 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
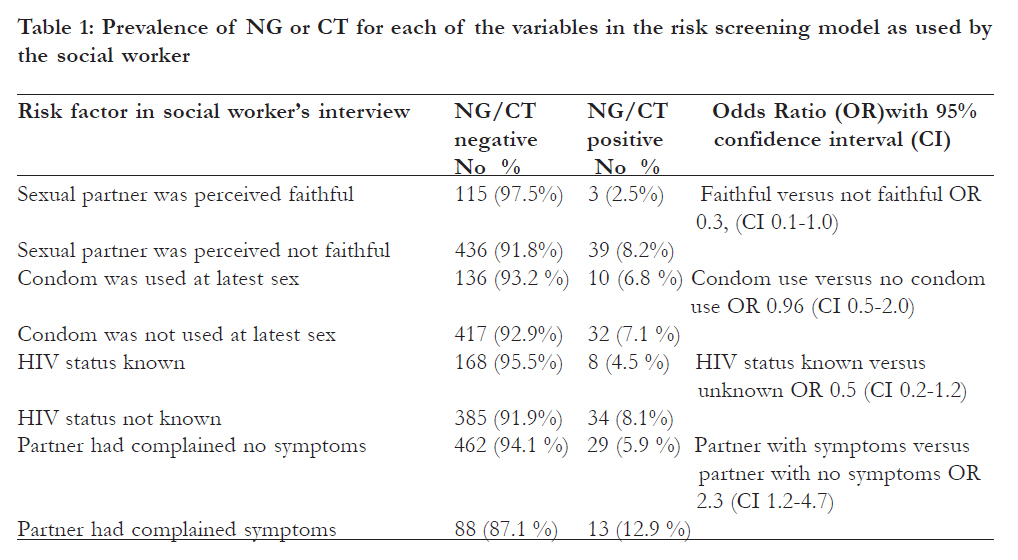
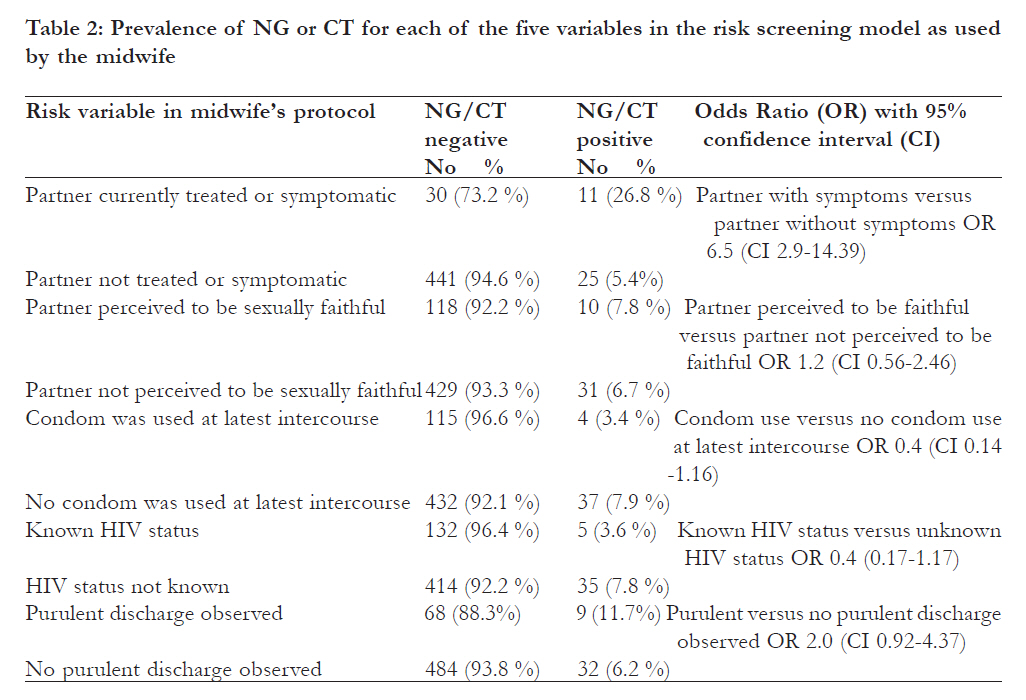
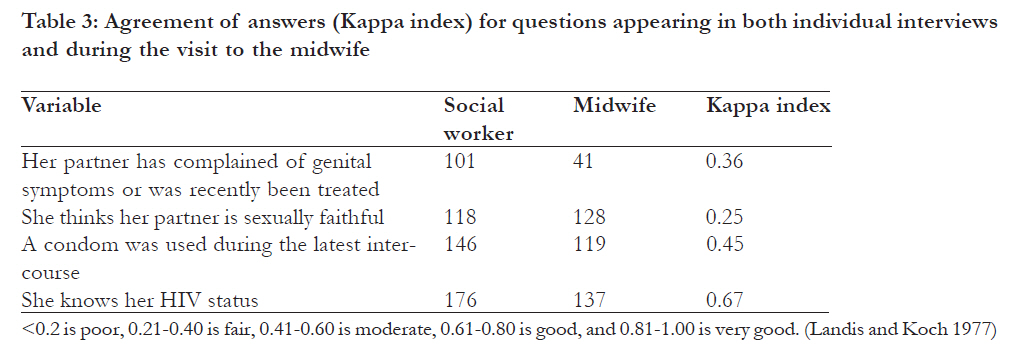
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 383 - 389 Self-reported sexual behaviour among adolescent girls in Uganda: reliability of data debated *Råssjö EB1, Mirembe F2, Elisabeth Darj3 1 Department of Obstetrics and Gynaecology, Centre for Clinical Research, Falun Hospital, Sweden, 2 Department of Obstetrics and Gynaecology, Mulago Hospital, Kampala, Uganda, 3 Department of Women’s and Children’s Health, International Maternal and Child Health, Akademiska Hospital, University of Uppsala, Sweden Code Number: hs11082 Abstract Objective: To compare self-reported information about sexual behaviour in a research interview to information retrieved during a clinical consultation. Key words: Adolescents, Risk factors, reliability, STI, Uganda Introduction The accuracy of self-reported behaviours and reliability of data obtained in studies of sexually transmitted infections (STI) and related risk factors is crucial for the interpretation of results. Reliability of a data sampling method refers to the dependability or consistency of measurement1. It is never possible to know if the reported behaviour represents the truth or if the responses are adjusted to fit the investigator’s perceived expectations. According to Foertenberry it is necessary to recognise and accept an irresolvable gap between an unknowable truth and a knowable datum 2. However, strenuous efforts toward accuracy and precision are an explicit responsibility of investigators. In a previous study of STIs and risk factors assessment among patients in a youth health clinic in Kampala, Uganda 3, some factors appeared associated with lower risk for infection. These factors were: sexually faithful partner, condom use at latest intercourse and known negative HIV status. In a theoretical model, these low-risk factors were combined and used in a flowchart for management of vaginal discharge in adolescents. A woman should be treated for NG and CT only if she had none of these low-risk factors or if her latest/current partner had complained of any genital symptom, or there were signs of pus on vaginal examination. Vaginal infections such as candidiasis, bacterial vaginosis and trichomonas should be treated according to symptoms and clinical signs. Theoretically, this new flow-chart had a better sensitivity for capturing true cases of Neisseria gonorrhoea (NG) and Chlamydia trichomatis (CT) without lowering specificity, compared to a flow-chart for syndromic management of AVD, developed by WHO 4. The objective of the current study was primarily to evaluate if this new flow-chart could be clinically used by midwives. Methods This study was approved by the Ugandan National Council for Science and Technology. This investigation was designed as a quantitative descriptive study. Data collection started in September 2006 and continued for 12 months. Young women visiting a youth clinic in Kampala and a youth clinic 18 km outside the city participated in this study evaluating the prevalence of NG and CT and possible risk factors associated with these infections. The urban study site was located in a densely populated slum area, while the rural study site was located near a small trading centre on the highway towards the south-western parts of Uganda. In both study sites clients were offered counselling, family planning, treatment for STIs and HIV counselling and testing. All women who met the inclusion criteria which comprised of age below 20 years; sexually experienced (had had vaginal sexual intercourse at least once); and, her reason for visiting the clinic was genital symptoms and/or a fear of being infected with an STI, were invited to participate. After receiving written and oral information, consenting women were interviewed by one of three social workers, one male and two females. Two of the social workers, the male and one of the females, were previously working in the study sites and known by some of the participants. They were all experienced in conducting research interviews and fluent in both English and Luganda, the most frequently spoken local language. A structured, pre-tested questionnaire was used. Questions asked in English or Luganda