 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
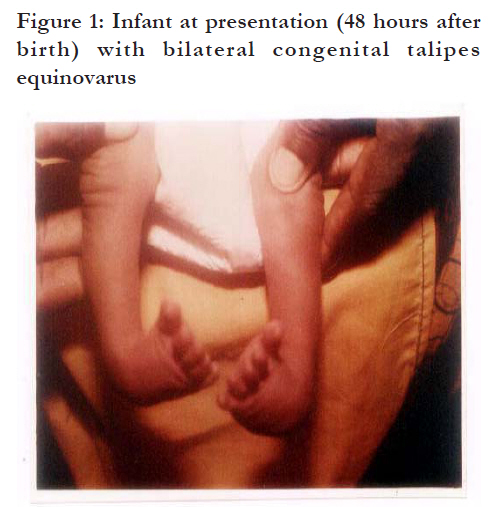
African Health Sciences, Vol. 11, No. 3, Sept, 2011, pp.444 - 448 Case Reports Physiotherapy management of an infant with Bilateral Congenital Talipes Equino varus *Ezeukwu AO1, 2Maduagwu SM 1 Department of Medical Rehabilitation, College of Medicine, University of Nigeria, Enugu Campus, 2 Department of Physiotherapy, University of Maiduguri Teaching Hospital, Maiduguri Code Number: hs11091 Abstract Background: Clinicians are constantly seeking for the most ideal option in the management of Congenital Talipes Equino Varus (CTEV), especially among infants. Keywords: Physiotherapy, talipes equinovarus, passive stretching, strapping. Introduction Congenital ClubFoot (CCF), otherwise known as Congenital Talipes Equino Varus (CTEV) is one of the commonest deformities occurring at the region of the ankle, subtaloid and mid-tarsal joints1. Talipes equino varus is a derivative from Latin: talus (ankle) and pes (foot); equinus (horse-like), that is, the heel in plantar flexion and varus-inverted and adducted2. Hence the deformity comprises of three elements visa-viz: Inversion (twisting inward) of the foot, adduction (inward deviation) of the forefoot relative to the hindfoot and equinus (plantar flexion) 3. Historically, talipes equino varus was recognized and documented since the time of the ancient Egyptians2,4. According to Strach5, Smith and Waren in 1924 found that Pharaoh Siptah of the XIX dynasty was afflicted with clubfoot. Hippocrates introduced talipes equinovarus into the medical literature in 400 BC5, 6. The incidence of CCF varies widely with race and sex. World wide, it is estimated at 1 to 2 per 1,000 live births7,8. In the United States the incidence is about 2.29 per 1,000 live births, 1.6 per 1000 live births in Caucasians and 0.57 per 1,000 in Orientals9. All populations show a consistency of 2: 1 male predominance, with about 50% of cases being bilateral4,6. In unilateral cases, right side affectation dominates10. A positive family history has been connected to high incidence6, 11. According to Strach5 ,Hippocrates had suggested that the treatment of CTEV should start as soon as possible after birth with repeated manipulation and fixations by strong bandages which should be maintained for a long time to achieve over correction. This sage’s teaching principles of treatment are as valid as they were over 2,300 years ago2. Presently management of CTEV is fraught with controversy hence there is no consensus as to the best treatment for this deformity12. In Nigeria, most parents/guardians remain unconvinced on why they should allow surgical procedures for their child. Sometimes they prefer to wait until when the child is old enough before management can commence. In view of this, this study presents a case report of a 2-day old baby boy with congenital talipes equinovarus managed conservatively using physical therapy. Case report A 2-day old baby boy (who weighed 3.2kg at birth) with talipes equinovarus was referred by an orthopaedic surgeon to the Physiotherapy clinic. The baby was delivered at full term, by spontaneous vaginal delivery (SVD) in a missionary hospital. On examination, the baby was found to have bilateral congenital talipes equinovarus [Figure - 1]. Both feet were noticed to turn inwards with the soles directed medially, giving a bow string appearance at both ankle regions. The right foot was observed to be more affected than the left. The characteristics features of CTEV, that is, a three dimensional deformity (inversion, adduction and equinus) with four components (C.A.V.E) were evident in both feet visa viz: C – Cavus (increased longitudinal arch of the feet) On passive movement, there was relative tightness of the tendoachilles on both ankles (the right more than the left); the talocrural, the subtaloid and the mid-tarsal joints were stiff. Every other part of the musculoskeletal system was clinically normal [Figure - 1]. Physiotherapy management The goal of management of the baby consisted of short term and long term goals. The short term goal was to correct the deformity so that the ankles assume plantigrade position by the time the baby would be three months old. The long term goal was to maintain the corrected ankle in situ and follow up the maintained correction until the baby starts walking and if feasible further follow up to avoid relapse. Means of management
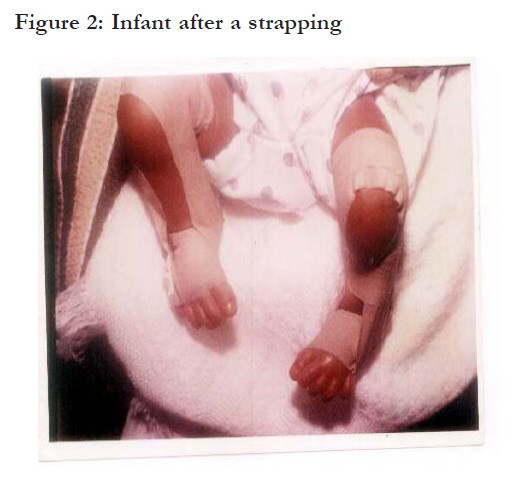
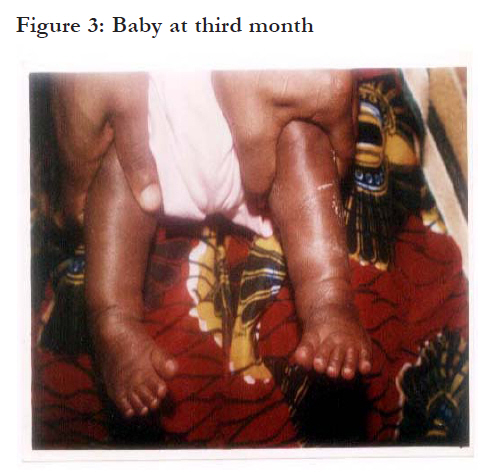
