 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 362-369 A comparison of triage methods for Kenyan women who screen positive for cervical intraepithelial neoplasia by visual inspection of the cervix with acetic acid *Lewis KCL1, Tsu VD1, Dawa A2, Kidula NA3, Chami IN2, Sellors JW1, 4 1 Reproductive Health Program, PATH, Seattle, USA, 2 PATH, Nairobi, Kenya, 3 Reproductive Health Department, Ministry of Health, Nairobi, Kenya, 4 Department of Family Medicine, McMaster University, Canada Code Number: hs11079 Abstract Background: Only about one in seven visual inspection with acetic acid (VIA)-positive women has high-grade disease;
further confirmatory testing could rule out false positives.
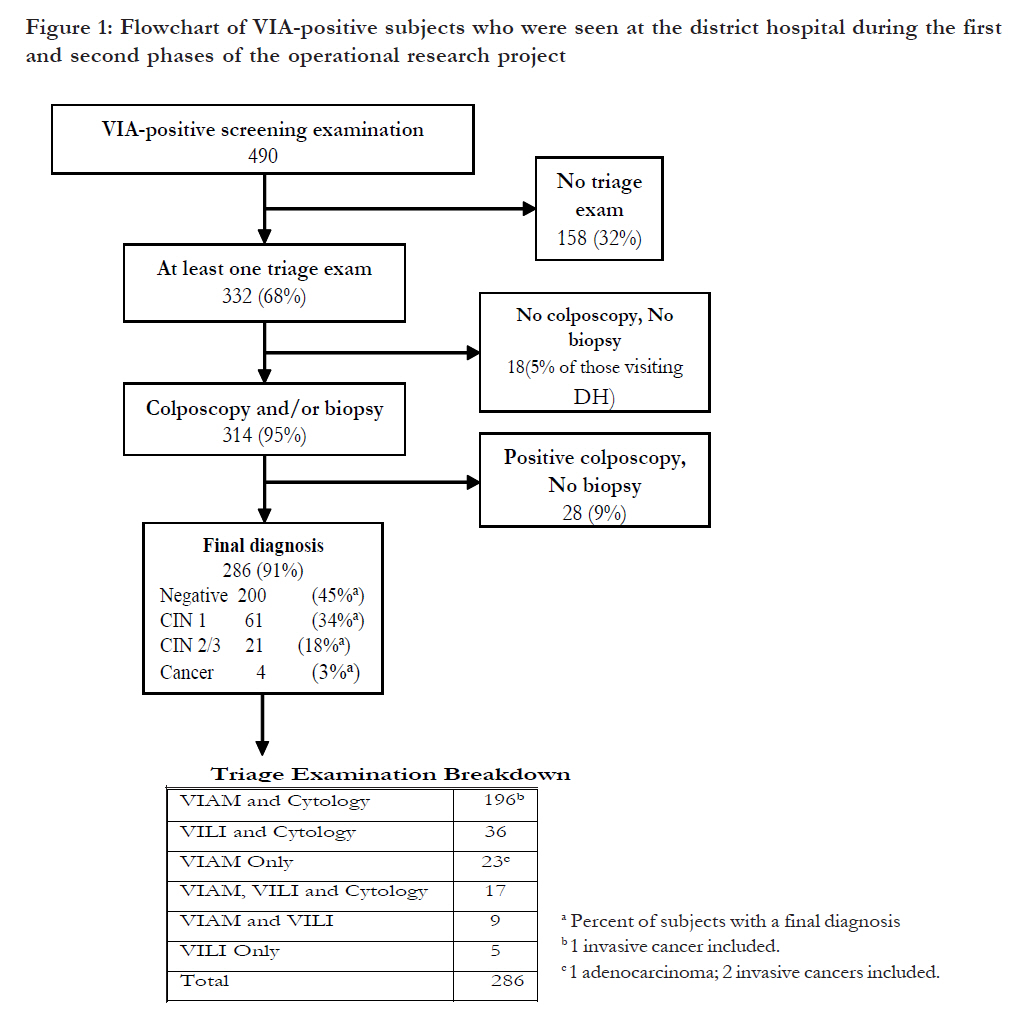
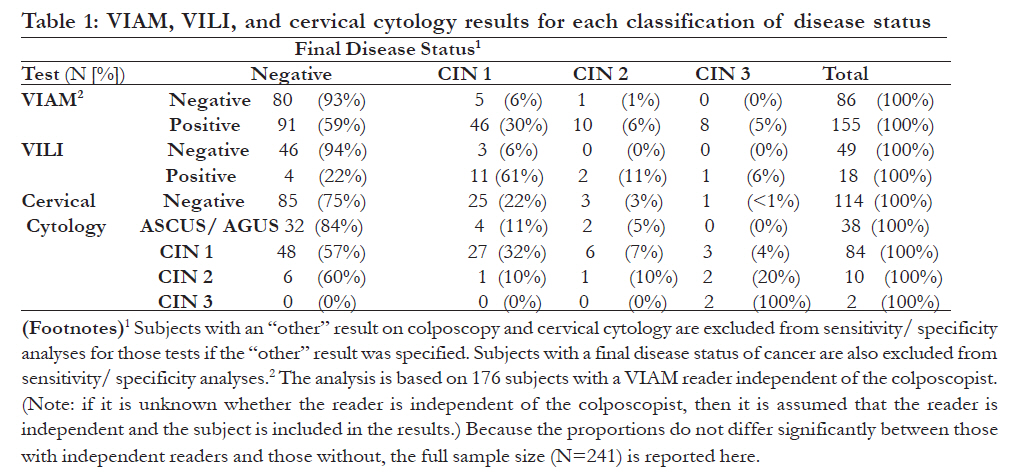
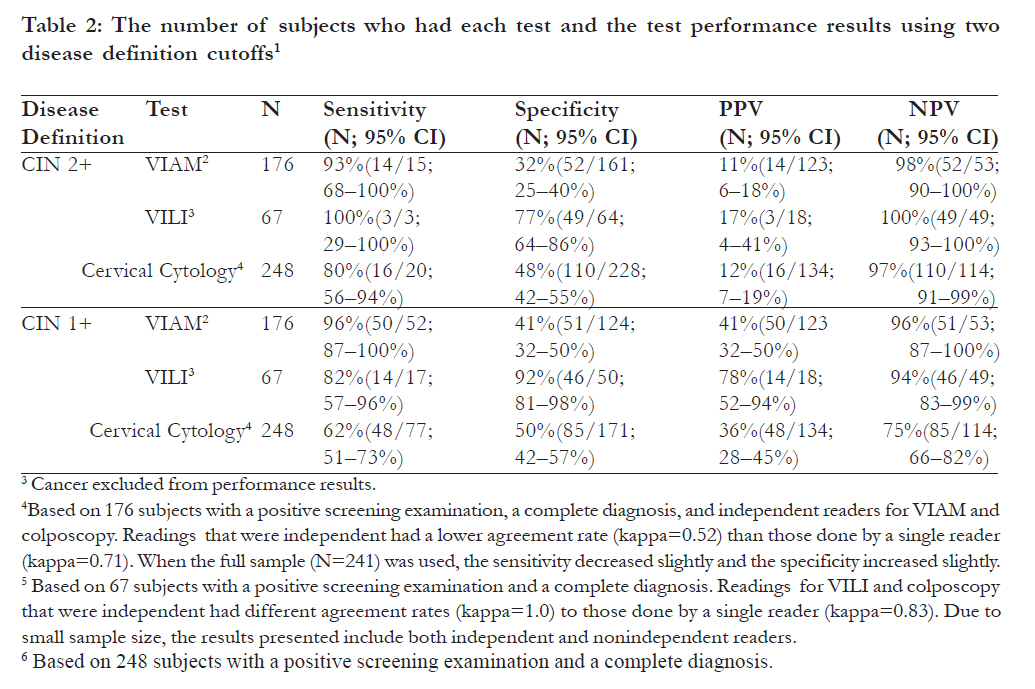
Key Words: cervical cytology, mass screening, neoplasms, precancerous conditions, uterine cervical neoplasms, developing countries. Introduction Cervical cancer is the second leading cause of cancer death among women in developing countries.1 In Kenya, cervical cancer kills more women than any other cancer creating a heavy burden of suffering for women and their families. Age-standardized rates for Eastern Africa are among the highest in the world and are more than three times the rates for Europe and North America.1 Intensive screening programs based on cervical cytology, colposcopy diagnosis, and effective treatment are responsible for the lower cervical cancer incidences in developed countries.2 Cervical cytology-based programs present many challenges that low-resource settings often are unable to meet, such as technical personnel to take and read cervical cytology smears, adequate laboratory supplies, quality control, and means to transport specimens and provide results thereby driving the search for alternatives to cervical cytology for lowresource settings. Visual inspection with acetic acid (VIA), visual inspection with acetic acid and magnification (VIAM), and visual inspection with Lugol’s iodine (VILI) provide immediate results and have been investigated extensively in low-resource settings as alternative screening methods to cervical intraepithelial neoplasia 2 or higher (CIN 2+). In a multicenter study in India and Africa, VILI had a significantly higher sensitivity (92%) than VIA (77%) and comparable specificity (85%). 3 In another study of over 5,800 women, VIAM had a significantly higher sensitivity in detecting CIN 2 or 3 lesions (61%) than VIA (56%) and comparable specificity (82–83%).4 Among women who were referred with abnormal cervical cytology, VIAM correctly identified 60% of those with and 69% of those without high-grade disease5. Among unscreened women, the sensitivity of VIAM for high-grade disease (74%) was not significantly different from cervical cytology (64%), but the specificity was significantly lower (77%) as compared to cervical cytology (96%).6 These visual inspection methods make it feasible to offer both screening and treatment in a single visit. Although many experts consider it to be safe and appropriate to provide treatment simply on the basis of VIA or VILI,2,7,8 only about one in seven VIA-positive women actually has high-grade disease; further confirmatory testing could rule out false positives. Since colposcopic evaluation is seldom possible in low-resource settings, it is important to determine if simple, more widely available methods to confirm the presence of disease are feasible. Although district-specific cancer rates are not available in