covered genital symptoms, sexual experience and behaviour. The “low-risk” questions were embedded in the questionnaire: do you think your partner is sexually faithful, was a condom used at latest intercourse, and have you ever been HIV-tested. They were also asked if their current or latest partner had complained or received treatment for any genital symptom. After the interview, a step-by-step protocol was followed by a midwife, who asked if the woman thought she could trust her partner, if condoms had been used at latest intercourse, if she knew her HIV-status and if the current or latest partner had complained of any genital symptom. The midwife also did a vaginal sampling for detection of NG and CT as well as making the decision on whether to treat or not. A woman was defined to be at low risk if there were no signs of pus on vaginal examination and if she answered yes to any of the questions: “Do you think your partner is sexually faithful?” “Was a condom used at latest intercourse?” “Have you ever been HIV tested?” and no to the question “Has your current or latest partner complained or received treatment for any genital symptom?”. If she answered no to all the “low risk” questions or if her partner had genital symptoms or had been treated or if pus was seen on vaginal examination, the woman was defined to have high risk of being NG/ CT positive and should receive treatment. The samples were sent on a daily basis for PCR analysis at the Ugandan National STD laboratory, Mulago Hospital. SPSS 15.0 for Windows was used for statistical analyses. Prevalence of NG and CT and associated risk factors were calculated. A bivariate analysis was conducted involving 2x2 tables, with a positive laboratory result for NG and/or CT as the outcome variable. A chi-square test was used to test significance of the results. Odds ratios and their 95% confidence intervals were estimated. Results A total number of 697 young women were available for the study. One hundred and two women abstained from participation or were excluded from the study for different reasons. The reasons for abstaining were being in their menstrual period, fear that the sampling procedure would be painful, too shy to be examined or they just did not want to participate. Three women had extensive genital sores and the midwife did not want to sample, as it could be too painful. Data from seven women who were 20 years old were excluded from the analysis. Therefore data from 595 women was analysed. Response rate varied for different questions from 507 to 595. The lowest response rate was found for the question about partner symptoms. The NG was diagnosed by PCR in 4.5% and CT in 3.7% of the participants, and 7.1% were found to have either NG or CT. There was no statistical difference in infection prevalence between the two clinics. [Table - 1] shows the prevalence of NG/CT for the risk factors explored in the social worker’s interviews. A lower risk of infection with NG/CT was noted among girls who said they trusted their partner. Only three women (2.5 %) were infected compared to 39 (8.2%) of those who did not trust their partner. Among the 146 women who claimed that they had used a condom at latest intercourse the prevalence of NG or CT was 6,8 %, similar to the prevalence among the 449 women who said that they had not used a condom (7.1 %). The interviewer also asked whether the woman always used condoms for protection. Among the 82 women who claimed they always use a condom, there were three (3.7%) NG/CT positive cases compared to 39 or 7.8% among these who were not constantly using condoms. The difference was not statistically significant. Almost one-third, had been tested for HIV (29.1%). Among the HIV-tested, NG/CT infection prevalence was 4.5 % (eight individuals) compared to 8.1% (34 women) among those not tested. Again, the difference was not statistically significant. Among the 101 women who knew that their artner had STI symptoms 12.9 % were infected by NG or CT compared to 5.9 % among those who did not know of any such symptom (OR 2.3, 95% CI: 1.17-4.70). Among those with any of our presumed low-risk factors: faithful partner, condom use at latest intercourse, or HIV tested, 5.7% (17 women) were positive for NG or CT, compared to 8.7% (25 women) among those who did not report low-risk factors. However, the