 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 414 - 420 Metabolic syndrome in Tunisian bipolar I patients *Ezzaher A1,2, Haj Mouhamed D1, Mechri A2, Neffati, F1, Douki W1, Gaha, L1, Najjar MF1 1 University Hospital of Monastir, Laboratory of Biochemistry-Toxicology, 2 Research Laboratory “Vulnerability to Psychotic disorders LR 05 ES 10 “, Department of Psychiatry. University Hospital of Monastir Code Number: hs11086 Abstract Background: The metabolic syndrome is a growing global public health problem which is frequently associated with
psychiatric illness.
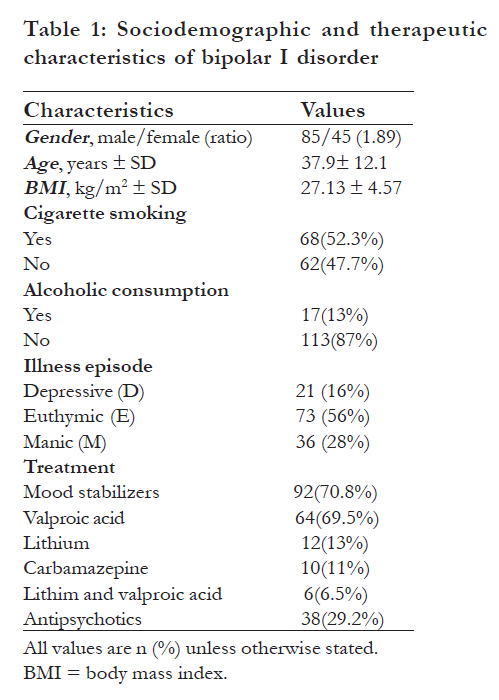
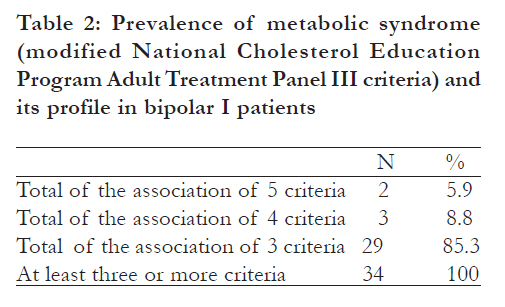
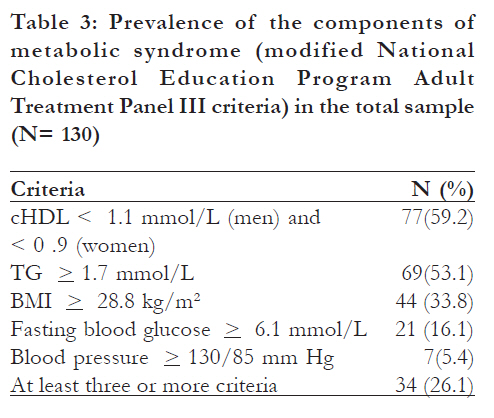
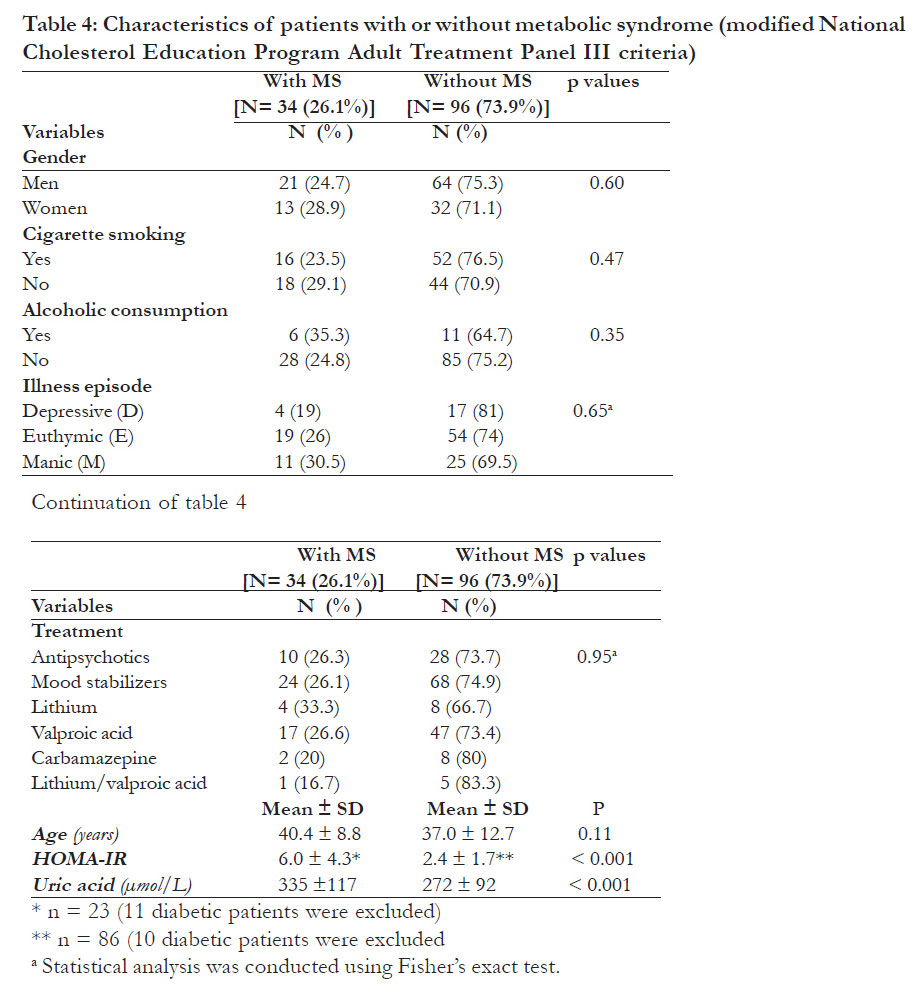
Bipolar disorders are common conditions, affecting approximately 3.5% of the population, and are characterized by recurrent episodes of depression and mood elevation1. It is a chronic disease that is associated with a potentially devastating impact on the patients’ wellbeing and social, occupational, and general functioning2. The disorder ranks as the sixth leading cause of disability in the world, with an economic burden that in the US alone was estimated more than a decade ago at $7 billion in direct medical costs and $38 billion (1991 values) in indirect costs3. Patients with bipolar disorder are known to suffer a considerable number of associated pathologies that may manifest at earlier ages and with higher frequency than in the general population4. The most recent studies have explored cardiovascular risk and the association with metabolic and endocrine disorders fundamentally, obesity and metabolic syndrome which are clearly associated with the development of cardiovascular disease5. The metabolic syndrome is composed of a number of risk factors including insulin resistance, abdominal obesity, dyslipidemia, and hypertension and is associated with an increase in morbidity and mortality6. Various studies conducted in bipolar patients report prevalence of metabolic syndrome rates from 1625% in European subjects7, 8 to 30-49% in U.S. subjects6, 9. Although, data in African area remain scarce,some studies performed in the African-American patients reported prevalence rates from 22.5% to 44%6, 10. This study aims to evaluate the prevalence of metabolic syndrome and to study its profile in 130 Tunisian bipolar I patients. Methods Patients This study was approved by the local ethical committee of Monastir University Hospital, and all subjects were of Tunisian origin. The sample included 130 bipolar I patients from the psychiatry department of the Teaching Hospital of Monastir with depressive (D=21), manic (M=36) or euthymic (E =73) episode. Patients included in the study were required to receive medications (mood stabilizers: valproic acid, lithium and carbamazepine, and classical or atypical antipsychotics such as risperidone or olanzapine) for at least three months. The mean age was 37.9 ± 12.1 years, with 45 women (37.5 ± 13.4 years) and 85men (38.1 ± 11.4 years). Consensus on the diagnosis, according to the diagnostic and Statistical manual of Mental disorders, fourth edition (DSM-IV) criteria 11, was made by psychiatrists. The exclusion criteria were age (<18 years), other psychiatric illnesses, epilepsy or mental retardation. All subjects were questioned about their age, gender, previous treatments and cigarette and alcohol consumption habits. The clinical and sociodemographic characteristics are shown in [Table - 1]. Samples After a 12 hour overnight fasting, venous blood for each patient was drawn in tubes containing lithium heparinate and immediately centrifuged. The plasma samples were stored at -20°C until the biochemical analysis. Biochemical analysis Metabolic syndrome (MS) was defined according to the National Cholesterol Education program (NCEP) Adult Treatment panel (ATP) III modified criteria and required fulfillment of at least three of the following five components: body mass index (BMI) > 28.8 kg/m2, triglycerides > 1.7 mmol/L, high-density lipoprotein cholesterol (c-HDL) < 