 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
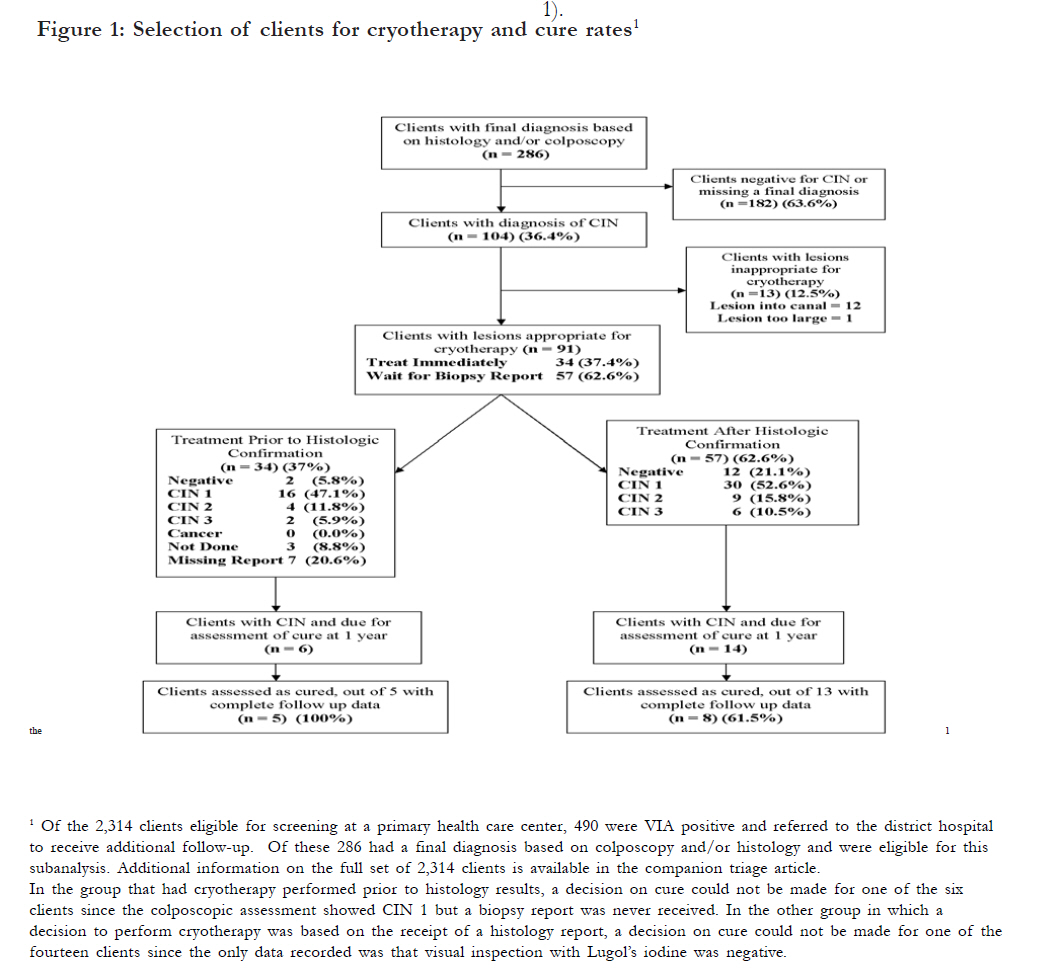
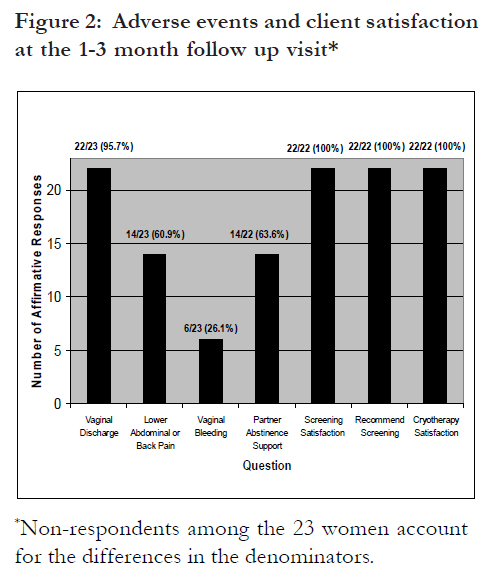
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 370-376 Report on a cryotherapy service for women with cervical intraepithelial neoplasia in a district hospital in western Kenya *Lewis KDC1, Sellors JW1,3, Dawa A2, Tsu VD1, Kidula NA4 1 Reproductive Health Program, PATH, Seattle, USA, 2 PATH, Nairobi, Kenya, 3 Department of Family Medicine, McMaster University, Hamilton, Canada, 4 Reproductive Health Department, Ministry of Health, Nairobi, Kenya Code Number: hs11080 Abstract Background: In low-resource settings, cryotherapy can be cost-effective, affordable, and a first-line treatment for cervical intraepithelial neplasia (CIN) of any grade. Key Words: cryotherapy; developing countries; neoplasms; precancerous conditions; uterine cervical neoplasms Introduction In contrast to the situation in developed countries, cervical cancer is currently the leading cause of death and years of life lost due to women’s cancer in developing countries1. Developed countries possess the political will and resources to mount effective screening programs based on cervical cytology2. An alternative screening method, visual inspection with acetic acid (VIA), has been used successfully to screen women who are at least 30 years of age in several developing countries3. Cryotherapy and loop electrical excision procedure (LEEP) ablate or excise the transformation zone, respectively, and are performed commonly as outpatient procedures4. In low-resource settings, cryotherapy, using either a ‘single visit’ or ‘see and treat’ approach, has been shown to be cost-effective, affordable, and an ideal first-line treatment for CIN of any grade when the cervical lesion size and location allows the cryoprobe tip to make adequate contact5, 6, 7, 8, 9. Cryotherapy can be performed at the primary care level by mid-level providers, such as nurses or midwives, who can be trained to perform cryotherapy with a minimum of supplies and equipment7, 10. A systematic review of cryotherapy performed in 2004 showed that cryotherapy is approximately 90% effective for all grades of CIN when assessed 1 year after cryotherapy, based mainly on studies from developed countries5. The side effects reported by women in the studies analyzed were lower abdominal cramping during and immediately after cryotherapy and a persistent watery vaginal discharge for approximately 1 month5, 6. To our knowledge there have been few studies in lowresource settings on the acceptability to women of the adverse-effects of cryotherapy, and their success in avoiding vaginal intercourse during the 1 month healing period11, 12. As part of a larger study on the accuracy of screening and triage tests, this analysis was conducted in order to evaluate the acceptability, safety and effectiveness of a new cryotherapy service for women referred to a district hospital in Western Kenya. Methods This project on the acceptability, safety and effectiveness of a newly established cryotherapy service in a low-resource setting was approved by the Human Subjects Protection Committee at PATH (Seattle, WA), and by the Ministry of Education, Science and Technology (Nairobi, Kenya). The VIA was conducted at five primary health center clinics, one dispensary clinic, and one district hospital in the district of Busia in Western Province, Kenya, from November 2000 until March 2004. Women who were VIA-positive or suspected of having cervical cancer based on an initial evaluation at a primary health facility were referred to and evaluated at the district hospital by Visual Inspection with Added Magnification (VIAM) and/or Visual Inspection with Lugol’s Iodine (VILI), as well as by colposcopy and directed cervical biopsy, as required. If necessary, cryotherapy was provided as treatment for CIN lesions. At the district hospital, all procedures were performed by one of four trained nurses or a visiting gynecologist. Pregnant women were excluded and instructed to return at six weeks postpartum. A specimen for conventional cytology was then collected on all women using an Ayre’s wooden spatula after a vaginal speculum had been inserted using water as a lubricant. These slides were examined by a cytologist after they were fixed and stained. Results were graded using the Bethesda System classification. The VIAM was performed using 35% acetic acid to wash the cervix and waiting 1 minute before examining the cervix with a lowpower, handheld magnification device, respectively. 