Kenya, Busia was selected for the project because national referral hospital records suggested a high proportion of cervical cancer patients come from Western Province.9 This operational research project in a rural, low-resource setting investigated the performance of VILI and VIAM as triage tests for VIA screen-positive women in comparison to conventional cervical cytology. Methods Project Overview From 2000 to 2004, a model cervical cancer prevention program suitable for low-resource settings in Africa was evaluated. The Human Subjects Protection Committee at PATH (Seattle, WA, USA) and the Ministry of Education, Science and Technology (Nairobi, Kenya) reviewed and approved this project. The project was carried out in Busia District in the Western Province of Kenya along the border of Uganda, close to Lake Victoria. Women 30 to 39 years old were deemed most at risk of treatable, precancerous disease. Those who were VIA screen-positive at primary health centres were eligible for study participation and were referred to the District Hospital. If pregnancy was known or suspected (based on a history 10 and/or a pregnancy test), women were examined for triage assessment if they wished, but biopsy and cryotherapy were delayed until at least six weeks after pregnancy completion to avoid any implication that the study procedure(s) disturbed the pregnancy. The test procedures were carried out primarily by nurses who recorded all patient information on standard forms. Clinical supervision was provided by clinical officers and district health managers in the Ministry of Health. Visit Protocol This project relied on a two–visit approach whereby all women receiving a positive screening result at the primary health center (first visit) were eligible for inclusion in the triage study and were referred to the district hospital for a triage examination (second visit). All procedures were done by providers who had completed competency-based training. VIAM was the only triage test used during the first two years of the study (November 2000 to October 2002), otherwise known as the first phase. VILI was investigated as a possible triage test during the second phase (November 2002 to March 2004). The procedures during the triage session followed this order: group and individual counseling, signing of informed consent, assessment of pregnancy status, speculum exam, collecting cervical samples for cytology, VIAM, colposcopy, VILI (second phase only) , and, when indicated, directed biopsy. All study procedures, except reading of cytology and histology, were performed by trained study nurses. To reduce expectation bias due to one observer performing more than one type of examination, two providers participated in each subject examination and were blinded to the other’s findings. When only one provider was available, the same provider performed all of the visual tests. To perform VIAM, the cervix was washed with a 5% acetic acid solution as in VIA but a handheld, battery-powered 4x magnification monocular device called the AviScope™ was used to assess the cervix.11 For VILI, the cervix was swabbed with Lugol’s iodine solution and viewed with the naked eye 12,13. Following the application of acetic acid, well-defined, precancerous lesions (CIN 1, 2, or 3) are differentiated by a white color on the cervix; likewise, lesions appear a mustard-yellow color when washed with Lugol’s iodine. For VIAM and VILI, subjects were classified as negative, positive, or suspicious for cancer. An indeterminate category was used only through mid-2002 