1.1 mmol/L (men) and < 0.9 mmol/L (women), blood pressure > 130 D 85 mmHg, and fasting glucose (> 6.1 mmol)12. Concentrations of triglycerides, c-HDL, fasting glucose and uric acid were determined by enzymatic methods using Konelab 30 equipment (Thermo Electron Corporation, Ruukintie, Finland). Insulin was determined using chemiluminescence (Elecsys 2010TM Roche diagnostics). Data measures Insulin resistance (IR) was estimated using the Homeostasis model of assessment equation: HOMA-IR = [fasting insulin (mU/L) × fasting glucose (mmol/L)] /22.5. The IR was defined as the upper quartile of HOMA-IR. Values above 2.5 were taken as abnormal and reflect insulin resistance13. Bipolar patients with diabetes (n = 21) were excluded in the HOMA-IR analysis. The BMI was calculated as weight (kg) divided by height (m2). Obesity was defined when BMI was > 28.5 kg/m2 12. Statistical analyses Statistical analyses were performed using SPSS v. 17.0 (SPSS, Chicago, IL, USA). Quantitative variables were presented as mean ± SD and comparisons were performed using the Student’s t test. Qualitative variable comparisons were performed using the chi square test and Fisher’s exact test (when cells with n < 5). The statistical significance level was set at p < 0.05. Results In our study, the prevalence of metabolic syndrome in bipolar I patients was 26.1% [Table - 2]. The highest prevalence of this syndrome was obtained by the association between obesity, low c-HDL and hypertrilyceridemia (44.1 %). In the total sample, the prevalence of individual diagnostic components was as follows: 59.2% for low c-HDL, 53.1% for hypertriglyceridemia, 33.8% for obesity, 16.1% for high fasting glucose and 5.4% for hypertension [Table - 3]. We found that gender was not associated with metabolic syndrome, 24.7% in men and 28.9% in women. As to age, we found that patients with metabolic syndrome were older than metabolic syndrome free patients (40.4 ± 8.8 years Vs 37.0± 12.7 years), but this difference was not significant. Cigarette smoking and alcoholic consumption were not significantly associated with metabolic syndrome; however, we showed that approximately a quarter (23.5%) of smoker patients and a third (35.3%) of alcoholic consumer patients had metabolic syndrome [Table - 4]. Our present data showed that there is no difference in metabolic syndrome prevalence between patients receiving antipsychotic and mood stabilizers treatment. However, we noted that patients treated with lithium had the highest prevalenceof metabolic syndrome. Our study failed to show any significant association between metabolic syndrome and illness episode, whereas, manic patients had the highest prevalence of this disorder (30.5%). Patients with metabolic syndrome had significantly higher levels of uric acid (p < 0.001) than metabolic syndrome free patients. Concerning HOMA-IR analysis, after diabetic patients exclusion (n = 21), we noted that patients with metabolic syndrome had significantly higher levels of HOMA-IR (p < 0.001) than metabolic syndrome free patients. Discussion To our knowledge, this is the first study to examine the prevalence and correlates of metabolic syndrome in Tunisian patients with bipolar I disorder. Using the ATP-III definition, we found that the prevalence of metabolic syndrome was 26.1% among patients, (24.7% in men and 28.9% in women). These prevalences were definitely higher than those reported in the Tunisian general population (13% in men and 18% in women) using a previous criteria 14. Compared with others studies, the prevalence of metabolic syndrome in our patients is between thatin Spanish patients (22.4%)15, Italian patients (25.3%)8 and US patients (30%)9. The highest prevalence of metabolic syndrome was obtained by association between obesity, low c-HDL and hypertriglyceridemia, confirming the high risk of dyslipidemia and obesity in bipolar I patients16. There is a need for psycho educational programmes including healthier eating habits and lifestyle advice for patients with bipolar disorder. Furthermore, effective programmes aimed at