 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
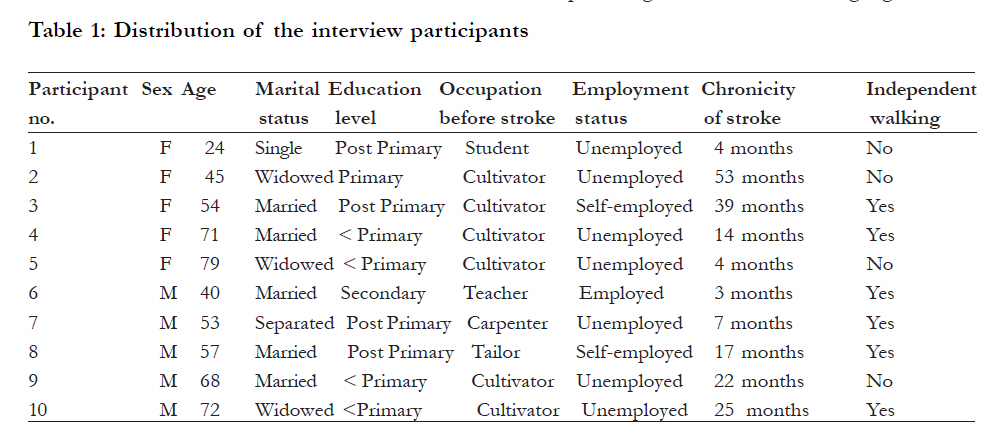
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 398 - 406 Environmental barriers experienced by stroke patients in Musanze district in Rwanda: a descriptive qualitative study *Urimubenshi G1, Rhoda A2 1 Physiotherapy Department, Kigali Health Institute, Rwanda, 2 Physiotherapy Department, University of the Western Cape, South Africa Code Number: hs11084 Abstract Background: Patients with stroke experience a number of environmental barriers, limiting their re-integration. Information regarding the barriers experienced by patients with stroke in a specific setting such as the Musanze district in Rwanda would assist with the development of rehabilitation programmes that would take into consideration the barriers experienced by the clients. Keywords: Stroke, environmental barriers, Musanze district, Rwanda Introduction Stroke is a major cause of long-term disability 1, and has potentially enormous emotional and socioeconomic results for patients, their families, and health services. Although some patients continue to show improvement up to one year after stroke, this does not reach statistical significance for the group as a whole, and between 3 and 5 years many patients experience increasing disability rather than improvement, perhaps due to comorbidity and increasing age2. Stroke patients experience environmental barriers which are often construed as physical but also include prejudice, stereotypes, inflexible organizational procedures and practices, inaccessible information, buildings and transport3. These environmental factors affect activities of daily living and social participation after stroke. Rather than helping, these factors can hinder the accomplishment of daily activities and social roles4, and hence are regarded as barriers. Studies which investigated environmental barriers experienced by stroke patients were mainly conducted in developed countries. The findings from the related studies can be divided into physical, social and attitudinal environmental barriers. Physical environment issues such as inaccessible entryways, bathrooms, and transportation systems, with key barriers including door thresholds and lack of handrails were identified as barriers to community participation among survivors of stroke in the United States5. Negotiating stairs and narrow doorways have also been identified as major barriers to role performance in the home for stroke survivors living in Ontario, Canada6. The reported social environmental barriers experienced by stroke patients include having little social support from friends owing to stroke-related disability and having a limited social network7. According to Chau, Woo and Chang8, social support for stroke patients, whether the support is emotional, informational, instrumental or appraisal, has a positive influence on a stroke patient’s functional and psychosocial recovery. Therefore, lack of social support as experienced by stroke patients would have a negative impact on the psychosocial recovery and reintegration post-stroke. Attitudinal environmental barriers to stroke patients include negative behaviors such as stigma. Stigma towards stroke patients was found in a qualitative study conducted in United Kingdom by Hare et al9 to explore the needs of patients with stroke and their families. The experiences of living with stroke are critical10. According to Ch’Ng, French and Mclean11, understanding the barriers faced by those who have suffered a stroke is useful to identify the longer-term issues that primary care based services for stroke will need to address. There is however a lack of information regarding the environmental barriers faced by stroke patients in some if not all African countries. A study was therefore conducted to explore the environmental barriers experienced by patients with stroke in Musanze district in Rwanda. This information is important as it could assist in the advocacy for services that are effective and appropriate. Background Although data about stroke is available in developed and in some developing countries12, no available study has been conducted on stroke in Rwanda to date. The only statistics by extrapolation estimate the prevalence and incidence of stroke in Rwanda to 1.7% and 0.22% respectively13. These statistics used for prevalence and incidence of stroke were typically based on US, UK, Canadian and Australian statistics, and were automated and did not take into account any cultural, environmental, socio-economic or other differences specific to Rwanda13. According to the experience of the researcher, Ruhengeri Hospital in Rwanda receives many stroke patients, and this indicates a significant incidence of stroke in Musanze district served by the Ruhengeri Hospital. While the evidence accumulated shows that effective stroke rehabilitation requires a multi-disciplinary team and equipped stroke units14, stroke patients at Ruhengeri Hospital are admitted and managed in general medical wards of the internal medicine or intensive care unit departments. Furthermore, the stroke care consists of medical and physiotherapy management only. After observing that the stroke patients are discharged very early and that there is no follow-up rehabilitation post-discharge, the researcher believes that the discharged patients experience many problems. In the absence of data on the potential burden of stroke, though, it is difficult to develop appropriate strategies to prevent stroke and its impact15. Strong et al16 highlight that misunderstandings of chronic diseases such as stroke have contributed to their global neglect. The majority of stroke patients discharged from the Ruhengeri Hospital live in Musanze district. The period following discharge from hospital or from inpatient rehabilitation is the most challenging for almost all stroke patients11. This