and then discontinued. Indeterminate cases were classified as positive for the purposes of patient management and data analysis. For cervical cytology, subjects were classified as disease negative if they had normal results and positive if the results were atypical squamous cells of undetermined significance (ASCUS) or higher. The reference standard used for evaluating the performance of triage tests was determined as follows. A subject was considered negative for CIN if her biopsy was negative or if there was no biopsy result and colposcopy was negative. Presence of neoplasia was assessed on the basis of histology. Results were analyzed in two ways: low- and highgrade combined (CIN 1, 2, or 3) or high-grade only (CIN 2 or 3; CIN2+). Since the goal of the triage examinations was to identify precancerous lesions, all women with cervical cancer (n=4) were excluded from analysis. Pathology The majority of the pathology specimens were reviewed by a pathologist in Nairobi, Kenya (Fazana Rana, MD). Pathology samples taken between November 2000 and August 2002 were reviewed by expert French gynecology pathologists (Lucien Frappart, MD; Bernhard Fontaniere, MD) blinded to all data except the age, menstrual and contraceptive history. The expert diagnoses were compared to the diagnoses made by the in-country pathologist to determine the rate of agreement. When available, the expert diagnoses were used in calculating test performance. Data Management and Analysis Clinical data were collected on standard forms, transferred to data forms by project staff, entered into an Access 2000 database14, and analyzed by using Intercooled Stata 8.2.15 The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and 95% confidence intervals were calculated for each triage method (VIAM, VILI, cervical cytology) as compared to the reference standard diagnosis based on colposcopy with histology as necessary. In order to eliminate potential expectation bias, the analysis of the performance of VIAM is based on results from independent readers only. However, we do not have an adequate sample size to assess the accuracy of VILI based on independent readers alone. We tested for potential bias of nonindependent readers (that is, readers performing both the colposcopy and triage examinations) by comparing test performance results between independent and nonindependent examinations, using chi-square scores and p-values. Results Study Population Of the 490 women with positive VIA screening results referred to the district hospital, 332 (67.8%) received a triage examination with VIAM and/or VILI and 284 (85.5%) of these women also received cytology. Among those receiving a VIAM and/or VILI examination, 314 (94.6%) had a cervical biopsy or colposcopy result and 286 (86.1%) had a final diagnosis. The VILI, VIAM, and cytology analyses are based on 67, 245, and 249 women respectively with a final diagnosis [Figure - 1]. Screen-positive subjects who attended a triage visit had similar physical and demographic characteristics with screen-positive subjects who did not attend triage (data not shown, -no significant differences). A cervicovaginal infection was suspected in 32% (107/332) of subjects. Syndromic management criteria identified 93% (100/107) of suspected infections, while 7% (7/107) were identified using cervical cytology. Of the nine subjects presenting for examination during pregnancy, eight of these subjects (89%) elected to have triage exams. [Table - 1] shows the distribution of VIAM, VILI, and cervical cytology compared to the final