difference was not statistically significant (OR 0.6, 95% CI 0.3-1.2). In the midwives’ interview it was revealed that among the 128 women who perceived their partner to be sexually faithful, ten (7.8 %) were infected by NG or CT with a similar infection rate (6.7 %) among the 460 who believed their partner had been unfaithful. Among the 115 women who told the midwife that they had used a condom at latest sexual intercourse 4 (3.4 %) were infected compared to 37 (7.9 %) of those who had not used a condom. Five of the 137 (3.6 %) women who said they had been HIV tested compared to 35 of the 449 (7.8 %) who had not been tested, were infected by NG or CT. Likewise, among the 41 women who said their partner had genital symptoms 26.8 % were infected with NG or CT compared to only 5.4 % of the 466 women who did not know about any such symptoms (OR 6.5, CI 2.9-14.39). Whereas the midwife noticed the presence of purulent vaginal discharge the rate of infection with NG or CT was 11.7 % compared to 6.2 % among patients without this sign (OR 2.0, CI 0.92-4.37). The prevalence of NG or CT for each of these five variables is presented in [Table - 2]. With the application of the suggested model for risk assessment, 184 women (32.2%) were classed as low risk and 396 (67.8%) were considered to be at risk. The prevalence of NG and/or CT was 5.4% in the low-risk group and 7.8% in the high-risk group. The difference in cervical infection rate between the assessed low- and high-risk groups was not statistically significant. The correlation between the responses in the research interviews and the risk having NG and/or CT infection (data not shown) and the correlation between anamnesis factors reported to the midwife and the risk of having NG or CT infection all went in the same direction, namely that the presence of the assumed low risk factors tended to indicate a lower risk to have an STI. However, it was observed that a substantial number of women had given incongruent answers in the two data collection situations. Cohen’s Kappa index (k) is a measure of agreement where 1.0 corresponds to perfect agreement and zero means no agreement better than chance5. The correlation between the responses in the The questions appearing in both the interviews research interviews and the risk having NG and/or and midwives protocol are presented in [Table - 3], CT infection (data not shown) and the correlation which shows that agreement was fair for questions between anamnesis factors reported to the midwife about partner symptoms and partners’ faithfulness, and the risk of having NG or CT infection all went moderate for condom use at latest sexual intercourse in the same direction, namely that the presence of and good only for knowledge of HIV status. Discussion The original aim of this study was to evaluate if the new theoretical Adolescent AVD Management Flowchart, developed in Kampala 3 performed better than the WHO algorithm for management of AVD. However, neither the risk-factor screening obtained by one social worker’s interview nor the assessment by a midwife could not discriminate well between women with and without cervical infection. Further, there were substantial discrepancies between information revealed in the individual interviews and during the medical consultation. The reason for using two data sampling methods was to resemble a clinical situation as much as possible although this was a study. The more extensive interview performed by the social workers was aimed at getting a broader picture of the participants than just the clinical and “low-risk” information obtained by the midwife according to her protocol. It was not possible to determine from these data, which set of information was more truthful, and therefore reliable. There were no trends for the women to give socially more acceptable responses when the question was asked a second time. Recall bias should not have been a problem because it was usually less than one hour between the research interview and the clinical consultation. Other possible explanations are that the women were intentionally misleading the investigators or that either the social worker or the midwife failed to fill in the protocol in accordance to the responses given. It can not be ruled out that midwives sometimes forgot to ask the questions and filled in the protocol in retrospect, guessing what the woman would have answered. This would imply that health workers don’t feel that the questions about partner’s symptoms, condom use, fidelity and HIV testing are a natural part of the consultation. In a review of the existing empirical literature, cognitive and situational factors that may affect the validity of adolescents’ self-reported sexual behaviour were described. 