 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
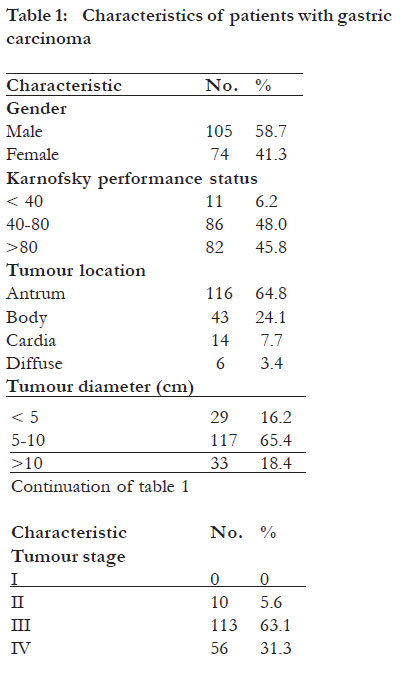
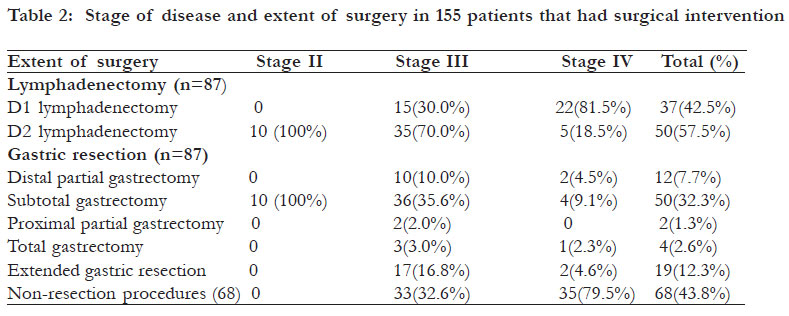
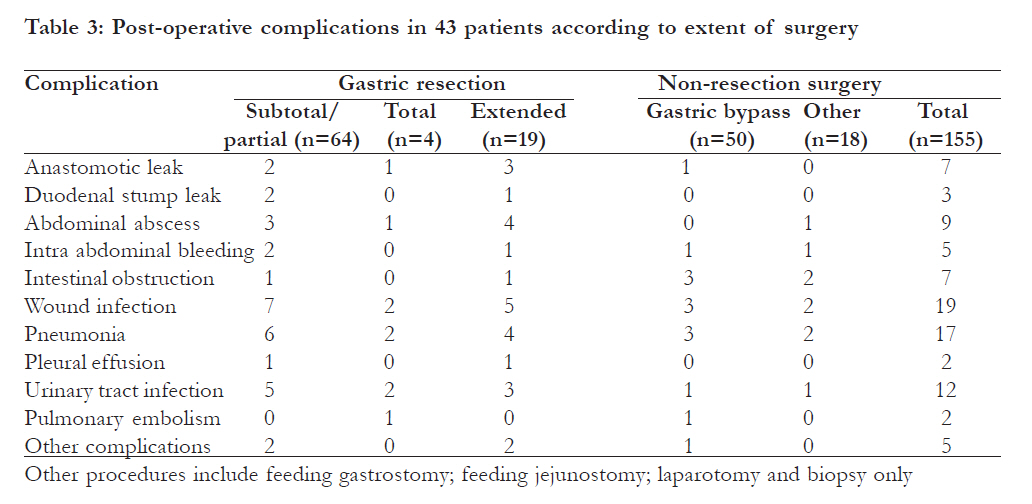
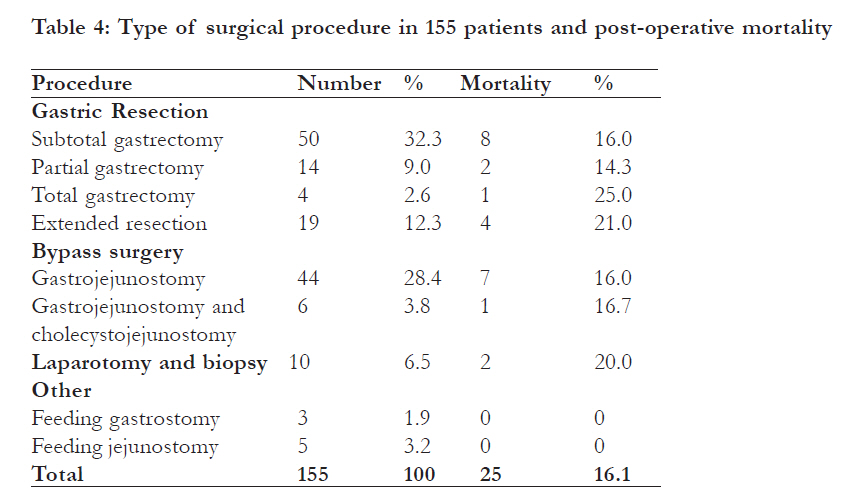
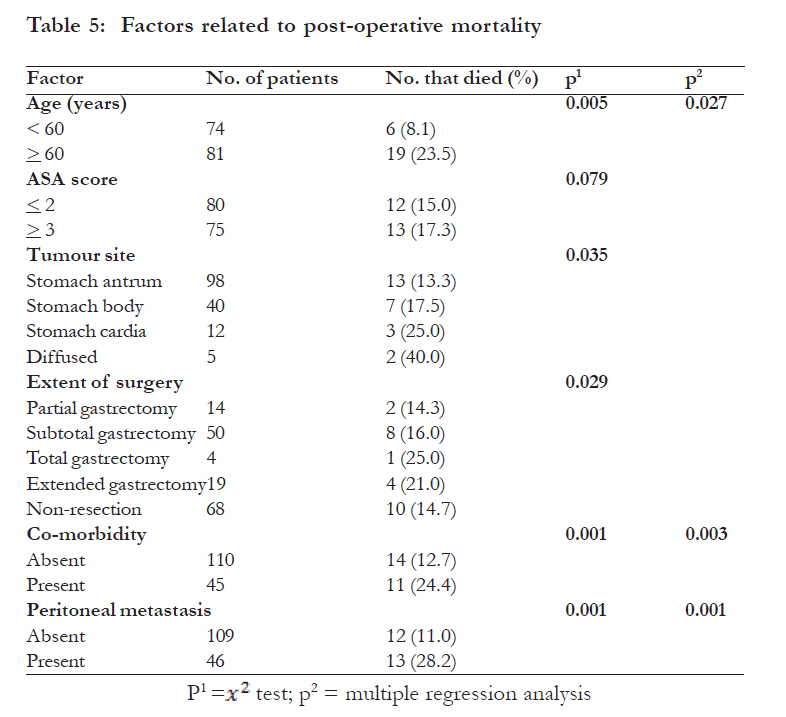
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 353 - 361 Management and outcome of gastric carcinoma in Zaria, Nigeria *Ahmed A, Ukwenya AY, Makama JG, Mohammad I Division of General Surgery, Department of Surgery, Ahmadu Bello University Teaching Hospital, Zaria, Nigeria Code Number: hs11078 Abstract Introduction: Gastric cancer is the second leading cause of cancer death in the world. The objective of this study was to present the clinical evaluation, treatment and outcome of 179 patients with gastric carcinoma in Zaria, Nigeria. Key words: Gastric cancer; Treatment; Gastrectomy; Morbidity; Survival Introduction In the past, gastric cancer (GC) was the second most common cancer in the world. 1, 2 Incidence is highest in Japan, South America and Eastern Europe3. In high income countries however, the incidence of GC has declined. In Britain the age-standadised incidence rates for males have more than halved from 31.0 per 100,000 in 1975 to 13.3 per 100,000 in 20064. Similar reports have been made from other high income countries5-7. In spite of decreased incidence of GC in Western countries, it remains the second most common cause of cancer death in the world8,9 . Gastric cancer has a low prevalence in sub-Saharan Africa with the lowest incidence rates in Western Africa4,10,11. The highest prevalence is in the stomach cancer region comprising Rwanda, Burundi, South Western Uganda and Eastern Kivu province of Democratic Republic of Congo12,13. The incidence of GC is increasing in sub-Saharan Africa. A report from an endoscopy service in Ile-Ife Nigeria described 102 patients with GC seen within four years14. Another report from Kenya showed an incidence of 7.01 per 100,000 males and 3.7 per 100,000 for females with a 10-fold increase incidence between the periods 1965–70 and 1991–93 respectively15. In low income countries patients with dyspeptic symptoms are managed solely based on clinical examination because radiological and upper gastrointestinal endoscopic facilities are not available. These patients present later with advanced GC which may be unresectable or relapse after complete resection. There are differences in morbidity and mortality rates associated with the different extents of GC surgery, although they are all commonly denoted as radical resection.16-18 The D2 lymphadenectomy is recommended by the Japanese Surgical Society as the surgical treatment for gastric cancer but its performance has not gained popularity worldwide, since it is associated with higher mortality and morbidity and does not offer much survival benefit over D1 lymphadenectomy.19-21 While a limited lymph node dissection may compromise the chance for cure or prolonged survival, the extent of surgery does not improve the overall survival and postoperative complications are significantly related to it.16,20 In sub-Saharan Africa patients present with advanced disease often complicated by gastric outlet obstruction, haematemesis or perforation.22-24 In addition, many patients also have significant comorbidity and a poor level of overall fitness.11,22 Therefore, the extent of surgery should consider not only the benefits of treatment and long term survival but also the operative risk and quality of life. Our approach has been to provide optimum surgery by balancing risk and radicality with variable lymphadenectomy and preservation of the spleen and pancreas according to the location of the tumour, its stage and the patient’s condition. There is paucity of information on the detailed treatment and outcome of gastric cancer