could be associated with a discharge without accurate assessment of the domestic environment, and the establishment of networks to meet critical needs such as personal care and home modifications. To the researcher’s knowledge, no study has been carried out on the challenges experienced by stroke patients living in Musanze district in Rwanda. The lack of information on the stroke patients’ experiences would be a barrier for planning the appropriate services for them. This would inevitably lead to an increase in suffering, poor coordination and inefficient use of health services, and place the population at the mercy of treatment and prevention strategies with primarily local and/or global commercial interests and with poor outcomes for the patients17. Methods Setting The study was conducted in Musanze district, in the Northern province of Rwanda. The Musanze District is an area which is mainly rural, and where at least 91% of the population is engaged in agriculture18. Musanze district has a total population of over 380,000 having the highest density in the country, 7 that is 70 persons per19 km2. Most families (about 65%) live below the poverty line20. In addition, many families have been destroyed by the 1994 genocide and the repetitive 1997-1998 wars in the region, leaving survivors with disabilities, widows and orphans. Musanze is the most mountainous district in Rwanda21, and therefore has difficult geographical access and transport. In Musanze district, there are neither outreach nor community-based rehabilitation services that are provided to stroke patients and these patients get institution-based rehabilitation services only as inpatients or outpatients. Design A qualitative phenomenological approach was used to collect information regarding the challenges experienced by stroke patients living in Musanze District. Sample, inclusion and exclusion criteria A sample of 10 individuals with stroke living in Musanze district was purposively selected. Characteristics that were considered for the purposively selection were the age, gender, chronicity of stroke, and independent walking. These characteristics were found to be significantly related to positive or negative adjustment and development of self-concept post-stroke22, and would contribute to a richer variation of the phenomena under study23. The chronicity of stroke was calculated as the difference between the date of data collection and the date of stroke onset. Patients who still needed assistance at least for one activity were included. On the other hand, it was necessary to recruit subjects who were able to articulate their experiences and feelings, and accordingly exclude individuals with communication or cognition problems. To obtain respondents with experiences related to stroke, individuals who had suffered other major diseases after the initial stroke were excluded (for example head injury, osteoarthritis and rheumatoid arthritis). Procedure for data collection The study commenced after permission was obtained from the necessary authorities. Interviews were conducted with the 10 participants in their own homes. The researcher contacted the 10 purposively selected patients who met the inclusion criteria to obtain their consent and willingness to participate in the study. The first patient who was contacted, and met the inclusion criteria, and agreed to participate in the study was recruited. To get 10 different participants, other patients were contacted, and those with different characteristics under consideration were recruited. All contacted subjects agreed to take part in the study and were willing and appreciative of the opportunity to relate their experiences. A convenient time and location were determined for the patient interviews, which lasted on average fifty minutes. The interviews were also done in private rooms where the participants had no fear of being overheard by others. The rooms where the interviews were conducted were assessed prior to commencing to ensure good quality recordings , without possible interruptions and distractions. In-depth face-to-face interviews in Kinyarwanda were used to provide descriptions of the informants’ challenges. All interviews were conducted by a researcher. The interviews were guided; an interview guide was developed on basis of the study objectives, the literature, together with the researchers’ experiences. This interview guide was translated from English to Kinyarwanda as the participants were more fluent in Kinyarwanda. Within this frame, the structure of the interviews was designed to be free and open. The relevance, acceptability and clarity of the questions were constantly considered during the conduct of the interviews. During purposeful conversations, information was sought from patients on their environmental challenges experienced. The interviews started with a ‘grand tour’ question to set the tone of the interview, and to let the participants determine what was important for them to tell about barriers while living with a long-standing disability24. Therefore, participants were asked to tell the story of their stroke and the way it had affected their lives, beginning with the question: “Please tell me about any problems you are having since you got stroke”. The remainder of the interview guide consisted of a series of guided probes that endeavored to obtain an in-depth description of the environmental challenges experienced. All interviews were audiotape-recorded, and the research assistant took field notes. Data analysis The tape-recorded interviews in Kinyarwanda were transcribed in full by the researcher. A trained, multilingual translator translated the transcriptions into English and the researcher analyzed those transcriptions to identify the main patterns of responses, consistencies and divergences across participants25. Common concepts were coded as suggested by Miles and Huberman26, producing