Rhythmic and repeated gentle manipulation The right foot which was more affected was first attended to. Before commencing the procedure, the right knee was placed at 90o flexion to prevent damage to the lower end of tibial and fibular epiphyses, and the knee joint. Thereafter the soft tissues of the right foot were passively stretched as follows: the forefoot was uncurled so that it moved away from the ipsilateral heel (that is forefoot abduction). This manoeuvre was to correct adduction. Then the foot was turned such that the sole faced outward (that is eversion), in an attempt to correct the inverted foot. Finally, to correct the equinus (plantar flexion deformity), the heel was cupped with the right hand from the front of the foot and an upward pressure was applied to it bringing the forefoot upward. This brought the ankle into dorsiflexion. Each of the above manipulation lasted for about two minutes and the entire procedure was repeated four times. The baby was allowed to rest for about 20 minutes while the mother breast fed him. Then the same manoeuvre and procedure were performed on the left. To maintain the feet in the corrected position, strapping was commenced. Materials needed for the strapping were: a 2.5cm width adhesive zinc oxide plaster, cotton wool, tincture of benzoin compound (TBC), methylated spirit and a pair of scissors. Before strapping commenced, skin toileting was religiously observed as follows: the hands were washed with medicated soap and distilled water, then dried with sterilized towel. Finger nails were always cut and kept clean. One of the authors stabilized the baby’s limb and the other carried out the procedure. Cotton wool soaked in methylated spirit was used to clean the right lower limb from the lower 1/3 of the thigh to the toes to avoid sepsis. Thereafter tincture of benzoin compound (TBC) was applied to prevent skin excoriation and improve the adherence of the plaster so that hairs would not stick to the straps. Scissors was used to cut the 2.5cm width zinc oxide plaster into four strips of appropriate lengths. Strapping began by holding the manipulated right foot to over corrected position. The first strip was applied from the medial border of the midpoint of the right leg down under the ipsilateral heel then along the lateral border of the leg to the lower 1/3 of the thigh with knee flexed at 90o. This was to correct the heel varus deformity. The second strip was applied over the dorsum of the mid-foot from lateral to medial then under the sole back to the lateral border of the mid-foot then along the border of the leg over the lower 1/3 of the thigh with knee still at 90o. This was important to correct the varus and equinus deformities by eversion of the foot and abduction of the forefoot. To bring the ankle into dorsiflexed position, the third strip was applied over the dorsum of the forefoot from lateral to medial, then along the plantar surface of the forefoot to the lateral border of the leg over the lower 1/3 of the thigh. The last strip was applied circumferentially around the leg at a point 2cm above the ankle joint. This was to correct the bow string appearance of the lower 1/3 of the leg, the ankle and the foot, and to increase eversion. The baby rested, then the left foot underwent the same process [Figure - 2]. At the end of the procedure the mother was asked to wait for 30 minutes while breastfeeding the baby. This was to observe for any compromise to circulation. For the first six weeks the baby was seen thrice a week and strapping applied twice per week. From the period the baby was 7 to 12 weeks, he was being seen two times in a week and the strapping was done once per week. At three months there was marked improvement, especially on the left foot [Figure - 3]. By this period (that is when the baby was three months), the strapping was no more effective because he was kicking vigorously with the lower limbs. It was then replaced with a full leg plaster of Paris (POP) with the knees at 90o of flexion. The plaster was changed weekly for the first eight weeks of application and the knees and feet mobilized on each occasion. Thereafter it was applied and changed forth-nightly for another eight weeks. The plaster was finally removed when the baby was exactly seven months. At eight months and three weeks he started standing with support and good plantigrade position. At the thirteenth month the baby could walk with good heel strike. The child is now three years without any obvious residual deformity, he is in nursery school and doing very well. Education and instructions to the mother The mother was assured and reassured that with her co-operation, consistency and compliance to treatment the deformity would be corrected. She was made to understand that the correction should be gradual and that we would follow up the case beyond when the baby starts walking. She was taught how to mobilize the feet in the absence of strap. She was instructed anytime a fresh strapping or plaster was applied to observe at frequent intervals any unusual crying by the baby, swollen or bluish colouration of the toes and report to the accident and emergency unit of our hospital. She was also advised