in sub-Saharan Africa. The objective of this study was to present the clinical evaluation, treatment and outcome of 179 patients with gastric carcinoma seen between 1995 and 2009 in a tertiary health centre in Zaria, Nigeria. Methods Patients that presented with gastric carcinoma from 1995 to 2004 were reviewed retrospectively while those managed from 2005 to 2009 were reviewed prospectively. Only patients with gastric carcinoma were included. Diagnosis of GC was based on barium meal, oesophagogastroduodenoscopy and biopsy. Other investigations performed include abdomino-pelvic ultrasound, biochemical and haematological assessments. The CT scan and assessment for Helicobacter-pylori were also done. All patients had histological diagnosis of gastric carcinoma. For staging of the tumours, the TNM classification system according to the AJCC staging was used. 25 For the retrospective study, information was obtained from case notes of the patients, operation records and discharge summaries. This was entered into a standardised data extraction form designed for the study. From 2005 to 2009, data were prospectively entered in to a profoma specifically designed for the study. The subjects gave written informed consent to the study protocol which was approved by the institutional ethical review committee. Surgical treatment The extent of resection was planned based upon pre-operative and intra-operative staging balanced against the age and fitness of the patient. Patients were offered D1 lymph node dissection by excision of all N1 (peri-gastric) lymph nodes if at laparotomy. No lymph node, hepatic, or peritoneal involvement were found. The D1 was also performed in high risk elderly patients (ASA III or IV) and those with widespread metastatic disease. Physically fit patients with locally advanced disease had D2 lymphadenectomy which required the removal of peri-gastric lymph nodes and those along the left gastric, hepatic, splenic and coeliac arteries, the anatomic N2 according to the classification of the Japanese Research Society for the Study of Gastric Cancer 19. The spleen and pancreas were preserved except when directly invaded by tumour. The performance of total or subtotal gastrectomy was determined by the size of the tumour, its position on the stomach and the ability to achieve a 5cm tumour free margin. Adjacent organs directly involved by tumour were resected in appropriate cases. Adjuvant chemotherapy consisting of epirubicin, cisplatin and 5-fluorouracil was given to some patients based on availability. Extent of gastric resection Tumours located in the distal or middle third of the stomach were treated with an 80% subtotal gastrectomy with a palpable 5cm tumour free margin. A limited partial (50%) gastrectomy was performed in high risk patients and those with advanced disease unlikely to benefit from radical surgery. Reconstruction following gastrectomy was by antecolic gastrojejunostomy. In patients with proximal tumours a proximal subtotal gastrectomy was done creating a gastric tube and a pyloromyotomy because of the inevitable vagotomy. Total gastrectomy with Roux-en-Y reconstruction was performed in tumours that were diffused. Patients with surgically unresectable or metastatic disease were offered nonresection operations including gastrojejunostomy, jejunostomy and laparotomy and biopsy only. Statistical analysis Patients were assessed from time of treatment until death or loss to follow-up. Frequencies, means and standard deviations were determined. Distributions were compared with unadjusted log-rank test. Comparison of categorical data employed student ’s t-test for groups and Fisher’s exact test for proportions. Logistic regression was used to identify clinicopathological variables associated with mortality and morbidity. The cumulative rate of