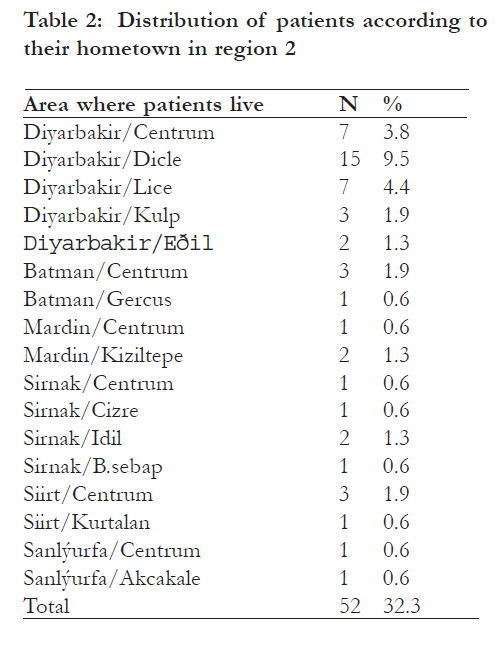
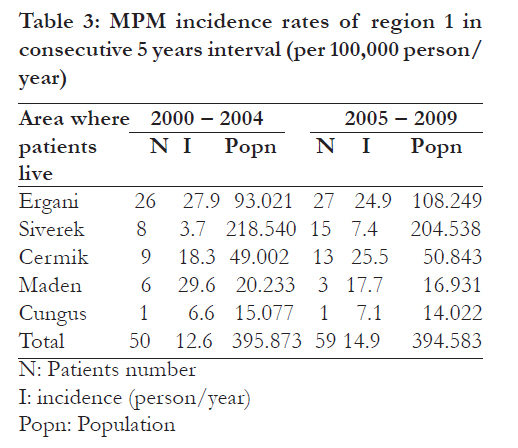
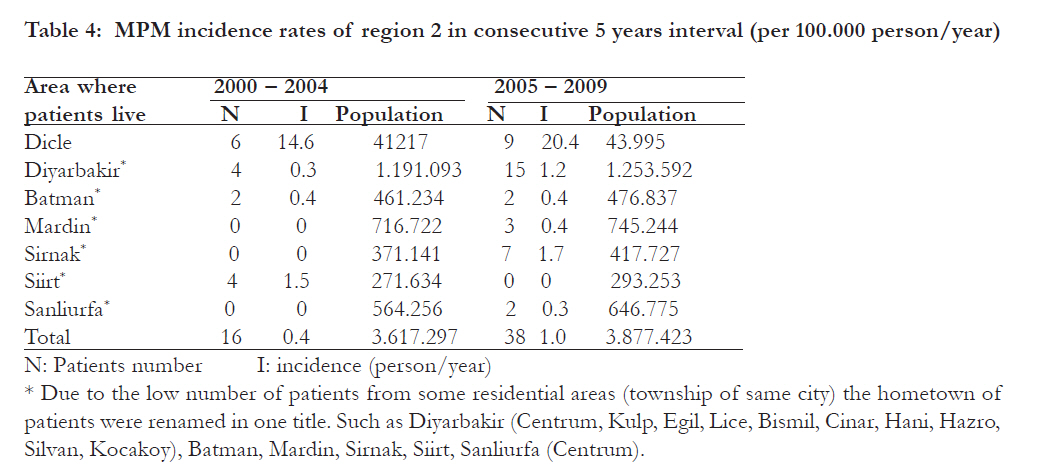
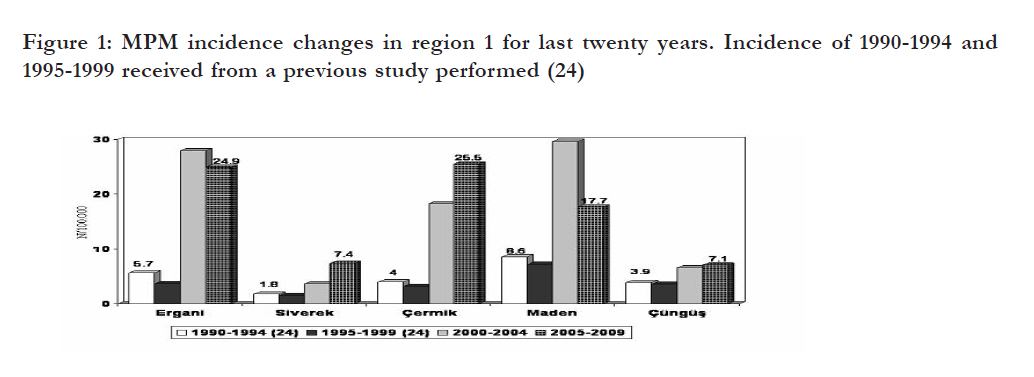
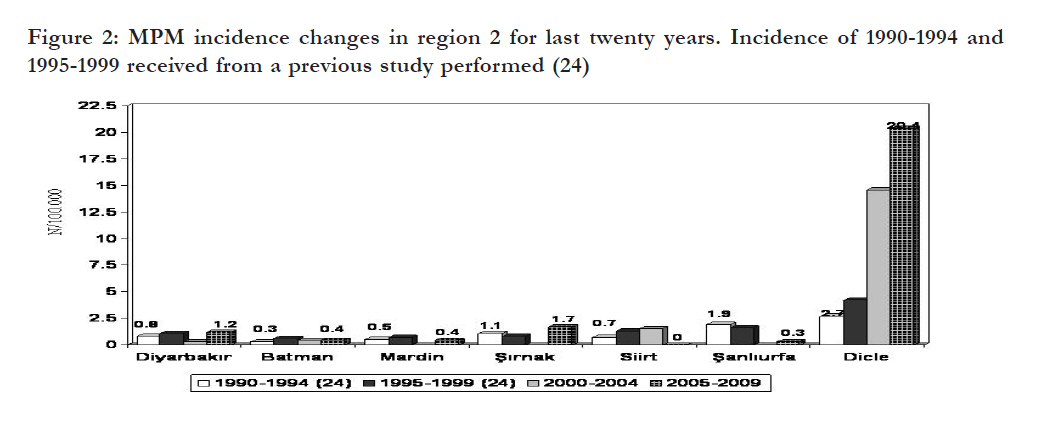
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 346 - 352 The incidence of mesothelioma has not decreased for the last twenty years in Southeast region of Anatolia Carkanat AI1, *Abdurrahman A1, Abakay O2, Cengizhan S1, Selimoglu SH1, Senyigit A1 1Department of Chest Disease, Medical Faculty, Dicle University, Diyarbakir, Turkey, 2Department of Chest Disease, Education and Training Hospital, Diyarbakir, Turkey Code Number: hs11077 Abstract Background: Malignant pleural Mesothelioma (MPM) is a very rarely encountered tumor in the normal population. Malignant pleural Mesothelioma (MPM) is a type of cancer originating from the mesothelial cells of mesothelium that is a serous membrane lining pericardium and tunica vaginalis as well as pleura and peritoneum. Most significant cause in its etiology is exposure to asbestos1. The risk of MPM is proportional to exposure to asbestos; the risk increases with the increase in exposure dose and with prolongation of the period after the first exposure (latent period)2. Exposure with asbestos or erionite begins at birth in rural areas. In that case, ‘latent period’ is the period up to the age where the disease is diagnosed and this period is around the ages of 5055 years in our the patient series of our country. In terms of latent period this is longer compared to patient series of occupational exposure, however, it is shorter in terms of the age at which the disease is diagnosed3-5. It is stated that the male/female ratio of MPM patients in industrialized countries is between 3/1 – 10/16,7. On the other hand, as the lifestyle of women and men are the same in rural areas the risk is shared equally, which means, the male/female ratio in the relevant patient series is around one3,5,8. The MPM prognosis is generally poor. In wide patient series survival it is approximately reported around 12 months9-12. This MPM is a very rarely encountered tumor in normal population. Its frequency in a population with no defined asbestos or mineral fiber exposure is reported to be between 1-2,2 in a million annually. This condition is also known as “background mesothelioma rate” in the literature2,13. Average annual incidence rate of MPM all around the world is reported to be 1.3/100,000 person-year for males, and 0.2/100.000 person-year for females 4,13,14. Three-thousand patients with MPM are diagnosed yearly in the United States of America. Annual incidence rate is 11/1,000 000 person-year for the general population14-16. Annual number of MPM patients identified in Britain is around 1000. Average annual MPM incidence rate in Australia is 6.6/100.000 for males, 0.7/100.000 person-year for females in normal population, and relative death rate from MPM in persons having direct exposure with asbestos is reported to be between 3.9% and 6 %17,18. The incidence rate in our community is not exactly known. However, according to the data fromÝzmir Cancer Record Center accepted by World Health Organization, the average annual mesothelioma incidence rate in the Aegean Region is 0.7/100,000 person-year for males, and 0.3/100.000 