to endeavour as much as possible to prevent the strapping or plaster from being wet or soiled either by water or any other fluid such as urine or faeces. Precautions taken during the application of the strapping and plaster Moderate pressure was used to apply the straps and later the plaster, in order to maintain and preserve circulation; A layer of cotton wool (the rolled type in layers), enough to cover the malleoli was applied at medial and lateral malleoli of both ankles to avert pressure sore; Where the strips of the straps were circumferentially applied, in between spaces were avoided to prevent window oedema; The strips of the straps were smoothly applied and no wrinkles were permitted, to prevent skin excoriation. Discussion The choice of techniques for management of CTEV in infants has historically provoked much debate. Recently, there is a swing towards conservative management15, 16, possibly because the results of surgical procedures are unpredictable17. Also there is no consensus on what the standard or most appropriate conservative method should be18. Various conservative techniques such as Kite method19, Ponseti technique13 and the French method14 have been tried and have shown to have varying degrees of success. However, when CTEV proves stubborn to conservative management, then surgical procedures become the option. Clinical decisions are usually impeded by a lack of adequate and convincing long-term reviews of treatment based on prospective assessment and unbiased comparisons of different techniques. This case report showed the outcome of Physical therapy approach for the management of an infant who presented with CTEV. Management in this case report involved a combination of passive stretching and manipulation, strapping technique, Plaster of Paris casting and education of the guardian. Unlike the Ponseti technique and kite methods the researchers opted to commence treatment with Zinc oxide strapping similar to the use of adhesive taping technique of the French method. Although it is usually recommended that serial plaster casting be the first direction of conservative treatment after manipulation 17, the researchers argued that the use of zinc oxide strapping could also be as much effective up till the point when the child starts kicking. The outcome showed that after treatment and at follow up a year later the child showed no sign of the initial presenting pathology. Until recently, treatment consisted of forcible serial manipulations under anaesthesias followed by casting. More recently, authors20,21,22 have advocated the use of serial casting with minimal force (not requiring anesthesia) and have emphasized its importance and potential for success of non-operative treatment. The case report presented employed this and shows that there can be remarkable success if serial POP casting is properly and timely applied. In this case report POP was applied when the application of adhesive tapping outlived it usefulness. Another major factor for the success of the method is the early commencement of treatments and subsequent cooperation from the guardian to bring the child for treatments. Thus, the importance of sufficient and persistent education is essential on the part of the physiotherapist. It has been reported23 that one of the most common reasons for failure is that patients are not referred on time and this affects the outcome of the treatments. Although there is no universally accepted method of assessing outcome in CTEV24 the central aim of physical therapy is to restore the patient to the maximum functional ability in the use of the lower limb especially the foot. Early commencement of physical therapy, proper education and an individualized plan of treatment are essential aspect of this care. This is vital because at this stage there is an enormous potential for remodeling of the tissues through peripheral manipulative therapy techniques if appropriately applied. This is also important as most guardians in Nigeria will not want their wards to undergo surgical procedures at a very early stage of development even when it is medically advisable. Conclusion This study presents a patient with Congenital Talipes Equino Varus successfully managed by Physical Therapy approach. This case report indicates that management of Congenital Talipes Equino Varus if commenced early after birth could help in achieving good recovery and reduce cost of treatment while ameliorating the psychological burden on both the caregiver and patient’s parents. Acknowledgements The authors wish to thank Ms S Oluwaseun Ogunmakin-Kubeyinje and Mr Vitus Eze for their assistance. References
African Health Sciences Vol 11 No 3 September2011 The following images related to this document are available:Photo images[hs11091f2.jpg] [hs11091f1.jpg] [hs11091f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}