survival data was measured using Kaplan-Meier method. All calculations were performed using the Statistical Package for Social Sciences (SPSS) software program, version 17.0 (SPSS Inc., Chicago, IL, U.S.A.) and results were considered statistically significant when the P value was <0.05. Results Patient’s characteristics Overall, there were 179 patients. Thirty nine (21.8%) patients were seen in the first five years of the study while 57 (31.8%) and 83 (46.4%) were managed during the second and third five years respectively. There were 105 males and 74 females; with a male: female ratio of 1.4:1 [Table - 1]. Their ages ranged from 21-89 years, with a mean of 51 ±6.3SD. Fifty four (30.2%) patients were <40 years while 93 (52.0%) were 40-60 years. Duration of symptoms ranged from 2 weeks to 3 years, with a median of 9 months. In 106 (59.2%) patients the tumour was palpable at presentation. Sixty nine (38.6%) patients presented with complications comprising 44 gastric outlet obstruction, 5 eosophageal obstruction, 15 bleeding and 5 perforation. Forty five (25.1%) patients had additional medical diseases including hypertension and diabetes mellitus in 36 and 15 of them respectively. Ten (5.6%) patients presented with early gastric cancer (EGC) while 76.0% and 18.4% had T3 and T4 respectively. In 7 (4.0%) patients only N1 lymph nodes were involved while 71.0% and 25.0% had N2 and N3 involvement respectively. In 18(10.1%) and 24(13.4%) patients there was liver and peritoneal metastasis respectively while 10 (5.6%) had both. Chemotherapy was administered to 57 (31.8%) patients including 38 that had gastric resection. Operative data One hundred fifty five (86.6%) patients had surgical intervention including gastric resection in 87 (56.1%) [Table - 2]. Subtotal gastrectomy was performed in 50 patients while 14 had partial gastrectomy. The remaining 23 patients comprised of total gastrectomy (n=4) Resection of stomach and adjacent organs grossly involved by tumour (n=19). The resected organs include colon 13, spleen 6, distal pancrease 4 and gall bladder 2. Of the 87 patients that underwent gastric resection, 50(57.5%) had D2 lymphadenectomy comprising 35 with distal subtotal gastrectomy and 15 with partial gastrectomy. The remaining 37(42.5%) patients had D1 lymphadenectomy. Of the 50 patients with stage III disease that had gastrectomy, 35(70%) had D2 lymphadenectomy compared to 18.5% of 27 patients with stage IV disease. Twenty five (28.7%) gastrectomies were deemed curative by excising all macroscopic disease leaving histologic margins free of tumour (R0). In 51(58.6%) and 11(12.7%) there was microscopic (R1) and macroscopic (R2) residual disease respectively. Outcome of treatment Postoperative complications seen in 43 (27.7%) 7.39), presence of pre-operative comorbidity (OR patients are shown in [Table - 3]. Univariate analysis 1.55, CI 1.09 - 12.83), resection of adjacent organs showed that age (p< 0.01), sex (p<0.01), extension (OR 4.26, CI 2.5 - 7.75) and D2 lymphadenectomy of resection (0.001), extent of lymphadenectomy (OR 2.76, CI 1.63 - 4.19) as independent predictors (p<0.04) and preoperative comorbidity (0.01) were of postoperative morbidity. Nine patients significantly associated with postoperative morbidity. underwent reoperation for colonic anastomotic Multiple regression analysis identified older age (odds breakdown (n=3), duodenal stump leak (n=2) and ratio (OR) 3.75, 95% confidence interval (CI) 1.52 -intra-abdominal abscess (n=4). Twenty five (16.1%) patients died postoperatively, by improved Karnofsky performance status(KPS), including one of 25 (4.0%) that had curative resection control of vomiting and reduced pain. The median [Table - 4]. Following logistic regression analysis, the hospital stay was 13 days (ranged from 8-62 days). factors