person-year for females19. In cohort studies conducted in the villages around Eskisehir, a city known to have an exact environmental exposure, the average annual MPM incidence rate was found to be 114.8/100,000 person-year for males, and 159.8/100.000 for female population20. These incidence rates are around or even higher than some of the incidence rates detected in the cross-sectional studies on employees having direct exposure with asbestos held at other regions in our country. The death rate due to MPM has been reported as 5.6% in the same study20. These rates show the degree of risk in the population having environmental exposure with asbestos. Similar environmental exposure results are reported from Greece, Corsica, Cyprus, Bulgaria, France and Yugoslavia2,21. The aim of this study was to search the changes in incidence MPM disease in the last decade in our region which has extensive asbestos deposits, and to study the factors affecting this change. Methods A total of 161 MPM patients diagnosed between January 2000 and December 2009 at Dicle University Hospital were included to the study. The patients’ charts were retrospectively evaluated. Data about age, sex, hometown, and initial complaint of the patients were collected from the charts. Mode and duration of asbestos exposure were also recorded. Asbestos exposure-related medical records of patients were thoroughly indentuified from their charts. Asbestos anamnesis was noted down in persons currently living or who previously lived in Cermik, Cungus, Ergani and settlements of Diyarbakir city, Maden district of Elazig city, and Siverek district of Sanlýurfa city, where direct exposure with asbestos was reported formerly. These places were labeled as Region 1. The previous locations (particularly places of birth) of cases coming from areas like Batman, Mardin, Sirnak, Sanliurfa, Siirt, Diyarbakýr center and other districts, where no exposure with asbestos was reported, were taken into the group “cases with no previously detected direct exposure with asbestos” and named as Region 2 in [Table - 1] and [Table - 2]. The methods used for the patients’ diagnoses were carefully noted from the charts. Closed pleural needle biopsy by using Ramel needle biopsy set was done as the first method for diagnosis in patients with pleural fluid. For cytological examination thoracentesis was performed in the cases with pleural effusion. Pleural biopsy under ultrasonography guidance was performed to the patients having low pleural fluid. Tissue samples taken by means of pleural biopsy were immediately placed in 10% formol and sent for histopathological examination. Various special stains, particularly Periodic Acid Shiff (PAS) were applied in order to distinguish MPM from adenocarcinoma and other possible diagnoses in histopathological terms. All cases were analyzed in three groups as right, left and bilateral lesion localizations. Video-assisted thoracoscopic surgery (VATS) was performed for the cases that we were unable to diagnose by using pleural biopsy or cytological examination of the fluid. In a few patients, that VATS was inconclusive and thoracotomy was performed for the diagnosis. Incidence was calculated by multiplication of the ratio of new cases to the population where the cases were living by 