diagnosis. Test-positive rates were 27% (18/67), 64% (155/241), and 54% (134/248) for VILI, VIAM, and cytology, respectively. For low-grade or higher lesions, a higher proportion of subjects were correctly diagnosed as negative for VIAM (93%; 80/86) and VILI (94%; 46/49) as compared to cervical cytology (75%; 85/114). In addition, a higher proportion of subjects were also correctly diagnosed as positive for VILI (78%; 14/18) and a slightly higher proportion (41%; 64/155) for VIAM as compared to cervical cytology (36%; 48/134). Among the 67 VIA-positive women who received a VILI examination, the 49 women negative for CIN2+ were correctly identified, thus reducing the number of screening false positives by 73% (49/67). VIAM and cytology eliminated significantly fewer false positives, 35% (85/241; p<0.0001) and 44% (110/ 248; p<=0.0001), respectively. Because VIAM was the only triage method tested in the primary phase, during which the majority (86%) of triage visits occurred, and because nonindependent readings and subjects with cancer were excluded from the analysis, the analyses of sensitivity and specificity for VIAM are based on a larger sample size (n=176) than are those for VILI (n=67). Cervical cytology (n=248) was done throughout the study and assessed by independent readers. Although there is some overlap among the 282 participants included in the analysis, not every subject receiving one of the tests also received one or both of the other tests. However, these three groups of subjects have similar ages, squamo– columnar junction visualization, presence of sexually transmitted infections (STI), and pregnancy status (age 35–39: 47–50%; squamo-columnar junction visualized: 96–100%; STI presence: 32–37%; pregnancy: 2–5%). Test Performance Test-positive rates were 33% (28/84) for VILI, 64% for VIAM (178/280), and 53% for cervical cytology (149/282) [Table - 2]. For CIN 2+, the sensitivities are similar among VILI, VIAM, and cervical cytology (p>0.05), but VILI is significantly more specific than VIAM and cervical cytology (p<0.05). For CIN 1+, VIAM is more sensitive than cervical cytology (p<0.05) and VILI is more specific than either VIAM or cervical cytology (p<0.05). The PPV of VILI is higher than VIAM or cervical cytology (p<0.05). The NPV of VIAM and VILI are similar, while the NPV of cervical cytology is lower (p<0.05). Test Independence In 30% (71/235) of subjects receiving a VIAM examination, the same provider performed the colposcopy examinations, while, for VILI, this occurred in 51% (25/49) of cases. When different providers performed the VIAM and colposcopy examinations, there were fewer concordant results than when the same reader did both examinations, but this was non significant (X2=2.18, p=0.14). The effect of independent readers on VILI was also nonsignificant (X2=1.48, p=0.22), but there were moreIn 30% (71/235) of subjects receiving a VIAM concordant results when the same reader performed examination, the same provider performed the the examinations in this small sample of subjects. Quality Control An expert pathologist reviewed 55% (156/282) of all cervical cytology and 48% (78/163) of all histology specimens. After grouping, the cervical cytology results into four categories (negative/ASCUS, CIN 1, CIN 2/3/atypical glandular cells of undetermined significance or AGUS, cancer), there was only slight agreement between the incountry and expert readers (kappa=0.08, p=0.02). Similarly, after grouping the histology categories (negative, CIN 1, CIN 2/3, cancer), there was also only slight