 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
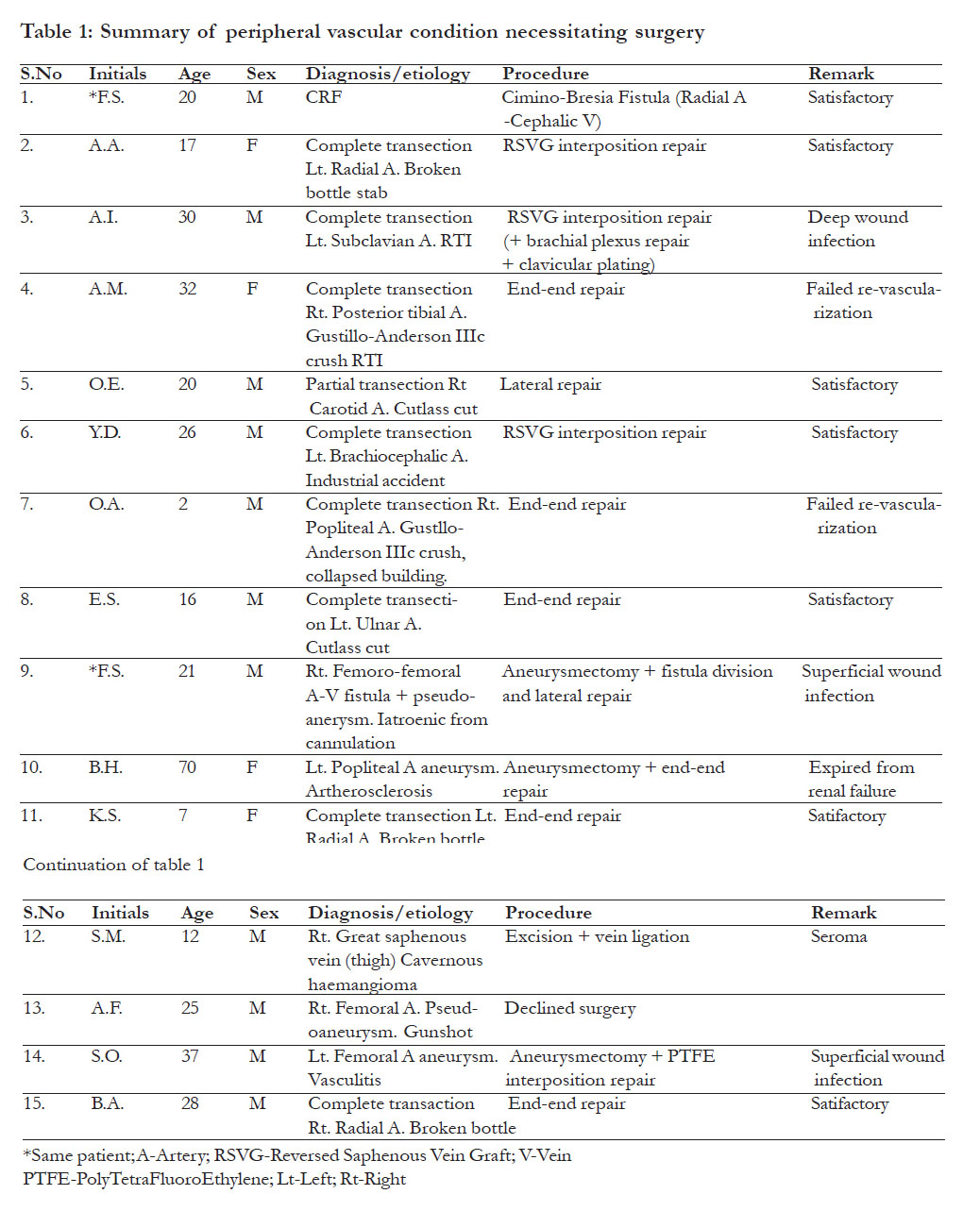
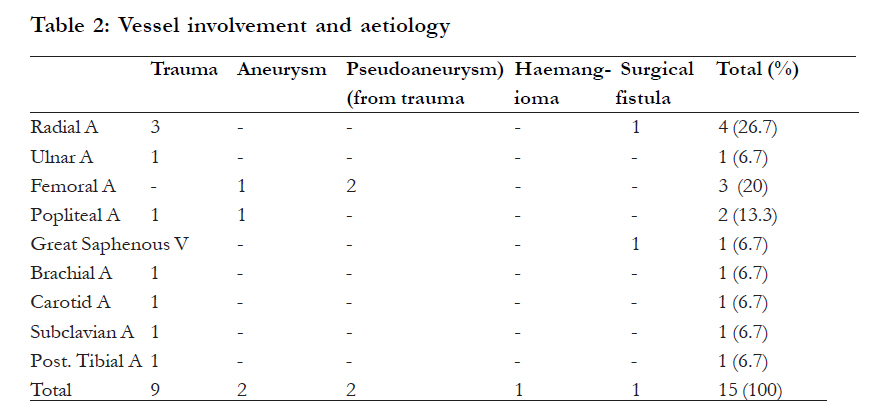
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp. 433 - 437 Peripheral vascular surgical procedures in Ilorin, Nigeria: indications and outcome *Adeoye PO1, Adebola SO2, Adesiyun OAM3, Braimoh KT3 1 Departments of Surgery, University of Ilorin Teaching Hospital, Ilorin, Nigeria, 2 Departments of Otorhinolaryngology, University of Ilorin Teaching Hospital, Ilorin, Nigeria, 3 Departments of Radiology, University of Ilorin Teaching Hospital, Ilorin, Nigeria Code Number: hs11089 Abstract Background: Data on peripheral vascular surgical interventions from Nigeria is scanty. Reports form Western and Eastern Nigeria dates back about twodecades. This study therefore analyses the various etiological conditions necessitating intervention, and their outcome. Key words: Peripheral vascular surgery, vascular trauma, Ilorin Introduction Peripheral vascular conditions requiring surgical intervention are multivarious and so are the surgical techniques employed. Most developed countries, in view of their comparatively older patient population, record high incidence of artherosclerotic disease in contrast to developing countries where traumatic events predominate1,2. In a world where trauma is assuming epidemic proportions, the mechanism by which it is inflicted also varies from society to society3. Where guns are permitted amongst civilians, vascular injuries resulting from gun shots may be seen more frequently, and sometimes the injuries may mimic those seen in conflict zones. This report from an urban setting of North-Central Nigeria is aimed at complementing earlier reports from thewestern and eastern parts of the country1,4,5. Methods This retrospective study therefore evaluated the various etiological conditions and surgical interventions offered to patients who presented with peripheral vascular conditions. The burden of vascular trauma in our environment is highlighted. Patients who had surgical intervention on peripheral vessels between July 2006 and June 2008 at the University of Ilorin Teaching Hospital were included in this retrospective analysis. Diagnosis was made by clinical evaluation in conjunction with plain roentgenography, doppler ultrasonography, venography or CT-angiography as indicated. Procedures were performed under general anaesthesia. Limb tourniquet was employed when there was active bleeding. Distal vessel embolectomy was performed using size 6Fr or 8Fr Foley’s urethral catheter followed by flushing with heparinised saline (5, 000 I.U. in 50mls) via size 5Fr feeding tubes. When the vessel calibre was too small to admit Foley’s catheter, flushing alone was employed. We adopted this technique for embolectomy due to lack of Forgathy embolectomy catheter in our practice. A lower limb was routinely prepared in anticipation of the eventual need for saphenous vein harvest. Post operatively, patients were placed on antibiotics and were anticoagulated for 72hours except longer administration was indicated by other clinical conditions. Low dose aspirin was administered for 1 month except in one patient with PolyTetraFluoroEthylene (PTFE) graft who had it for up to one year. Presence of distal pulsation, capillary refill, warmth and colour were employed to assess success of revascularization. Few patients