themes that were then classified into major themes and sub-themes27. Two weeks after the initial coding, another separate coding was done and the generated sub-themes and themes in the second coding were then compared with the initial coding. This led to further refinements, producing sub-themes and themes that were interpreted for the meaning of the content. The environmental barriers expressed by the participants were grouped into three major themes which are social, attitudinal and physical environmental barriers as conceptualized in the International Classification of Functioning, Disability and Health (ICF) 28. Ethical Considerations Ethical clearance for the study was obtained from the Senate Research grants and study leave Committee at the University of the Western Cape. In addition permission to conduct this study was obtained from the National Ethics Committee of Rwanda and the Mayor of Musanze district. Written informed consent was obtained from guardian and the participant. Participation in the study was voluntary, and the participants were informed of their right to withdraw from the study at any time. The participants were told that if anything happened to upset them, counseling services were available for them. Results Five participants (50%) were females and other five (50%) were males. The participants were aged between 24 and 79 years (mean age = 56.3years, SD = 16.9 years). Half of the participants (50%) were married while three (30%) were widowed. The chronicity of stroke among the participants lies between 3 and 53 months (mean = 19 months, SD = 16.4 months). Only half of the participants (50%) had more than primary school education. Only 60% of the participants were able to walk independently. Eighty percent of the participants were involved in manual activities before the stroke, and the majority (60%) among them were cultivators before getting stroke. In Rwanda, agriculture is mainly for subsistence and is associated with low socioeconomic status. At the time of interview, the majority of the participants (70%) were unemployed. Out of 10 participants, only one lived in a house with a toilet inside. Others were living in houses with toilets outside in form of latrine. During the interviews, the participants were open to respond to the researcher’s questions. The feelings from the participants that emerged during the interviews as environmental barriers can be classified into three major themes which are social, attitudinal and physical barriers. The sub-themes emphasizing each theme will be highlighted [Table - 1]. Social barriers The subthemes related to social barriers as described by the participants were lack of social support and inaccessible physiotherapy services. Lack of social support There were mixed feelings with regard to social support. When asked if the society was supporting them, the participants described family members and other people to be supportive, but some participants reported lack of support from the relatives since having stroke, and others felt that the support was decreasing as time progressed. For example, a participant said that she was not supported by the family members: “All my relatives have turned away from me…they do not care for me. I look after myself because I don’t have anyone to take care of me” (P2). Some participants emphasized in common that as the period of the disease lengthened, social support became less frequent as illustrated by the following quotes: “ … at the beginning, people were highly willing to help me, I was being helped by relatives and volunteers, but as it took a long time, they became tired, and often they no longer come to visit me” (P4). “… sometimes, people used to come and help me to go to church to pray and this was for two years. After that they stopped and I no longer go to church” (P2). “ … now, I do not respect the physiotherapy appointments because my parents cannot continue to pay the transport fees three times a week…just after I got sick they were able to pay all the transport fees three times a week, but now they cannot…money is finished” (P1). Inaccessible physiotherapy services Many participants expressed that they could not attend physiotherapy out-patient sessions due to problems of accessibility. This was expressed with regard to the limitations in walking and the high cost of transport. The following quotes illustrate the problem: “When I was discharged from the hospital, the doctor told me to continue physiotherapy for three times a week. Oh, it is hard for me! I cannot walk...my caregiver and I need transport to reach there, and it is very expensive” (P5). “…my first problem now is to get a ticket to continue physiotherapy….I go to the hospital three times a week, but it is very far from my home and the transport is very expensive….It is RWF 2400 (= USD 5) per week” (P9). “ … the hospital is very far, and the transport to go there for physiotherapy is very expensive … To go to the hospital every single day is RWF (Rwandan Francs) three thousand, it means RWF nine thousand every week (= US Dollars 17 by the interview period), the money is finished. I decided to get a private home physiotherapy treatment as it becomes cheaper, but sometimes the physiotherapist does not come” (P7). Attitudinal barriers The perceived attitudinal barriers were related to people’s negative attitudes, although not frequent. These attitudes varied from people who said that the stroke patients were being punished by God, to those who felt happy after their rivals in achievements got stroke. P2 reported: “People are saying that God has punished me”. P3 also perceived negative attitudes from others. The participant said: “When I got sick, some people felt bad, but others felt very happy, for example those who were jealous of my achievements, now they feel happy”. Physical barriers There were frequent expressions from the participants