associated with mortality were presence of Patients that developed postoperative complications peritoneal metastasis (p<0.001), pre-operative had a longer hospital stay. Follow-up ranged from 2 comorbidity (p<0.01) and age more than 60years to 94 months, with a median of 10.5 months. Seventy (p<0.03). Of the 24 (13.4%) patients that did not three (47.1%) patients were followed-up for two have surgical intervention 5 died on admission. years, while 29.0% and 10.7% were followed up Overall, 124 (80.0%) patients had significantly for 3 and 5 years respectively. improved quality of life postoperatively as evidenced by improved Karnofsky performance status(KPS), control of vomiting and reduced pain. The median hospital stay was 13 days (ranged from 8-62 days). Patients that developed postoperative complications had a longer hospital stay. Follow-up ranged from 2 to 94 months, with a median of 10.5 months. Seventy three (47.1%) patients were followed-up for two years, while 29.0% and 10.7% were followed up for 3 and 5 years respectively. The overall median survival was 13.6 months. The and total gastrectomy were 17.2 (95%CI; 5.1-21.0) median survival time after gastric resection was 15 and 6.0 (95% CI; 2-9) months respectively (p<0.01). months (95% CI; 7.7- 20.4) compared to 6 months Overall, 70.1% of patients that had gastrectomy (95% CI; 2.1-7.3) following non-resection surgery survived one year while 49.4% and 21.8% survived (p< 0.01). Of the 25 patients that had curative 2 and 5 years respectively. Using multiple regression resection 14(56.0%) were alive 5 years after surgery. analysis, the factors that significantly affected survival Resection of contagious structure did not offer were patient age (0.03), tumour location (0.01), survival benefit over gastrectomy alone (p>0.59). presence of peritoneal metastasis (0.001), histological The median survival for distal sub-total gastrectomy type (0.01) and medical conditions (0.001) [Table - 5 ]. Discussion This study revealed an increasing prevalence of gastric carcinoma in our institution. The patients present with advanced disease and often have significant comorbidity and a poor level of fitness. In 64.8% of patients the tumour was located in the gastric antrum. Surgical intervention was carried out on 155 (86.6%) patients including gastrectomy in 56.1%. Gastric resection was associated with high morbidity and mortality. However, it was the only potentially curative treatment associated with long term survival. In Nigeria, GC accounts for 1.1-6.0% of all cancers, the incidence being higher in the Southern than the Northern parts of the country.11,22 In this study there was increased prevalence of GC similar to other reports from our sub-region.26,27 This may be due to increased access to diagnostic facilities or to a true increase in incidence. The peak age of incidence was the fifth decade which had been noted in previous studies.11,25 This is about a decade earlier than in high income countries probably because of the younger age of our patients. In the present study the median duration of symptoms was nine months and most patients were treated for peptic ulcer or dyspepsia solely based on clinical examination. The poor correlation between clinical and endoscopic findings in patients with dyspepsia necessitates regular endoscopic evaluation and careful follow up in the management of these patients.12,14 Although fibre optic gastroscopy has been available in our institution since 1977, its use has been mainly to confirm the diagnosis of GC since those examined were referred to the hospital with established symptoms.25 For this reason 94.4% of our patients presented with advanced disease similar to other reports from low income countries.12,15,26 The number of EGC has increased in recent years due to improved diagnostic