agreement (kappa=0.11, p=0.03). Discussion In this study, VILI appears the most promising triage test. The specificity of VILI was higher than either cervical cytology or VIAM, and the false positive rate was lower, without loss of sensitivity. Our results are similar to those in a multi-center study of over 55,000 subjects where the sensitivity and specificity of VILI were found to be 92% (95% CI: 90–93) and 85% (95% CI: 85–86), respectively.3 VILI was used as a primary screening examination in the latter study, but due to the higher prevalence of disease in a screen-positive population, one would expect test performance to be better in a screen-positive group of subjects. Other than the difference in settings, it is not clear then why our results are similar to those of Sankaranarayanan3, despite the use of VILI in screened subjects rather than in unscreened subjects. The small sample size contributed to wide confidence intervals and, with a larger sample, our results may have shown better test performance in this screenpositive population. Use of VILI as a triage test would be expected to result in fewer subjects being treated unnecessarily compared to using VIAM or cervical cytology for triage. The reduction in treatment of false positives decreases discomfort and inconvenience for subjects, provider workload, and treatment cost. As other studies have shown, VIAM does not offer any advantage over other screening or triage techniques4,5,7,16-20. In addition, the AviScope™ is susceptible to equipment failure if dropped on a hard surface or immersed in water. Given recent findings and advances in technology, there is optimism that the performance and affordability of a handheld scope could be improved.11 Although further studies should be performed with a larger sample size, in a two-visit approach, VILI seems to be superior to VIAM as a triage test without the need for additional equipment or the repair and maintenance of such equipment. This project found that nurses, rather than gynecologists or general physicians, can be trained to perform VILI and VIAM in one to two weeks with didactic and practical sessions13 and, because the supplies are low-cost and readily available, such a program can be integrated into routine service delivery allowing for opportunistic screening. In order to maintain provider competence, supervisory visits can be used to perform refresher training onsite by direct observation and using pictures of VIAand VILI-stained cervices. The direct observation and immediate feedback are helpful in assessing provider capabilities and improving skills21. Only two providers were active throughout the study so we are unable to comment on the generalizability of the results to other providers. Although cervical cytology is the screening method in developed countries, it is difficult to implement effectively in low-resource settings due to the prohibitive travel time and costs associated with multiple clinic visits. Due to the distance between clinic and laboratory sites, returning cervical cytology results to subjects is often delayed and, consequently, loss to follow-up occurs. Other difficulties include a shortage of trained pathologists and inadequate implementation of quality control mechanisms22,23. It may also be argued that the sensitivity of any screening test used once or twice in a woman’s lifetime should be as high as possible. While the most cost-effective strategy is based on a single visit24, in some settings it is not feasible to provide treatment at the primary care