3 The VILI was performed by washing the cervix with Lugol’s iodine solution and immediately examining the cervix with the naked eye.3 A positive test result for VIAM was the presence of a welldefined area of acetowhitening on the cervix and a positive VILI result was a well-defined Lugolnegative area.3 If any visual test was positive, colposcopy was performed and a cervical biopsy obtained from any abnormal area. Cervical biopsies (histology) were performed by expert pathologists who were blind to the clinical findings and, whenever possible, positive readings were assessed by a second pathologist and disagreements resolved by discussion. As cervical lesions are slow growing and treatment is not urgent, other factors like convenience and patient preference determined whether or not cryotherapy was performed immediately following colposcopic diagnosis. In some cases, cryotherapy was done immediately after colposcopy and biopsy at the district hospital (a priori histological confirmation) while in others the patient was given an appointment for cryotherapy when her histology results would be available (a posteriori histological confirmation). Patients who defaulted from treatment initially were located later and encouraged to attend for re-assessment and cryotherapy if warranted. The decision to treat immediately, before knowing the histology result, was based on the certainty of the colposcopist that a CIN lesion was present, the appropriateness of the lesion for cryotherapy, and the preference of the patient. If cervicitis was suspected based on observation of purulent cervical discharge and inflammation, norfloxacin (400 mg cap, two stat) and doxycycline (100 mg tab, BID for 5 days) were prescribed and the woman was instructed to return for treatment after about two weeks. Assessment of cure following cryotherapy was completed during a 1year post-cryotherapy follow-up visit. Cryotherapy using nitrous oxide and a cryotherapy unit (model LL100, Wallach Surgical Devices; Orange, CT) was conducted for two 3minute periods, separated by a 5-minute period for thawing, as previously described4. To prevent infection, all women were given norfloxacin and doxycycline in the same dosages as for cervicitis, immediately after cryotherapy. The use of cryotherapy was considered inappropriate if a lesion could not be adequately covered by the tip of the cryoprobe, or if the lesion extended into the endocervical canal. Any woman with a lesion that was inappropriate for cryotherapy and those with confirmed or suspected cervical cancer were referred to a provincial hospital for further management. Women who had still not returned for cryotherapy treatment by the end of the study period were contacted and encouraged to attend. After cryotherapy, women were advised to abstain from vaginal intercourse for at least 1 month and invited to return for two follow up visits; one visit at 1 to 3 months for supportive care, and another at 1 year for test of cure based on conventional cytology and colposcopy, with directed biopsy as necessary. Women found to have persistent disease at the 1-year follow-up visit were managed using repeat cryotherapy, when appropriate, or referral to the provincial hospital. The adverse events and acceptability of cryotherapy were assessed during the 1 to 3 month follow-up visit by asking a series of questions assessing vaginal discharge, bleeding, pain, satisfaction with screening and treatment, and partner support