facilities. In Korea the proportion of EGC increased from 28.6% in 1995 to 47.4% in 2004 whereas in Japan EGC is diagnosed in about 50% of patients due to mass screening.28 In the present report 5.6% of patients had EGC compared to none previously reported from our institution.25 A recent report from an endoscopy unit in Nigeria identified 102 GC cases between 1999 and 2003 of which 50% were EGC.14 Our gastric resection rate of 56.1% compares favourably with 13% to 67% reported in other studies.22,23,.25 The presence of comorbidity and poor level of fitness in our patients increase the risk of postoperative complications and lowers patients’ ability to survive major complications when they occur. In the present study, D2 lymphadenectomy was carried out on fit patients with locally advanced disease. However, for optimal postoperative recovery and functional outcome, less radical surgery (D1) was performed on high risk and very old patients and those with wide spread metastatic disease. This prevents complications in those patients least able to tolerate them and in whom the potential survival benefit of more radical surgery would be minimal. A recent report from China revealed that in selected patients, morbidity and mortality were higher following D2 or D3 compared to D1 lymphadenectomy.29 Similarly, prospective randomized studies have revealed significantly higher postoperative morbidity and mortality rates and no 5- and 11-year survival benefit following D2 compared to D1 lymphadenectomy.30-32 As demonstrated in our selective approach, recently, Lamb P et al showed the safety of a tailored approach to gastric cancer surgery that balances risk and radicality which are associated with low mortality and satisfactory long-term survival.33 However, in Japan and other Asian countries more extended D2 and D3 lymphadenectomy are being performed for locally advanced GC and are associated with low mortality and improved long term survival.34-36 In our patients, peritoneal recurrence was the most common pattern of treatment failure indicating that adequate locoregional control was obtained by appropriate lymph node dissection. Following gastrectomy combined resection of other organs is not of long-term benefit and it significantly increased postoperative complications and mortality.25,37,38 Robert C G et al reported that the overall 5year survival rate for the 286 patients undergoing gastrectomy with additional organ resection was significantly less than the gastrectomy-alone group.39 In another study, postoperative complications in the spleen-preservation group and splenectomy group were 11.6% and 29.3%, respectively while the mean survival time was 72.0 months in the spleenpreservation group compared to 56.7 months in the splenectomy group.40 In the present study, spleen and pancreas were preserved unless they were directly involved by tumour. Postoperative complications seen in 27.7% of our patients compare well with other results.12,25,37 In keeping with other studies, the presence of comorbidity, resection of adjacent organs and extended lymphadenectomy were independently associated with complications.37,38,41 Surgical wound infection was the most common complication but was usually superficial and easily controlled by local wound care. Anastomotic leak was followed by intraabdominal infection which often caused peripancreatic abscess, and eventually pancreatic fistulas in some cases. These required additional operations which prolonged hospital stay and the cost of treatment. Improvement of surgical technique is therefore crucial to lower the occurrence of intra-abdominal haemorrhage and anastomotic leak while their prompt recognition and treatment would reduce the attendant mortality. In addition, prior treatment of preoperative comorbidity is essential to the