level25 or to offer a two-visit screening program based on VIA for primary screening and VILI for triage of VIA-positive subjects. Quite often, a woman may need approval from her husband for each step of the management process: screening, triage, diagnosis, and treatment.25 For these reasons, it may be more feasible and acceptable to offer a two-visit screening program integrated into routine service delivery using VIA for primary screening and VILI for triage of VIA-positive subjects. If staffing levels for other services are adequate, additional providers are not required and opportunistic screening can be provided when women seek clinic services for other reasons. Lugol’s iodine and extra cotton swabs, readily available in low-resource settings at a small cost, are the only supplies needed. Our study findings are limited in that they apply to the 30 to 39 year eligible age group. Ideally, all three triage tests should have been performed on each woman by independent assessors to allow comparison of their performance to a reference standard. Because this was operational research carried out in a low-resource setting, this proved impossible. Although there were no differences in demographic characteristics among the three groups of subjects receiving each triage test, some of the differences in test performance observed may be due to small sample sizes and biases introduced by nonrandom allocation. Finally, there was poor agreement between the local and expert histology readers. Expert results were used as the histology gold standard when available, but were not completed during Phase 2 or for all Phase 1 readings. As discordance between the available local and expert reviewer readings both downgraded and upgraded disease, it is unknown how the use of expert histology results for all participants would have affected the final results. Due to the limited numbers of subjects, the results of VILI tests performed by the same provider who did the colposcopy and those performed by a different provider were combined to assess VILI test performance; this may have biased our conclusions in favor of VILI. Before the results from this study can be generalized, they should be replicated with a widened age range (for example, 30 to 49 years), all tests performed on each woman by different examiners, and adequate sample sizes used. Conclusion Based on these findings among small numbers of women, VILI might be useful as a triage test after VIA to correctly identify women who truly have cervical precancer and would benefit from treatment, while substantially reducing the number of falsepositive cases. More research is needed to confirm the reliability and accuracy of VILI when used for triage. Acknowledgements This project was supported by a grant from The Bill & Melinda Gates Foundation through the Alliance for Cervical Cancer Prevention. PATH staff and partners who contributed their expertise to this project who provided valuable input to the early design and management of the project. We would like to thank all of our collaborators in Western Kenya, including our partners and their staff (Kenya Cancer Association; Maendeleo ya Wanawake Organization; the national, provincial, and district levels of the Kenyan Ministry of Health; and the Ministry of Culture, Sports, Education, and Welfare). Lastly, in France, Drs. Fontaniere and Frappart who provided pathology quality control. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11079t2.jpg] [hs11079f1.jpg] [hs11079t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}