with regard to physical barriers. The subthemes which emerged from the interviews as related to physical barriers included inaccessible pathways and toilets. Inaccessible pathways When probed about factors that were obstacles in their daily life, participants also mentioned problems with physical accessibility. The barriers which were described are stones, stairs and uneven grounds. These are illustrated by the following quotes: “ … I stay at home; I cannot go anywhere unless I have someone to assist me … When I am in a wheelchair I cannot push it myself because of stones and stairs within the ways I use” (P2). “………….I can walk with a stick, but it is not possible when there are stairs” (P6). “… I walk very slowly … I am no longer able to walk for a long distance. As the ways in our village are eneven with many stones, when I am walking even with a stick, it is very difficult, and I become tired in short time” (P10). Inaccessible toilets Some participants indicated that they had a problem with the use of toilets, as these were not accessible. This was related to the physical construction of the toilets, and some participants revealed the coping strategies they developed. “… I cannot go to that toilet…I do my toilet in bed, and my children do cleaning” (P 9). “ … I cannot really be able to tell you what problems came with this disease. I am struggling to live … I have difficult to go to toilet … There at Kigali (the capital of Rwanda with better accessible physical environment) where I have been before, there are modern toilets I could use easily, here I have to use a tablet” (P7). “ … It is hard for me to go to the toilet. The toilet we use here demands squatting and I cannot …I use a chair” (P8). Discussion The aim of the study was to explore the environmental barriers experienced by patients with stroke in the Musanze district in Rwanda. Identified barriers included social, attitudinal and physical barriers. Social barriers The interview findings related to the lack of social support are consistent with other research findings where the lack of social support was a frequent experience of stroke patients11,29. For example, Lynch et al29, in their qualitative study in US on dimensions of quality of life that are important to patients after stroke, found that lack of social support was one of the experiences of the stroke patients. This challenge related to the lack of social support from family and friends was particularly mentioned by all the unemployed participants (P1, P2, and P4) as the help of a family member to access medical care and provide practical help was important. Some participants expressed that the support became less and less as the period of their disease became longer. It was found that the mean of chronicity of stroke was 19 months among the interview participants. This period is very long when a patient is supported by others, especially when these are volunteers and not relatives. They may become tired and stop their support. The findings supported Dorsey and Vaca30 who noted that as time passes, social activities and contacts with stroke survivors begin to diminish. Literature highlights the important role of social support in stroke rehabilitation10. Results from quantitative studies indicated that the social support has a positive influence on a stroke patient’s functional and psychosocial recovery8,10. As the current study population is composed of vulnerable individuals with low socio-economic status, some being widowed and old, in addition to the acquired poststroke disability, the lack of social support would be a barrier to the emotional, informational, and instrumental or appraisal support that they need. Consequently, the lack of social support would have a negative impact on their functional and psychological recovery, and social reintegration poststroke. Therefore, measures to encourage social support for people with stroke in Musanze District are suggested. Lack of transport to access physiotherapy services was also expressed by the participants as a challenge experienced and was particularly raised by the participants who were unemployed (P5 and P9). The participants’ expressions regarding the lack of transport to access physiotherapy rehabilitation were consistent with the findings from the in-depth interviews in New Zealand used to explore the perceptions of individuals with stroke towards outpatient physiotherapy in the hospital, and homebased settings31. Similarly, the participants who were part of the study conducted by Hale et al31 expressed that it was difficult for them to attend outpatient physiotherapy in the hospital due to lack of transport31. The situation of the current study participants was more difficult as these were poor and were no longer involved in income generating activities and they could not find themselves money for transport. In other countries like Turkey, Thailand, Brazil, United States and Italy, stroke patients, after the clinical stability of stroke is achieved in an acute treatment hospital, are ushered into rehabilitation settings32. In Rwanda, there are no such rehabilitation settings for stroke patients, and these are discharged to their homes. The United Nations (UN), in its Standard Rules on the Equalization of Opportunities for Persons with Disabilities (PWDs), recommends that states should ensure that all rehabilitation services are available in the local community where the PWDs live33. However, in Musanze District, there is no provision of home-based, outreach or communitybased rehabilitation programmes, and PWDs can only get the rehabilitation services at the hospital as outpatients. Broadly, PWDs in Rwanda share the same difficulties that other Rwandans without disabilities face in accessing health care, but there are some differential factors. For example, most of the current study participants need assistance to reach health