early detection and adequate treatment by the psychiatric team should be considered. Implementation of programmes that emphasise lifestyle modification to reduce weight in overweight/obese patients can positively influence many components of metabolic syndrome15. Moreover, when analyzing the prevalence of the single components of metabolic syndrome in the total sample, we found that lipid disorders (low c-HDL and hypertriglyceridemia) and obesity were the most common abnormalities. This is in line with results reported by Garcia- Portilla et al 15. We found that 59.2% of bipolar patients met the criteria of low c-HDL, 53.1% of hypertriglyceridemia and 16.1% of high fasting glucose, which are higher than in Italian8 and in US patients9 (23%, 48% and 11%; 36.1%, 38.2% and 8% respectively). However, the prevalence of obesity (33.8%) and hypertension (5.4%) in our patients were lower than in Italian patients (50% and 40% respectively)8 and US patients (49% and 39% respectively)9.These differences could be due to ethnicity and eating habits. Concerning socio-demographic characteristics, there was no significant difference in the prevalence of metabolic syndrome among gender and age. This is in line with results reported by Yumru et al 17. Cigarette smoking was not significantly associated with metabolic syndrome, but we showed that approximately a quarter of smoker patients had metabolic syndrome. There are several possible explanations for the association between smoking and metabolic syndrome in former smokers. First18, mechanisms for these long lasting effects of smoking on insulin resistance may include vascular changes that lead to decreased glucose uptake by skeletal muscle. Second19,20, smoking increases the circulating white blood cell count, a marker of inûammation, in subjects undergoing general health screening. It is possible that proinflammatory cytokines, such as tumor necrosis factor-á may explain the association between smoking, increased white blood cell count, and metabolic syndrome. Third21, 22, both current and former smoking are negatively associated with plasma levels of adiponectin. Decreased adiponectin is thought to play a major role in the development of insulin resistance; thus, it may be an underlying mechanism of metabolic syndrome in smokers. We found that alcoholic consumption is not significantly associated with metabolic syndrome propably because of the small size of alcoholic consumer patients (n = 17). However, we showed that approximately a third of alcoholic consumer patients had metabolic syndrome. Some studies have shown positive association, whereas others have observed a negative association or no relation at all23 .. This irregularity in results could be related to the complex mechanistic relation between alcohol consumption and each component of metabolic syndrome. While mild to moderate alcohol consumption has a favourable influence on lipids metabolism, abdominal obesity and glucose regulation, excessive alcohol consumption causes hypertension and hypertriglyceridemia constituting alcohol-related metabolic syndrome23. We noted that there was no significant change in the prevalence of metabolic syndrome in relation to illness episode; however, manic patients had the highest prevalence. This may explain the high risk of cardiovascular disease in manic patients compared with depressive one24. Additionally, Angst et al 25 showed that individuals with bipolar I disorder are at greater risk for cardiovascular mortality than individuals with bipolar II disorder. However, the difference in cardiovascular mortality between the two bipolar subtypes reflects the manic symptom burden, which predicts cardiovascular mortality independently of diagnosis and cardiovascular risk factors at intake. The results suggest that mania, either directly (through factors intrinsic to illness) or indirectly (through other mediators or associated variables), may itself influence cardiovascular disease. Our study failed to show any significant association between metabolic syndrome and treatment. However, we