6 The recall of sexual behaviour is influenced by the length of the recall period but also of the frequency of a behaviour. High-frequency sexual behaviours are reported less consistently compared to low-frequency behaviours. The terminology used in questions about sexual behaviour can also influence the response rate. It is also assumed that responses to questions about sexual behaviour are influenced by fear of disapproval from the health worker and that socially desirable answers are given. Some researchers believe that inaccurate reporting of sexual history can be a result of intentional denial of STI. This appeared to be the most plausible explanation in one study, because, gonorrhoea, the most stigmatizing of the STIs, was found to be most underreported by African American adolescent girls 7. However, other explanations such as failure by the provider of the services to create confidentiality and trust, or the characteristics of the interviewer or health care provider are also factors to consider 8. Honesty and respect from the health care provider were highly rated as important prerequisites required in order to obtain truthful answers from respondents. Clark et al speculates that an unknown interviewer could cause some adolescents to hesitate to open up while others could fear to disappoint an interviewer with whom he or she has developed a relationship 9. The same authors also points out that the milieu of the study site also might affect the accuracy of reporting. Even if attempts are made to ensure privacy, this may not always be the teen’s perception. Participants in focus groups have explained that they would not trust health care providers who promised confidentiality but were seen as dishonest or disrespectful 10. In one study adolescents who had been tested for gonorrhoea, chlamydia and trichomonas within the last month tended to underreport their infections 7. Only slight to moderate correlation between selfreported history of pregnancy and STIs and information obtained from medical records was observed in a study of adolescents who were deemed to be at high risk for HIV8. On the other hand, selfreport of condom use was a valid indicator of risk for STIs among adolescents in Minnesota, USA 9where adolescent’s written self-report of condom use was compared to history obtained by clinicians and laboratory diagnosis to assess validity of written self-report. . Research from South Africa has shown that also African adolescents tend to be inconsistent in their reporting of sexual behaviour 11. The only study of reported sexual behaviour, to our knowledge, where face-to face interview is compared to answers to the same questions from a nurse while she was doing the sampling, is the study by Mensch et al 2008. In their study the face-to face interview produced more consistent reporting of sexual activity 12. According to some young women who were consulted after the present study, they were not at all surprised to hear that the answer often was different if given to a social worker or to a midwife. These women were living near the study area but had not participated in the study. They claimed that medical workers often concentrate on symptoms and treatment and they do not probe if the answer to a question is not clear. Social workers on the other hand are used to taking their time and making sure that the client can make herself clear. This means it would be more difficult to come up with an answer which is not truthful if asked by a social worker. Both the young women whom we asked for explanation and the social workers and midwives in the study thought that some participants may have felt that they needed to change the answer when the same question appeared again. Adolescent girls in this setting are unused to talking about sexual matters, which are considered taboo in the Buganda culture10. Additionaly the social workers and the midwives who participated in the