100,000. Populations of the settlements were determined from the national census done in 2000 and from the address-based census done in 200822. The 2000-2009 settlement populations were separately calculated by a projection technique using population increase-decrease rates. The population to be used for the 2000-2004 incidence calculation was achieved by dividing the total population of these five years to five. The 20052009 incidence calculation was carried out in a similar manner. Incidence rates in 100,000 individuals of these settlements were calculated in this way. Five-year incidences (2000-2004 and 20052009) of the MPM patients in the areas known with asbestos exposure and in the areas with unknown direct asbestos exposure were calculated and are presented in [Table - 3] and [Table - 4]. Statistical analysis Percentage distributions, average values and incidences were calculated by using SPSS 11.5 software. Results Sixty four (39.8%) of the 161 patients were female and 97 (60.3%) were male. The Male/Female ratio was found as 1.54/1. The Mean age in females was 54.4 ± 13.5 (22-85) years and 55.5 ± 12.7 years (1982) in males and 55.1 ± 13.1 years in the total study group. Symptoms and signs of patients were as follows; 129 (80.1%) patients had dyspnea, 111 (68.9%) patients had loss of weight, and 99 (61.5%) patients had chest pain. A total of 127 (78.9%) of the patients had exposure toasbestos. All asbestos exposures were in the environmental exposure. Average asbestos exposure duration was 30.8 ± 16.1 years. The hometowns of the patients are given in [Table - 1] and [Table - 2]. The diagnosis was made with closed pleural biopsy in 121 (75.2%) patients, video-assisted thoracoscopy in 32 (19.9%) patients, pleural fluid cytology in 5 (3.1%) patients and thoracotomy in 3 (1.9%) patients. Mesothelioma type was determined in 155 patients, of these, 119 (73.9%) were identified as epithelial, 20 (12.4%) as mixed type and 16 (9.9%) as sarcomatous type of MPM. A total of 100 (62.1%) patients had right-side involvement, 51 (31.6%) had left-side involvement and 10 (6.3%) had bilateral involvement. The 109 (67.7%) patients were from Region 1 and 52 (32.3%) from the Region 2. The MPM incidence in the last decade was calculated to be 3.9/ 100,000 person-year in the overall. The incidence rate between the years 2000 and 2004 in Region 1 was 12.6/100,000 person-year and was 14.9/100,000 person-year between 2005 and 2009. In Region 2, 2000-2004 incidence rate was 0.4/ 100,000 person-year and 2005-2009 incidence rate was 1.0/100,000 person-years [Table - 3] and [Table - 4]. Twenty eight patients were diagnosed in 2008, nineteen in 2007, twenty in 2009, fifteen in 2003 and 2006 years, fourteen in 2001 and 2002, twelve in 2000, eleven in 2005 and ten patients in 2004. It is found that the numbers of patients increased in the last three years. Discussion Yazýcýoglu et al., reported for the first time in the region that asbestos-soil is used as plastering material and whitewash and therefore, THE MPM rate in the region was high23,24. In other MPM studies carried out in the region, asbestos exposure rateS in these patients wERE 60-65%, and this exposure generally took place in the form of environmental asbestos exposure (i.e. processing and sale of asbestos-soil for plastering