had post-operative doppler ultrasonographic assessment because it was not usually available for our use. Patients’ demographic data, the etiologies of the vascular condition, mechanism of injury, surgical procedure performed, and outcome were documented and subsequently analysed using SPSS version 15.0 windows (SPSS Inc, Chicago, Il, USA) statistical package. Results A total of 14 patients presented with 15 peripheral vascular conditions requiring surgical intervention over the two-year period. Fourteen of these were operated. There were 10 (71.4%) males and 4 females (28.6%), M: F = 2.5: 1. The age range of the patients was 2-70yrs (mean = 24.4 ±SD 16.3) majority of whom were aged 20-29yrs (5, 35.7%). The age groups 10-19yrs and 30-39yrs accounted for 3 patients (21.4%) each. Two patients (14.3%) were under 10yrs and 1 (7.1%) was 70yrs. [Table - 1] provides a summary of all the patients. The commonest etiological factor was acute trauma accounting for 60% [Table - 2]. The only venous pathology was a cavernous haemangioma of the great saphenous vein in the right thigh. A patient with chronic renal failure (CRF) initially had no direct vascular pathology but required creation of Cimino-Brescia fistula for haemodialysis; he subsequently developed right femoro-femoral artero-venous fistula with pseudo-aneurysm of femoral vein as a complication of a previous cannulation for dialysis [Table - 1].When the 2 traumatic events complicated by pseudoaneurysm were combined to the acute traumatic presentations, trauma accounted for 73.3% of cases. [Table - 2] shows the vessels involved by the various etiologies. Direct repair was performed in 9 (64.3%) of the 14 operations performed, including 6 end-to-end anastomoses, 2 lateral repairs, and 1 side-to-side anastomosis (for fistula creation). Interposition graft was employed in 4 (28.6%) cases using reversed great saphenous vein (RGSV) in 3 and PTFE vascular graft in 1. The ends of the great saphenous vein were ligated after excision in the case with cavernous haemangioma. Most procedures involved the radial artery 4 (28.6%). There were 2 (13.3%) each of femoral and popliteal arterial procedures while carotid, subclavian, brachial, ulnar, and posterior tibial arteries and great saphenous vein accounted for one (6.7%) each. Major morbidity was recorded in 3 (21.4%) cases. Deep wound infection occurred in 1 patient who had contaminated supraclavicular wound from Road Traffic Injury (RTI) and required nerve repair and fixation of fractured clavicle in addition to vascular repair. Two patients had failed revascularization. Minor complication included superficial wound infection in two patients and seroma in one patient. Mortality rate of 7.1% was recorded. This occurred in the 70yearr old woman with popliteal artery aneurysm. Discussion Peripheral vascular conditions requiring surgical intervention vary in different parts of the world. However, trauma has been identified to be a major indication for intervention as vascular injuries may result in severe complications though they constitute only 3% of all traumatic events3,6. Peripheral vessels are affected in about 80% of vascular injuries7. Two of four patients who had peripheral arterial repair in Adebo et al’s report had lesions secondary to trauma5. In our review, 73.3% of cases with peripheral vascular conditions necessitating surgery had etiologies related to