of abstinence from vaginal intercourse for 1 month after treatment. At the 1year visit the client was asked whether she would recommend cryotherapy to others. Sample size was limited by the rate of referral to the district hospital, the numbers of women referred who were suitable for cryotherapy over the first 2.5 years, and the 1-year period of follow-up required for women after cryotherapy. For this reason a sample size requirement was not calculated a priori and is based on a convenience sample, given the time and resources available. Data on all women in the study were collected on precoded data forms, entered into a computer, and analyzed using Intercooled Stata 8.2. Statistical significance was not tested due to the small sample sizes. Results Of the 2,290 women attending screening at a primary health clinic, 489 (21%) had a positive VIA test and were referred to the district hospital for confirmatory testing. Of these, 337 (69%) presented for reexamination at the district hospital and 286 (59%) were examined at the district hospital using a triage examination (VIAM and/or VILI) and had a final diagnosis based on colposcopy with or without cervical histology. Of the 286 women with a final diagnosis, 104 (36.4%) with a mean age of 34.7 (SD, 3.6) years had cervical neoplasia diagnosed [Figure - 1]. Of the 104 women with cervical neoplasia, 13 (12.5%) had lesions that were deemed inappropriate for cryotherapy and were referred to a provincial hospital for follow-up care. Approximately 88% (91/104) had lesions that were compatible with CIN on colposcopy and appropriate for cryotherapy and, therefore, were eligible to receive cryotherapy [Figure - 2]. Cervicitis (n=16), trichomoniasis (n=3), and pelvic inflammatory disease (n=1) were diagnosed clinically and treated in 20 women (22.0%), 19 (95.0%) of whom had cryotherapy delayed until antibiotic treatment was completed. All women with pelvic inflammatory diseases and trichomoniasis were treated after receipt of biopsy results (a posteriori), while 62.5% (10/16) of women with cervicitis were treated a posteriori and the other 37.5% (6/10) were treated prior to receipt of biopsy results (a priori). Of the 91 women eligible to receive cryotherapy, the decision to administer cryotherapy was based on the colposcopic impression in 34 (37.4%) and based on the results of a colposcopically-directed biopsy in 57 (62.6%). Of the 34 women who had cryotherapy based on colposcopic impression, a biopsy result was reported for 24 and the rest either had no biopsy done or the results were not reported [Figure - 1]. Among the 81 women with histology results available, 14 (17.3%) had a negative result, and CIN 1, 2 and 3 were confirmed in 46 (56.8%), 13 (16.0%), and 8 (9.9%), respectively. Of the 14 women with negative biopsy results, 9 (64.3%) were treated on the basis of an initially positive histology reading (7 CIN 2, 2 CIN 1) that were later assessed as negative for cervical neoplasia on pathology review, and 5 (35.7%) were treated on the basis of the colposcopic diagnosis of CIN. While 21.1% (12/57) of women treated after receipt of biopsy results had a negative final diagnosis based on the triage visit to the district hospital, only 5.8% (2/34) treated prior to receipt of biopsy results had a negative final diagnosis. At the time of study closure, 83.3% (20/ 24) of the 35.8% (24/67) of women eligible to participate in a 1-year follow-up visit were examined. The 20 women eligible and available to participate in the 1-year follow-up visit were examined by colposcopy, directed biopsy as necessary, and cytology. One client each in the a priori and a posteriori groups did not have adequate information for assessing a final diagnosis. Therefore the calculation of cure rates is based on the 18 women with complete data at the time of follow up. Overall, 13 of the 18 clients (72.2%) (95% CI, 51.5% - 92.9%) were assessed as cured, including 75.0% (6/8) with CIN 1, 80.0% (4/5) with CIN 2, and 60.0% (3/5) with CIN 3. The cure