and whitewash)25, 26. Environmental asbestos exposure rate in our study was found to be 79%. The reason of higher asbestos use in our study is thought to be due to new settlements using asbestos, and more common use of this material in houses. In areas formerly identified to be consuming asbestos, people were mining asbestos from the surrounding mountains and hills, and making it ready for use by processing the material with water by themselves or with their partners. Moreover, they sell this material to make money. The male/female ratio in our patients was found to be 1.54/1. Other studies reported similar male/female ratios25,27. Some studies carried out in the region also found similar male/female ratios like 1.126. Environmental exposure begins at birth and the exposure is continous. The latent period between MPM formation and beginning of the exposure with asbestos is approximately 20 – 40 years2,21. The age group of patients in our study is younger than other studies since it was due to environmental exposure. In other MPM series related to environmental exposure with asbestos age usually ranges between 50 and 55 years of age3-5, 25,25. The most common complaints of MPM patients are known to be dyspnea and chest pain. Dyspnea occurs due to the restriction caused by pleural fluid or pleural thickening. The pain generally occurs in the side wall of chest and has a spreading and an obtuse nature. The symptoms prevailing among our patients are dyspnea, chest pain and weight loss. These symptoms are in accordance with the current data in the literature5,13,28. In our study, epithelial type frequency was higher, though sarcomatous and mixed types were lower compared to the data present in the literature29,32 . Our overall MPM incidence was calculated as 3.9/100,000 person-year. Yazýcýoðlu et al., calculated this rate as 5/100,000 person-year23, and Þenyiðit et al., found it as 4.3/100,000 person-year25. No considerable change in the MPM incidence of the overall of our region was spotted. In a similar study carried out in Eskisehir and its neighborhood, known to have environmental asbestos exposure, MPM incidence rates were found to be higher than our results20,33. Again, in another study conducted in Cappadocia region, MPM incidence rates was found to be 220 -800/100,000 person-years34. The MPM incidence rate is higher in the vicinity of Cappadocia due to the use of erionite material, which is a non-asbestos fibrous zeolite and a more potent carcinogen than asbestos20,33,34. When we look at the recent incidence study findings in the region, MPM incidences showed an increase in five settlements formerly detected to have exposure to asbestos24,25 ([Figure - 1] and [Figure - 2]). The MPM rates in these regions were also at high levels in the first MPM studies carried out in our region22,23. Two thirds of our patients were coming from the settlements having asbestos exposure. If we consider that exposure with asbestos was detected in Dicle district, about 80% of our patients are coming from these areas. However, the previous incidence data showed that; 59.7% of the patients were coming from areas using asbestos24. Incidence rate increased in the asbestos using areas during these two decades and this proved that preventing asbestos use is far from