trauma. Urbanization with its attendant increase in violence or conflict and RTI may account for this. The majority of these injuries are due to penetrating trauma, with stab, gunshot wounds and road traffic crashes being the most common causes8,9. While Singh and Rk reported 59% to arise from penetrating injury in India3, Niels reported 70-90% from the United States of America (USA)7 and it accounted for about 67% of our cases. Unlike in the USA where gunshots are the culprit in 70-80%7, India reported a similar distribution with us where stabs and RTI are more prominent3. One patient from our study had iatrogenic injury. This reflects the low volume of vascular catheterization procedure performed in our centre. While Neils reported a 5% incidence of iatrogenic injuries7, Shalkow from Mexico reported up to two thirds of paediatric arterial injury being iatrogenically inflicted and 26-67% of arterial injuries resulting from transfemoral cardiac catheterization10. Artherosclerosis was found in only one patient who presented with popliteal artery aneurysm. In the western world, artherosclerosis affects 10% of the population over 60 years2. It accounts for up to 100, 000 surgical procedures performed per year in the USA11. Hence if the life expectancy in our society (currently about 47 years12) improves, then we may see more peripheral arterial diseases secondary to artherosclerosis and requiring surgery. The radial artery was the most common vessel requiring surgery from our study. Fifty-eight percent of injuries involved the lower extremity vessels in the report by Singh and Rk3, but it was about 36% from our study (with inclusion of the 2 late complications of trauma causing pseudoaneurysm). Most peripheral vascular surgical procedures involved direct repair (64.3%). This is supported by Singh and Rk’s report of 68.8% and Adebo’s documentation3,9. In 4 cases where direct repair was impossible the RSVG was helpful in 75%, with only one patient requiring a PTFE vascular prosthesis. Our limb salvage rate amongst all operated cases was 85.7%, but was 77.8% amongst acute traumatic cases. Factors responsible for failed re-vascularization in 2 cases were extensive crushing injury (Gustillo-Anderson 3c class) and delayed injury-intervention time (> 6hrs). However, in repairs of ulnar or radial artery the presence of collateral circulation is expected to maintain adequate supply. Pulsation of the repaired vessel was however restored. The only mortality recorded resulted from renal failure due to extensive atherosclerotic disease in the 70-year-old lady with popliteal aneurysm. Conclusion Despite the varied presentations of peripheral vascular conditions, trauma still presents a major problem in our environment. It must be approached promptly to avoid debilitating morbidity and mortality. While most repairs are amenable to one form of direct repair or the other, there must be adequate preparation for a graft option of which the RSVG comes most handy. Wound infection was the most frequent post-operative complication. The Revascularization rate was satisfactory. However, long term outcome could not be documented because of the poor follow-up record of the patients. References
Copyright © 2011 - African Health Science The following images related to this document are available:Photo images[hs11089t2.jpg] [hs11089t1.jpg] |
| |||||||||

{kind=link}
{kind=link}