rate among clients treated a priori (5/5, 100.0%) was similar to clients treated a posteriori (8/13, 61.5%) For the women with provider information available, the cure rates were similar for those treated by nurses (9/11) and those treated by the gynecologists (2/4). By the end of the study period, 34 women were eligible to attend the 1 to 3 month follow-up visit, and 23 (67.6%) attended and answered questions regarding adverse events and satisfaction with treatment [Figure - 2]. The most commonly reported complications were moderate watery or foul-smelling vaginal discharge in 22 of 23 respondents (95.7%), lower abdominal or back pain that may not have been present prior to cryotherapy in 14 of 23 (60.9%), and mild or moderate vaginal bleeding in 6 of 23 (26.1%). All subjects responding to the question reported that they were satisfied with the treatment (22/22; 100%). Partner support during the 1 month postcryotherapy abstinence period was reported by 14/ 17 (82.4%) respondents. Satisfaction with screening and treatment was unanimous among the 22 respondents to this question, and all said that they would recommend screening to their friends. Discussion To our knowledge this is the first report of a newlyestablished cryotherapy service in a low-resource setting in Kenya. Women found cryotherapy acceptable and nearly all would recommend the service to their family and friends, in agreement with other reports from low-resource settings11, 12. The majority of husbands and partners were supportive of the empirically-based, recommended 1 month period of abstinence from vaginal intercourse in order to decrease the chance of injury or infection of the cervix while it is healing. The post-cryotherapy complications reported by clients in this study are consistent with the abundance of evidence on cryotherapy showing that adverse events are usually minor and of brief duration5. In addition, nurses were found capable of performing cryotherapy and may be a suitable alternative to gynecologists who are not routinely available in such a remote setting. Among the women with a visual impression of CIN, 87.5% were assessed as suitable for cryotherapy without any contraindication such as endocervical canal involvement, a lesion larger than the cryoprobe tip or a lesion suspicious for cancer. Of those with a histologic diagnosis of CIN and able to be followed up 1 year later, an average of 72.2% were cured across clients treated a priori and a posteriori with a lower 95% confidence limit of 51.5%. Although the data presented here were generated in a very poorly-resourced setting with a sample of convenience, the small numbers suggest an overall cure rate that is similar to recently reported cure rates of 81.4% (CIN 1), 71.4% (CIN 2), and 68.0% (CIN 3) achieved by nurses in a Southern India research setting, and cure rates of 88% and 97% overall by physicians in Peruvian and Ghanaian settings respectively. 13, 14, 15 Providers were permitted to treat clients using cryotherapy based on a colposcopic impression of an appropriately-sized and located CIN lesion, provided they first had obtained a biopsy. This was felt to be an important option for patients and providers since it has been shown that convincing women of the importance to return for follow-up is difficult, and treatment offered immediately after screening yields optimal programmatic effectiveness7,9 . Without symptoms of disease, women with precancerous cervical lesions are unlikely to seek followup care because of fear, costs of transport and child care, and need for permission16. We believe that providers chose to provide cryotherapy in the absence of biopsy results for over one third of clients because of these potential barriers to returning to the district hospital for treatment. Interestingly, fewer women had negative final diagnoses in the group receiving cryotherapy a priori as compared to women receiving cryotherapy a posteriori, perhaps because providers were more willing to recommend treatment without