the desired levels. In a study carried out in the region, asbestos users are found to have insufficient knowledge about the issue35. We suggest that socio-economic measures and education would help to fight asbestos use in these settlements. A total of 32.3% of our patients are coming from areas formerly not associated with asbestos exposure, and incidence rates were not shown to be increased in these regions according to other recent studies25,26. However, the incidence rates in Diyarbakir city, Dicle district is found to be ten times bigger than 1990-1994 years’ MPM incidence rate. It has been reported that asbestos use in this area is in the form of whitewash in houses just like Ergani and Cermik districts of Diyarbakir city. Besides, MPM incidence rate increase in Dicle is also found in the publication released in the region25. Incidence rates have shown a decrease in places without asbestos exposure other than Dicle district. We think that making a soil analysis and a research on the asbestos content of the district will be useful. Moreover, it will be good to examine whether this material was used in the houses in Dicle district. Probably asbestos-soil is mined in all these regions and used by the locals. It is particularly estimated that the use of asbestos-soil, known as ‘white plaster’, has decreased with the utilization of lime as a plastering material in many regions. Incidence figures in all settlements did not show an increase, but the incidence rate in areas formerly detected to be using asbestos rose. The rates of. abandoning asbestos use are not at the as desired levels. When the latent period required for MPM formation in these regions is taken into account, the incidence rate of the diseasecan be predicted to increase or at least to stay at the same level in the following two or three decades. The number of patients has shown an apparent increase in the last three years. This is more distinctive compared to other recent studies25,26. The reason for this is the climactic point of asbestos use in the region and it is wide use in the settlements. In addition, this makes us think that the use of asbestos in the region is at highly dangerous levels and particularly education studies and socioeconomic measures should be taken to prevent this situation. Conclusion Most of the patients in our study are coming from areas found to have a previous exposure to asbestos. There is a need for instructing the people living in these areas having asbestos exposureabout MPM and the biggest cause which is asbestos. Education programs should be more frequent and research drawing attention to the asbestos use habit of these people should be conducted. Additionally, it is necessary to create a detailed asbestos map in the region (especially in Diyarbakir). Broad field studies to identify etiology are required in these settlements in order to reduce the risk of MPM. Soil samples should be widely collected and analyzed in these regions. Further more, we suggest that microfilm scanning might be useful in settlements of regions having positive soil analysis results. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11077f1.jpg] [hs11077f2.jpg] [hs11077t3.jpg] [hs11077t1.jpg] [hs11077t4.jpg] [hs11077t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}