noted that patients treated with lithium had the highest prevalence of metabolic syndrome. The increased risk to develop metabolic syndrome during treatment with lithium is in part related to its propensity to induce weight gain. According to Casey26, lithium has been shown to stimulate appetite and increase calorie intake through different mechanisms. The HOMA-IR is significantly higher (p < 0.001) in patients with metabolic syndrome than others. This increase in HOMA-IR values reflects an insulin resistance and is associated with two to three fold increases in cardiovascular disease independent of classical risk factors 27. In addition, uric acid levels were significantly higher (p < 0.001) in patients with metabolic syndrome. According to Vuorinen-Markkola et al 28, hyperuricemia forms another consistent feature of the metabolic syndrome which led to the suggestion of uric acid being a new component of the syndrome. In addition, Chien et al29 reported that metabolic syndrome induces high oxidative stress and the accompanying hyperuricemia worsens this stress. Furthermore, uric acid stimulates vascular smooth muscle proliferation, induces endothelial dysfunction, decreases endothelial nitric oxid production, and consequently, makes peripheral tissue resistant to insulin effects and results in endothelial dysfunction 29. High levels of uric acid are associated with increased renal glomerular pressure and sodium reabsorption, enhanced by high insulin concentrations23 .. In addition, hyperuricemia was associated with insulin resistance markers, including triglycerides, microalbuminuria and impaired glucose tolerance. These disturbances contribute to increase cardiovascular risk29. This insulin- resistance causes steatosis, which is associated with hyper secretion of hepatic enzymes30. Several methodological limitations should be considered when interpreting these findings. First, a larger sample size of groups would be beneficial. Second, our work is a cross-sectional study that does not permit follow-up of biological parameters. Finally, the sample of bipolar patients may not be representative of more heterogeneous populations. Tunisian bipolar I patients have a higher prevalence of metabolic syndrome compared with the general population. The highest prevalence of this syndrome was obtained by association between obesity, low c-HDL and hypertrilyceridemia. Age, gender, illness episode, and treatment were not significantly associated with metabolic syndrome; but insulin resistance and uric acid were significantly associated with this syndrome. The combination effects of these parameters on metabolic syndrome results in high cardiovascular risk. Conclusion Bipolar patients require specific care, particularly for lipid profile and weight. The effectiveness of this care will be evaluated during follow-up period. . Acknowledgements The authors thank the patients and control subjects for their assistance in this study. AE conceived the study, gathered and managed the data, carried out the immunoassays, performed the literature search and statistical analysis and wrote the paper. DHM participated in the literature search, the management of the data, statistical analysis and writing of the paper. AM contributed to the clinical and rating evaluations during the follow-up periods, participated in the statistical analysis and in correction of the final manuscript. FN participated in carrying out the immunoassays. WD participated in designing the study, analysing the data, writing the paper and in correction of the final manuscript. LG contributed to the clinical and rating evaluations during the follow-up periods. MFN participated in designing the study, analysing the data, writing the paper and in correction of the final manuscript. All authors read and approved the final manuscript. References
Copyright © 2011 - African Health Science The following images related to this document are available:Photo images[hs11086t4.jpg] [hs11086t2.jpg] [hs11086t3.jpg] [hs11086t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}