biopsy confirmation when the lesion was more obvious. Since this study was not designed to assess the effect of timing of cryotherapy on treatment outcomes it is not possible to make any conclusions on whether the a priori or the a posteriori histologic confirmation approach is better. Other barriers to administration of cryotherapy for those who need it include equipment malfunction due to blockage and poor design (e.g., the Wallach cryotherapy equipment had a design flaw that caused temperatures above -20°C that led to a product recall), and breakage without the availability of adequate repair and maintenance training. 17 In Ghana, Peru and Kenya, we and others have reported problems with interruption of cryotherapy because of ice formation in the cryotherapy apparatus tubing which blocks the passage of refrigerant gas that cools the tip of the cryoprobe. 18 Further research has been conducted to understand possible solutions for this problem, such as an inexpensive gas conditioner device designed by PATH which eliminates ice crystal blockage by drying the gas as it passes between the gas tank and cryotherapy probe (Seattle, WA). 18 While the successful performance of cryotherapy provides some challenges, in contrast to LEEP, cryotherapy equipment is simpler and less costly, does not require local anesthesia or electricity, and can be performed safely and effectively by mid-level providers such as nurses and midwives. 7, 9, 10, 19 One limitation of this research is that the number of women able to be followed up for adverse events, acceptability, and test of cure was limited due to the short duration of the project, restricting the ability to test for statistical significance between groups. However, the methodology employed was as rigorous as possible given the project setting in a routine health care delivery system. Study strengths include that, since this study was performed at a very low level of the health care system in rural Kenya with few inputs other than provision of the equipment and training of local providers in how to perform the procedures, it is possible to generalize the findings to other lowresource settings in developing countries. In a South African randomized controlled trial of screening by VIA versus testing for oncogenic types of human papillomavirus, followed by cryotherapy of women who were positive, cryotherapy was shown to reduce the prevalence of high-grade CIN (CIN 2, 3) found at colposcopy performed 6 and 12 months later by 42% and 76%, respectively, compared to controls20. These findings strongly support the results from similar studies13, 14. Cryotherapy can be used as a firstline treatment by mid-level providers in low-resource settings and diagnostic colposcopy can be reserved for referral situations. Conclusion This research regarding the acceptability, safety and effectiveness of a newly established cryotherapy service in a low-resource setting indicates that cryotherapy is appropriate and effective for most women with abnormalities on visual screening. Additional research is needed to investigate factors influencing the cure-rate of cryotherapy in lowresource settings. Acknowledgements This project was supported by a grant from The Bill & Melinda Gates Foundation through the Alliance for Cervical Cancer Prevention. We would like to thank PATH staff and partners, including Dr. Ketra Muhombe, contributed their expertise to this project and provided valuable input to the early design and management of the project. We would like to thank all of our collaborators in Western Kenya, including our partners and their staff (Kenya Cancer Association; Maendeleo ya Wanawake Organization; the national, provincial, and district levels of the Kenyan Ministry of Health; and the Ministry of Culture, Sports, Education, and Welfare). Lastly, in Lyon, France, Drs. Fontaniere and Frappart provided pathology quality control. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11080f1.jpg] [hs11080f2.jpg] |
| |||||||||

{kind=link}
{kind=link}