postoperative recovery of patients with gastric cancer. The postoperative mortality following gastric cancer surgery is 1.7-16% in Western countries.42-45 Our post-operative mortality was 16.0% which is lower than 27.0% reported by Mabogunje et al from our institution and 23-36% reported from our sub-region.11,23,25,26 Older patient age, peritoneal seedlings and severe medical diseases were significantly associated with mortality. More frequent use of CT scan and laparoscopy will reduce the number of unnecessary laparotomy in patients with liver and peritoneal metastases which is associated with higher morbidity and mortality.32, 46 Anastomotic and duodenal stump leakage was the main cause of mortality following gastric resection, whereas disease progression was the most common cause of death following non-resection procedures. In the present study, 1-year survival of 70% following gastrectomy was better than other reports from our sub-region.12,25,26 This reflects decreased postoperative mortality and the use of chemotherapy for advanced disease.47 There was also an improvement in 5-year survival to 21.8% probably because of improved staging, patient selection for curative resection and decreased postoperative mortality. This is better than 0-14% reported from our sub-region but lower than 25-38.4% reported from Western countries and 66% from Korea.22,28,33 Gastric resection is associated with longer survival compared to all others treatments including by-pass procedures.34,48 In addition, the quality of life, assessed by relief of preoperative symptoms, was also better after resection than after gastrojejunostomy.49,50 In our experience, improved survival has been shown after resection even when localized liver metastases were present. This increased survival may be due to relief of obstruction and the prevention of bleeding. The inclusion of retrospectively collected data is a limitation in this study. More frequent use of CT scan and laparoscopy would have significantly reduced the proportion of patients that had unnecessary laparotomy (had biopsy only) which was associated with high morbidity and mortality. In addition, many patients that would have benefited from chemotherapy did not have it because of financial constraints. Therefore, the full potential effects of chemotherapy could not be assessed in our patients. Conclusion This study shows that patients with gastric cancer present with advanced disease. This would improve if patients with dyspepsia are regularly evaluated with oesphagogastroduodenescopy and closely followedup during treatment. Treatment of GC patients should be based on a reasonable choice of operation that must consider not only the survival benefits but also the surgical risks and post-operative quality of life. The scope of lymphadenectomy should be individualised and decided based on an accurate preoperative and intraoperative assessment of the extent of disease and the patient’s fitness. Patients that are fit for surgery should have a D2 lymphadenectomy with preservation of the pancreas and spleen. For far- advanced cases and high risk patients, a more limited D1 lymphadenectomy should be carried out. For a better quality of life and low postoperative morbidity, total gastrectomy should be avoided except for cancers diffused on the stomach. Following this approach in our patients, we have acceptable postoperative morbidity and mortality and long survival time. In addition, our patients had significantly improved quality of life. This approach is appropriate and effective in our setting and is recommended for surgeons practicing in similar circumstances. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11078t4.jpg] [hs11078t2.jpg] [hs11078t1.jpg] [hs11078t3.jpg] [hs11078t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}