facilities. According to the Ministry of Health34, only 5% of Rwandan PWDs are able to access the services they need. The inaccessibility of physiotherapy services as experienced by the study participants is likely to interfere with the functional outcomes, social participation and social reintegration, and would increase other medical complications32. Therefore, the study results emphasize the need of provision of transport facilities, home-based or community-based rehabilitation programmes for stroke patients. Attitudinal barriers It has been hypothesized that stroke is a stigmatizing condition35, and this has been supported by the study findings as the participants explicitly drew attention to the negative attitudes although not frequent. The negative attitudes perceived by the participants were similar to qualitative findings in a study conducted by Hare et al. 9 in the UK. According to Thomas36, PWDs in Rwanda face negative attitudes, and these are particularly strong towards those with severe disabilities. In the present study, it was found that participants who reported experiencing negative attitudes are those with low education level (P3) and the unemployed (P2). Thomas36 also found that persons with low education level and economic status in addition to disability experience negative attitudes more than those with a higher education level and economic status. The negative attitudes as perceived by the participants could result in social isolation for people with stroke, and these may start themselves to avoid deliberately meeting other people9. Physical barriers The participants’ expressions on inaccessible pathways were in agreement with the reports from a study conducted in Canada by Reid37. In this study, it was found that the outside of the home poses barriers to occupational performance for many individuals with stroke, with key issues including uneven ground and stair access37. Also, Udesky38 highlighted that for many people who have had a stroke, simply walking again can be extremely difficult, and if there are steps to climb or narrow doorways to pass through, it may seem totally impossible. The present study findings suggest that the physiotherapists should visit the stroke patients’ homes to check for potential hazards like stairs and indicate changes to make getting around the houses easy and safe. Given the fact that the paths in the Musanze district are made of stones, and that the Musanze district and the Government of Rwanda are not maybe ready (due to financial reasons) to build better accessible paths or roads, efforts should be put in re-education aiming at the walking performance in the patient’s community. However, transport facilities to overcome the physical barriers, and to assist the people with stroke to get out the house and take part in social activities are also suggested. The challenge related to the accessibility of the toilets was also mentioned by Stein39 who said that after a stroke, some people have difficulty rising from a standard height toilet owing to weakness. The Australian Human Rights Commission40 reported a woman who had a stroke and who was complaining that there was no accessible toilet at a local arts theatre. The participants’ expressions on inaccessible toilets could be expected as most of them live in houses with toilets outside, in form of latrine. However, as also pointed out by Stein39, participants with higher education level like P7 and P8, compared to other participants like P9, revealed some strategies they adopted to find practical solutions to the physical barriers they experienced, such as using a chair or a tablet for being able to use the available toilets. The inaccessible toilets as felt by the participants is a factor for more dependence in self care activities with patients being more psychologically affected owing to their status of dependence. Given the physical construction of the toilets in many rural areas like in Musanze district which is not accessible to people with stroke, and given the fact that the majority of the families are not able to get the modern accessible toilets, during rehabilitation of stroke patients emphasis should be to minimize the dependence for using the available toilets, maybe in encouraging and improving the coping strategies as revealed by the participants. Study limitations The limitations of the study are the following: (i) Individuals with communication or cognition problems were excluded from the interview sample; therefore, the sample may only represent a group of individuals with no significant communication or cognition problems poststroke while the excluded group might have different experiences; Conclusion The study findings revealed that after the discharge from the hospital to their homes, stroke patients experience various environmental barriers ranging from social to attitudinal and physical barriers. These barriers could heavily impede the functional and social activities among the stroke survivors. The findings of this study highlight the need for interventions that include awareness and education of communities about disability and advocating for accessible services and physical structures for persons with disabilities living in this geographical setting. Authorities responsible for development programmes should pay special attention to the involvement of the stroke survivors and put income generating activities in place as it is difficult for them to return to their previous manual occupations such as agriculture. Acknowledgements We are most grateful to the authorities who gave us the permission to conduct such a study. We highly thank the participants who accepted to participate in this study and all who assisted us in one way or the other. References
Copyright © 2011 - African Health Sciences The following images related to this document are available:Photo images[hs11084t1.jpg] |
| |||||||||

{kind=link}