study claimed that the social worker could spend more time with the interviewee than the midwife could. Health workers in busy clinics may focus on solving the current situation and do not enter into discussions with clients on how to prevent disease. We conclude that in order to talk about sensitive matters, such as sexual relationship, contraceptive use and the risk of STIs, including HIV, it is necessary to build confidence and trust, which is time consuming. Health workers need to be sensitised to the importance of listening to young clients and compiling all information and clinical findings into an informed decision about treatment. The most prominent risk factor for cervical infection in this study was the information that the partner had symptoms or was recently treated for a genital infection. There is a reason to believe that many young women in this setting are not aware of or informed by their, many times older partners, if he is having any symptoms. However, for those who did know about their partners’ symptoms, this was important information because those who reported that their partner had symptoms or was treated for an STI had a higher rate of infection themselves. Although we are aware of the problems with gender differences and young women not being expected to ask or to question their boyfriend’s /husband’s behaviour, partner’s symptoms should be asked for in a sensitive way and a positive answer should be a reason to treat this woman as if she had an infection. In the interview, the few women who said that they trusted their partner had a low infection rate. Most of the women choose the answer “I don’t know if he is faithful” which was an option given in the interview but not necessarily by the midwife. This might explain the difference in the answers received by the social worker and the midwife. According to the Uganda Demographic and Health Survey 2000-2001, almost 40% of unmarried women age 15 to 19 years were currently using condoms 13. In our study, condom use at latest sexual encounter was reported by 24% only. Among those who reported that they always use a condom there was a tendency to have a reduced infection risk. This finding indicates that information about consistent condom use could be a better predictor of low risk for cervical infection. Less than one-third of participants had been previously tested for HIV. There was a trend towards lower risk for cervical infection, although it did not reach statistical significance, for previously HIV tested young women. We believe that youth who have been HIV-tested generally have a health promoting behaviour. The finding in the present study compares well to findings in a previous study in the same area 14. A purulent discharge was observed in 11.7% (OR 2.0, 95% CI: 0.9-4.3) of the participants. The difference in NG/CT infection rate between women with and without this sign did not reach clinical significance. Nevertheless still, purulent vaginal discharge is known to be a sign of NG/CT infection15. The evaluation of a discharge can be difficult without any laboratory equipment or tests and is dependent on the experience of the examiner. Although we were unable to present a reliable method to identify women with cervical infection we still think that the evaluated risk factors: symptomatic partner, faithfulness, condom use and known HIV status are important issues to discuss during a dialogue between a health provider and adolescents visiting youth facilities or any other health facility especially where the concern is related to genital problems. Conclusion Information about sexual behaviour and experience revealed in this study in individual interviews and in a clinical situation was incongruent. Any approach or flow-chart for management of STIs, which is built on self-reported risk factors, needs careful assessment of reliability. This assessment must be done within the social and cultural context where the flow-chart is intended to be used. Acknowledgement We would like to thank all the study participants and staff at the youth clinics. The study was supported by the Centre for Clinical Research, Dalarna, Sweden and SIDA, Department for Research Cooperation. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11082t3.jpg] [hs11082t1.jpg] [hs11082t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}